KEY POINTS
The risk of nosocomial pneumonia is considerably higher in the subset of ICU patients treated with mechanical ventilation, with an incremental risk of about 1% per day of ventilation.
Ventilator-associated pneumonia (VAP) is associated with mortality in excess of that caused by the underlying disease alone, particularly in case of infection due to high-risk pathogens, such as Pseudomonas aeruginosa and Acinetobacter spp and when initial antibiotic therapy is inappropriate.
The predominant organisms responsible for infection are Staphylococcus aureus, P. aeruginosa, and Enterobacteriaceae, but etiologic agents differ widely according to the population of hospital patients, duration of hospital stay, and prior antimicrobial therapy.
Although appropriate antibiotics may improve survival in patients with VAP, use of empirical broad-spectrum antibiotics in patients without infection is potentially harmful, facilitating colonization and superinfection with multiresistant microorganisms. Any strategy designed to evaluate patients suspected of having developed VAP therefore should be able to withhold antimicrobial treatment in patients without pneumonia.
Because even a few doses of a new antimicrobial agent can negate results of microbiologic cultures, pulmonary secretions in patients suspected of having developed VAP always should be obtained before new antibiotics are administered.
Quantitative techniques, when performed before introduction of new antibiotics, enable physicians to identify most patients who need immediate treatment and help to select optimal therapy in a manner that is safe and well tolerated.
Empirical treatment of patients with VAP should be selected based on available epidemiologic characteristics, information provided by direct examination of pulmonary secretions, intrinsic antibacterial activities of antimicrobial agents, and their pharmacokinetic characteristics.
Once the microbiologic data become available, antimicrobial therapy should be reevaluated in order to avoid prolonged use of a broader spectrum of antibiotic therapy than is justified by the available information. For many patients, including those with late-onset infection, the culture data will not show the presence of highly resistant pathogens, and in these individuals, therapy can be narrowed or even reduced to a single agent in light of the susceptibility pattern of the causative pathogens without risking inappropriate treatment.
Some very simple, no-cost measures, such as avoiding nasal insertion of endotracheal and gastric tubes, maintaining the endotracheal tube cuff pressure above 20 cm H2O to prevent leakage of bacteria around the cuff into the lower respiratory tract, removal of ventilator tubing condensates with minimal exposure to patients, placement of ventilated patients in a semirecumbent position when enteral nutrition is used, providing adequate oral hygiene with an antiseptic such as chlorhexidine, as well as avoiding unnecessary sedation, may have an impact on the frequency of VAP.
Ventilator-associated pneumonia (VAP) remains a major cause of mortality and morbidity despite the introduction of potent broad-spectrum antimicrobial agents, major advances in the management of ventilator-dependent patients admitted to ICUs, and the use of preventive measures, including the routine use of effective procedures to disinfect respiratory equipment. Rates of pneumonia are considerably higher among patients hospitalized in ICUs compared with those in hospital wards, and the risk of pneumonia is increased three- to tenfold for the intubated patient on mechanical ventilation (MV).1-8 In contrast to infections of more frequently involved organs (eg, urinary tract and skin), for which mortality is low, ranging from 1% to 4%, the mortality rate for VAP, defined as pneumonia occurring more than 48 hours after endotracheal intubation and initiation of MV, ranges from 20% to 50% and can reach >70% in some specific settings or when lung infection is caused by high-risk pathogens.2,9-14 Because several studies have shown that appropriate antimicrobial treatment of patients with VAP significantly improves outcome, more rapid identification of infected patients and accurate selection of antimicrobial agents represent important clinical goals.2,9-16 However, consensus on appropriate diagnostic, therapeutic, and preventive strategies for VAP has yet to be reached.
EPIDEMIOLOGY
Accurate data on the epidemiology of VAP are limited by the lack of standardized criteria for its diagnosis. Conceptually, VAP is defined as an inflammation of the lung parenchyma caused by infectious agents not present or incubating at the time MV was started. Despite the clarity of this conception, the past three decades have witnessed the appearance of numerous operational definitions, none of which is universally accepted. Even definitions based on histopathologic findings at autopsy may fail to find consensus or provide certainty. Pneumonia in focal areas of a lobe may be missed, microbiologic studies may be negative despite the presence of inflammation in the lung, and pathologists may disagree on the findings.17-20 The absence of a “gold standard” continues to fuel controversy about the adequacy and relevance of many studies in this field. Prolonged (>48 hours) MV is the most important factor associated with nosocomial pneumonia. However, VAP may occur within the first 48 hours following intubation. Since the seminal study by Langer and colleagues, it is usual to distinguish early-onset VAP, which occurs during the first 4 days of MV, from late-onset VAP, which develops 5 days or more after initiation of MV.21 Not only are the causative pathogens commonly different, but the disease also is usually less severe and the prognosis better in early-onset than late-onset VAP.1,3
The exact incidence varies widely depending on the case definition of pneumonia and the population being evaluated.22-27 All studies, however, have confirmed that nosocomial pneumonia is considerably more frequent in ventilated patients than in other ICU patients, with an incidence increasing by as much as 6- to 20-fold in this subset of patients.6,28 VAP occurs in 9% to 27% of all intubated patients and its incidence increases with duration of ventilation.26,29 The risk of VAP is highest early in the course of hospital stay, and is estimated to be 3% per day during the first 5 days of ventilation, 2% per day during days 5 to 10 of ventilation, and 1% per day after this.29 Because most mechanical ventilation is short term, approximately half of all episodes of VAP occur within the first 4 days of mechanical ventilation.
In a large epidemiological study, independent predictors of VAP retained by multivariable analysis were a primary admitting diagnosis of burns, trauma, central nervous system disease, respiratory disease, cardiac disease, mechanical ventilation during the preceding 24 hours, witnessed aspiration, and use of paralytic agents. Exposure to antibiotics conferred protection, but this effect was attenuated over time.29
According to four studies, the VAP rate was higher in patients with ARDS than other ventilated patients, affecting between 34% and >70% of patients with ARDS and often leading to the development of sepsis, multiple organ failure and death.10,30-32
Mechanically ventilated patients in the ICU with VAP appear to have a two- to tenfold higher risk of death as compared with patients without pneumonia. Although these statistics indicate that VAP can be lethal, previous studies have not demonstrated clearly that pneumonia is responsible for the higher mortality rate of these patients.33 It is often difficult to determine whether ICU patients with severe underlying illness would have survived if VAP had not occurred. VAP, however, has been recognized in several case-controlled studies or studies using multivariate analysis as an important prognostic factor for different groups of critically ill patients.8,33-37
Other factors beyond the simple development of VAP, such as the severity of the disease, the responsible pathogens or the appropriateness of initial treatment, may be more important determinants of outcome for patients in whom pneumonia develops.38 Indeed, it may be that VAP increases mortality only in the subset of patients with intermediate severity of illness,37 when initial treatment is inappropriate,13,15,39-44 and/or in patients with VAP caused by high-risk pathogens, such as P. aeruginosa.38,45 Patients with very low severity and early-onset pneumonia caused by organisms such as Haemophilus influenzae or Streptococcus pneumoniae have excellent prognoses with or without VAP, whereas very ill patients with late-onset VAP occurring while they are in a quasi-terminal state would be unlikely to survive. Using a multistate progressive disability model that appropriately handled VAP as a time-dependent event in a high-quality database of 2873 mechanically ventilated patients, Nguile-Makao et al recently showed that VAP attributable mortality was 8.1% overall, varying widely with case-mix, severity at admission, time to VAP onset, and severity of organ dysfunction at VAP onset.38 These results are consistent with the 10.6% value obtained in five German ICUs using also a multistate progressive disability model and other studies having used similar methodology for determining attributable mortality.46,47
It is impossible to evaluate precisely the morbidity and excess costs associated with VAP. All studies, however, have shown clearly that patients with VAP have prolonged duration of mechanical ventilation and lengthened ICU and hospital stay as compared with patients who do not have VAP.1,3,48,49 Summarizing available data, VAP appears to extend the ICU stay by at least 4 to 6 days, with the attributable ICU length of stay being longer for medical than surgical patients and for patients infected with “high-risk” as opposed to “low-risk” organisms.50 The prolonged hospitalization of patients with VAP underscores the considerable financial burden imposed on the health care system by the development of VAP.26,48,49,51-55
Microorganisms responsible for VAP differ according to the population of ICU patients, the durations of hospital and ICU stays, and the specific diagnostic method(s) used to establish the responsible pathogens. A number of studies have shown that gram-negative bacilli (GNB) cause many of the respiratory infections in this setting.1,3,56,57 The data from 24 studies conducted on ventilated patients, for whom bacteriologic studies were restricted to uncontaminated specimens obtained using a protected specimen brush (PSB) or bronchoalveolar lavage (BAL), confirmed these results: GNB represented 58% of recovered organisms (Table 59-1).3 The predominant GNB were P. aeruginosa and Acinetobacter spp, followed by Proteus spp, Escherichia coli, Klebsiella spp, and H. influenzae. A relatively high rate of gram-positive pneumonias was also reported in those studies, with S. aureus involved in >20% of the cases.56 Many episodes of VAP are caused by multiple pathogens.3,58
Etiology of VAP as Documented by Bronchoscopic Techniques in 24 Studies for a Total of 1689 Episodes and 2490 Pathogens
| Pathogen | Frequency (%) |
|---|---|
| Pseudomonas aeruginosa | 24.4 |
| Acinetobacter spp | 7.9 |
| Stenotrophomonas maltophilia | 1.7 |
| Enterobacteriaceaea | 14.1 |
| Haemophilus spp | 9.8 |
| Staphylococcus aureusb | 20.4 |
| Streptococcus spp | 8.0 |
| Streptococcus pneumoniae | 4.1 |
| Coagulase-negative staphylococci | 1.4 |
| Neisseria spp | 2.6 |
| Anaerobes | 0.9 |
| Fungi | 0.9 |
| Others (<1% each)c | 3.8 |
Underlying diseases may predispose patients to infection with specific organisms. Patients with chronic obstructive pulmonary disease (COPD) are at increased risk for H. influenzae, Moraxella catarrhalis, or S. pneumoniae infections; cystic fibrosis increases the risk of P. aeruginosa and/or S. aureus infections, while trauma and neurological disease increases the risk for S. aureus infection. Furthermore, the causative agent for pneumonia differs among ICU surgical populations, with 18% of the nosocomial pneumonias caused by Haemophilus or pneumococci, particularly in patients with trauma, but not in patients with malignancy, transplantation, abdominal or cardiovascular surgery.1,3
Despite somewhat different definitions of early-onset pneumonia, varying from onset of less than 3 to less than 7 days, high rates of H. influenzae, S. pneumoniae, MSSA or susceptible Enterobacteriaceae were constantly found in early-onset VAP, whereas P. aeruginosa, Acinetobacter spp, MRSA and multiresistant GNB were significantly more frequent in late-onset VAP.3 The different pattern of distribution of etiologic agents between early- and late-onset VAP is linked to prior antimicrobial therapy in many patients with late-onset VAP. When multivariate analysis was used to identify risk factors for VAP caused by potentially drug-resistant bacteria such as MRSA, P. aeruginosa, Acinetobacter baumannii, and/or S. maltophilia in 135 consecutive episodes of VAP, only three variables remained significant: duration of mechanical ventilation of longer than 7 days before onset of VAP, prior antibiotic use, and prior use of broad-spectrum drugs (third-generation cephalosporins, fluoroquinolones and/or imipenem).59 Not all studies have confirmed this distribution pattern, and in some studies the most common pathogens associated with early-onset VAP were P. aeruginosa, MRSA and Enterobacter spp, with similar pathogens associated with late-onset VAP.60,61 These findings might be explained in part by prior hospitalization and the use of antibiotics before transfer to the ICU.
The incidence of multiresistant pathogens is also closely linked to local factors and varies widely from one institution to another. Consequently, each ICU has to continuously collect meticulous epidemiologic data.62 Clinicians clearly must be aware of the common microorganisms associated with both early-onset and late-onset VAP in their own hospitals in order to avoid the administration of initial inadequate antimicrobial therapy.
Legionella species, anaerobes, and even Pneumocystis jirovecii should be mentioned as potential causative agents, but these microbes are not commonly found when pneumonia is acquired during mechanical ventilation. Herpesviridae, namely herpes simplex virus (HSV) can be detected in the lower respiratory tracts of 5% to 64% of ICU patients, depending on the population and the diagnostic method used. In most cases, HSV recovery from lower respiratory tract samples of nonimmunocompromised ventilated patients corresponds to viral contamination from the mouth and/or throat. For some patients, however, real HSV bronchopneumonitis can develop and it can evolve into ARDS and/or facilitate the occurrence of bacterial superinfection.63-65 Cytomegalovirus-induced pneumonia is a rare event in ventilated patients. As for HSV bronchopneumonitis, it is impossible to know whether CMV detection in the lower respiratory tract is merely a marker of disease severity or signals real disease with its own morbidity and mortality.66-69
Isolation of fungi, most frequently Candida species, at significant concentrations poses interpretative problems. Invasive disease has been reported in VAP but yeasts are isolated more frequently from respiratory tract specimens in the absence of apparent disease, even when retrieved at high concentrations from bronchoscopic specimens.70-74 Thus, based on current data, the presence of yeasts in respiratory secretions obtained from non-immunosuppressed ventilated patients usually indicates colonization rather than infection of the respiratory tract, and does not justify by itself a specific antifungal therapy. Evidence of lung tissue invasion is needed for making the diagnosis of Candida pneumonia in such a setting. Interactions, however, between Candida and bacteria, particularly Pseudomonas, have been reported, and colonization of the respiratory tract by yeasts may predispose to bacterial VAP.75-78
By examining currently available data, the clinical significance of anaerobes in the pathogenesis and outcome of VAP remains unclear except as etiologic agents in patients with necrotizing pneumonitis, lung abscess or pleuropulmonary infections. Anaerobic infection and coverage with antibiotics, such as clindamycin or metronidazole, should probably also be considered for patients with respiratory secretions documenting numerous extra- and intracellular microorganisms after Gram staining in the absence of positive cultures for aerobic pathogens.
PREDISPOSING FACTORS
Risk factors provide information on the probability of lung infection developing in individuals and populations. Thus, they may contribute to the elaboration of effective preventive strategies by indicating which patients might be most likely to benefit from prophylaxis against pneumonia. Independent factors for VAP that were identified by multivariate analyses in selected studies are summarized in Table 59-2.2,11,13,14,29,51,79-83
Independent Factors for VAP Identified by Multivariate Analysis in Selected Studies
| Host Factors | Intervention Factors | Other |
|---|---|---|
| Serum albumin <2.2 g/dL | H2 blockers ± antacids | Season |
| Age ≥60 years | Paralytic agents, continuous intravenous sedation | |
| ARDS | >4 units of blood products | |
| COPD, pulmonary disease | Intracranial pressure monitoring | |
| Coma or impaired consciousness | MV >2 days | |
| Burns, trauma | Positive end-expiratory pressure | |
| Organ failure | Frequent ventilator circuit changes | |
| Severity of illness | Reintubation | |
| Large-volume gastric aspiration | Nasogastric tube | |
| Gastric colonization and pH | Supine head position | |
| Upper respiratory tract colonization | Transport out of the ICU | |
| Sinusitis | Prior antibiotic or no antibiotic therapy |
Postsurgical patients are at increased risk for VAP. In a 1981 report, the pneumonia rate during the postoperative period was 17%.84 Those authors stated that the development of pneumonia was closely associated with preoperative markers of severity of the underlying disease, such as low serum albumin concentration and a high score on the American Society of Anesthesiologists preanesthesia physical status classification. A history of smoking, longer preoperative stays, longer surgical procedures and thoracic or upper abdominal surgery were also significant risk factors for postsurgical pneumonia. Another study comparing adult ICU populations demonstrated that postoperative patients had consistently higher rates of nosocomial pneumonia than did medical ICU patients, with a risk ratio of 2.2.82 Multiple regression analysis was performed to identify independent predictors of nosocomial pneumonia in the two groups; for surgical ICU patients, mechanical ventilation (>2 days) and acute physiology and chronic health evaluation score (APACHE) were retained by the model; for the medical ICU population, only mechanical ventilation (>2 days) remained significant. It has been suggested that different surgical ICU patient populations may have different risks for nosocomial pneumonia: cardiothoracic surgery and trauma (particularly the head) patients were more likely to develop VAP than medical or other types of surgical patients.29
The use of antibiotics in the hospital setting has been associated with an increased risk of nosocomial pneumonia and selection of resistant pathogens.13,36,59,85-89 In a cohort study of 320 patients, prior antibiotic administration was identified by logistic regression analysis to be one of the four variables independently associated with VAP along with organ failure, age >60 years, and the patient’s head positioning (ie, flat on his back or supine vs head and thorax raised 30°-40° or semirecumbent).36 Other investigators, however, found that antibiotic administration during the first 8 days was associated with a lower risk of early-onset VAP.90 For example, Sirvent et al showed that a single dose of a first-generation cephalosporin given prophylactically was associated with a lower rate of early-onset VAP in patients with structural coma.91 Moreover, multiple logistic regression analysis of risk factors for VAP in 358 medical ICU patients identified the absence of antimicrobial therapy as one of the factors independently associated with VAP onset.92 Finally, the results of the multicenter Canadian study on the incidence of and risk factors for VAP indicated that antibiotic treatment conferred protection against VAP.29 This apparent protective effect of antibiotics disappears after 2 to 3 weeks, suggesting that a higher risk of VAP cannot be excluded beyond this point.
Prolonged antibiotic administration to ICU patients for primary infection is thought to favor selection and subsequent colonization with resistant pathogens responsible for superinfections.12,59,88,93-95 According to our data on 567 ventilated patients, those who had received antimicrobial therapy within the 15 days preceding lung infection were not at higher risk for development of VAP, but 65% of the lung infections that occurred in patients who had received broad-spectrum antimicrobial drugs versus only 19% of those developing in patients who had not received antibiotics were caused by Pseudomonas or Acinetobacter spp.12,59,88,93-95 In a 1988 investigation on mechanically ventilated baboons treated with a variety of regimens of intravenous and topical antibiotics or no antibiotics at all polymicrobial pneumonia occurred in almost all untreated animals.95,96 However, baboons that had received prophylactic topical polymycin had only a slightly lower incidence of pneumonia, and the prevalence of drug-resistant microorganisms in the tracheal secretions was very high: 60% and 78% after 4 and 8 days of MV, respectively. Therefore, strong arguments suggest that the prophylactic use of antibiotics in the ICU increases the risk of superinfection with multiresistant pathogens while only delaying the occurrence of nosocomial infection.
In theory, patients receiving stress-ulcer prophylaxis that does not change gastric acidity, such as sucralfate, should have lower rates of gastric bacterial colonization and, consequently, a lower risk for nosocomial pneumonia, than those receiving antacids or H2-blockers.97,98
According to meta-analyses of the efficacy of stress-ulcer prophylaxis in ICU patients, respiratory tract infections were significantly less frequent in patients treated with sucralfate than those receiving antacids or H2-blockers.99,100 This conclusion, however, was not fully confirmed in a very large, multicenter, randomized, blinded, placebo-controlled trial that compared sucralfate suspension (1 g every 6 hours) with the H2-receptor antagonist ranitidine (50 mg every 8 hours) for the prevention of upper gastrointestinal bleeding in 1200 ventilated patients.101 Clinically relevant gastrointestinal bleeding developed in 10 of the 596 (1.7%) patients receiving ranitidine, as compared with 23 of the 604 (3.8%) receiving sucralfate (relative risk [RR], 0.44; 95% confidence interval [CI], 0.21-0.92; p = 0.02). In the ranitidine group, 114 of 596 (19.1%) patients had VAP, as diagnosed by an adjudication committee using a modified version of the CDC criteria, versus 98 of 604 (16.2%) in the sucralfate group (RR, 1.18; 95% CI, 0.92-1.51; p = 0.19). VAP, however, occurred significantly less frequently in patients receiving sucralfate when the diagnosis of pneumonia was based on Memphis VAP Consensus Conference criteria (if there was radiographic evidence of abscess and a positive needle aspirate, or histologic proof of pneumonia at biopsy or autopsy) (p = 0.03).101
Sucralfate appears to have a small protective effect against VAP because stress-ulcer prophylactic medications that raise the gastric pH might themselves increase the incidence of pneumonia.102,103 This contention is supported by direct comparisons of trials of H2-receptor antagonists versus no prophylaxis, which showed a trend toward higher pneumonia rates among the patients receiving H2-receptor antagonists (OR, 1.25; 95% CI, 0.78-2.00).99 Furthermore, the comparative effects of sucralfate and no prophylaxis are unclear. Among 226 patients enrolled in two randomized trials, those receiving sucralfate tended to develop pneumonia more frequently than those given no prophylaxis (OR, 2.11; 95% CI, 0.82-5.44).104,105
The presence of an endotracheal tube by itself circumvents host defenses, causes local trauma and inflammation, and increases the probability of aspiration of nosocomial pathogens from the oropharynx around the cuff. Scanning electron microscopy of 25 endotracheal tubes revealed that 96% had partial bacterial colonization and 84% were completely coated with bacteria in a biofilm or glycocalyx.106 The authors hypothesized that bacterial aggregates in biofilm dislodged during suctioning might not be killed by antibiotics or effectively cleared by host immune defenses. Clearly, the type of endotracheal tube may also influence the likelihood of aspiration. Use of low-volume, high-pressure endotracheal cuffs reduced the rate to 56% and the advent of high-volume, low-pressure cuffs further lowered it to 20%.107 Leakage around the cuff allows secretions pooled above the cuff to enter the trachea; this mechanism, recently confirmed, underlines the importance of maintaining adequate intracuff pressure for preventing VAP.108
In addition to the presence of endotracheal tubes, reintubation is, per se, a risk factor for VAP.109 This finding probably reflects an increased risk of aspiration of colonized oropharyngeal secretions into the lower airways by patients with subglottic dysfunction or impaired consciousness after several days of intubation. Another explanation is direct aspiration of gastric contents into the lower airways, particularly when a nasogastric tube is kept in place after extubation.
Some investigators postulated that early tracheotomy could lower VAP rate because it can permit easier oral hygiene and bronchopulmonary toilet or less time spent deeply sedated.110 Such benefit, however, was not confirmed in other studies, including two large recent randomized trials having systematically evaluated this issue.111-114
Almost all ventilated patients have a nasogastric tube inserted to evacuate gastric and enteral secretions, prevent gastric distention, and/or provide nutritional support. The nasogastric tube is not generally considered to be a potential risk factor for VAP, but it may increase oropharyngeal colonization, cause stagnation of oropharyngeal secretions, and increase reflux and the risk of aspiration. A multivariate analysis retained the presence of a nasogastric tube as one of the three independent risk factors for nosocomial pneumonia based on a series of 203 patients admitted to the ICU for 72 hours or more.80
Early initiation of enteral feeding is generally regarded as beneficial in critically ill patients, but it may increase the risk of gastric colonization, gastroesophageal reflux, aspiration and pneumonia.115,116 The aspiration rate generally varies as a function of differences in the patient population, neurological function, type of feeding tube, location of the feeding port and method of evaluating aspiration. Clinical impressions and preliminary data suggest that postpyloric or jejunal feeding entails less risk of aspiration and may therefore be associated with fewer infectious complications than gastric feeding, although this point remains controversial.117,118 Nonetheless, aspiration can easily occur should the feeding tube be inadvertently dislodged. A retrospective study of noncritically ill adult patients showed a 40% rate of accidental feeding-tube dislodgment, but all the patients whose tube was dislodged were confused, disoriented or had altered awareness, as is frequently observed in ICU patients.119
Maintaining ventilated patients with a nasogastric tube in place in a supine position is also a risk factor for aspiration of gastric contents into the lower airways. When radioactive material was injected through a nasogastric tube directly into the stomach of 19 ventilated patients, the mean radioactive counts in endobronchial secretions were higher in a time-dependent fashion in samples obtained from patients in a supine position than in those obtained from patients in a semirecumbent position.120 The same microorganisms were isolated from the stomach, pharynx and endobronchial samples of 32% of the specimens taken while patients were lying supine. The same investigators conducted a randomized trial comparing semirecumbent and supine positions.121 The trial, which included 86 intubated and ventilated patients, was stopped after the planned interim analysis because the frequency and the risk of VAP were significantly lower for the semirecumbent group. These findings were indirectly confirmed by the demonstration that the head position of the supine patient during the first 24 hours of mechanical ventilation was an independent risk factor for acquiring VAP.36 However, to what degree of elevation the head of bed should be targeted remains controversial.122-125 Van Nieuwenhoven and colleagues randomized 221 patients to be placed either in the semirecumbent position or supine, but not completely flat. In that study, microbiologically confirmed as well as clinically diagnosed VAP were not different between the groups. Importantly, the feasibility of the 45° elevation of the head was also challenged by the authors, who were unable to maintain this position in their patients despite constant monitoring of bed position.125 The inconsistency in the efficacy of the semirecumbent position on VAP prevention was confirmed by a recent meta-analysis that pooled data from all randomized trials and did not find a significant reduction of clinically or microbiologically diagnosed VAP.126
Ventilators with humidifying cascades often have high levels of tubing colonization and condensate formation that may also be risk factors for pneumonia. The rate of condensate formation in the ventilator circuit is linked to the temperature difference between the inspiratory-phase gas and the ambient temperature, and may be as high as 20 to 40 mL/h.127,128 Examination of condensate colonization in 20 circuits detected a median level of 2.0 × 105 organisms/mL, and 73% of the 52 gram-negative isolates present in the patients’ sputum samples were subsequently isolated from condensates.128 Because most of the tubing colonization was derived from the patients’ secretions, the highest bacterial counts were present near the endotracheal tube. Simple procedures, such as turning the patient or raising the bed rail, may accidentally spill contaminated condensate directly into the patient’s tracheobronchial tree.129 Inoculation of large amounts of fluid with high bacterial concentrations is an excellent way to overwhelm pulmonary defense mechanisms and cause pneumonia. Heating ventilator tubing markedly lowers the rate of condensate formation, but heated circuits are often nondisposable and are expensive. In-line devices with one-way valves to collect the condensate are probably the easiest way to handle this problem; they must be correctly positioned into disposable circuits and emptied regularly.
To decrease condensation and moisture accumulation in ventilator circuits, several studies have investigated the use of heat-moisture exchangers (HME) in place of conventional heated-water humidification systems. Slightly lower VAP rates were observed in four studies and a significant difference in a fifth study, suggesting that HME are at least comparable to heated humidifiers and may be associated with lower VAP rates than heated humidifiers.130-134 Changing the HME every 48 hours did not affect ventilator-circuit colonization and the authors concluded that the cost of mechanical ventilation might be substantially reduced without any detriment to the patient by prolonging the time between HME changes from 24 to 48 hours.135 Furthermore, using HME may decrease the nurses’ workload (no need to refill cascades, to void water traps on circuits, and so on), decrease the number of septic procedures (it was clearly shown that respiratory tubing condensates must be handled as an infectious waste), and reduce the cost of mechanical ventilation, especially when used for prolonged periods without change. Because some observational studies, however, have documented an increased resistive load and a larger dead space associated with exchangers,136,137 their use should be discouraged in patients with ARDS ventilated with a low tidal volume and in patients with COPD during the weaning period, if pressure support, and not T-piece trials, are used.
There is no apparent advantage to changing ventilator circuits frequently for VAP prevention. This holds true whether circuits are changed every 2 days or every 7 days compared with no change at all, and whether they are changed weekly as opposed to 3 times per week.138-140 A policy of no circuit changes or infrequent circuit changes is simple to implement and the costs are likely lower than those generated by regular, frequent circuit changes; thus, such a policy is strongly recommended by the 1997 CDC guidelines and other guidelines.141-143
While many studies have compared the risk of nosocomial sinusitis as a function of the intubation method used and the associated risk of VAP, only a few were adequately powered to give a clear answer. In one study of 300 patients who required mechanical ventilation for at least 7 days and were randomly assigned to undergo nasotracheal or orotracheal intubation, computed tomographic evidence of sinusitis was observed slightly more frequently in the nasal than oral endotracheal group (p = 0.08), but this difference disappeared when only bacteriologically confirmed sinusitis was considered.144
The rate of infectious maxillary sinusitis and its clinical relevance were also prospectively studied in 162 consecutive critically ill patients, who had been intubated and ventilated for 1 hour to 12 days before enrollment.145 All had a paranasal computed tomography scan within 48 hours of admission which was used to divide them into three groups (no, moderate or severe sinusitis), according to the radiologic appearance of the maxillary sinuses. Patients who had no sinusitis at admission (n = 40) were randomized to receive endotracheal and gastric tubes via the nasal or oral route and, based on radiologic images, respective sinusitis rates were 96% and 23% (p <0.03); yet, no differences in the rates of infectious sinusitis were documented according to the intubation route. VAP, however, was more common in patients with infectious sinusitis, with 67% of them developing lung infection in the days following the diagnosis of sinusitis.145 Therefore, whereas it seems clear that infectious sinusitis is a risk factor for VAP, no studies have yet been able to definitively demonstrate that orotracheal intubation decreases the infectious sinusitis rate compared to nasotracheal intubation. Thus no firm recommendations on the best route of intubation to prevent VAP can be advanced.
A prospective cohort study conducted in 531 ventilated patients evaluated the impact of transporting the patient out of the ICU to other sites within the hospital.146 Results showed that 52% of the patients had to be moved at least once for a total of 993 transports and that 24% of the transported patients developed VAP compared with 4% of the patients confined to the ICU (p <0.001). Multiple logistic regression analysis confirmed that transport out of the ICU was independently associated with VAP (OR = 3.8; p <0.001).
DIAGNOSIS
VAP is typically suspected when a patient has new or progressive radiographic infiltrates and clinical findings suggesting infection, such as the new onset of fever, purulent sputum, leukocytosis, increased minute ventilation, and/or a decline in arterial oxygenation. Because interpretation of chest radiographs is difficult, particularly in patients with prior abnormalities, such as ARDS, it is also mandatory to consider the diagnosis of VAP in ventilated patients who clinically deteriorate, and/or in whom vasopressors should be increased to maintain blood pressure, even in the absence of a clear-cut progression of the radiographic abnormalities.
The systemic signs of infection, however, such as fever, tachycardia and leukocytosis, are nonspecific findings that can be caused by any condition that releases cytokines. In trauma and other surgical patients, fever and leukocytosis should prompt the physician to suspect infection, but during the early posttraumatic or postoperative period (ie, during the first 72 hours), these findings usually are not conclusive. Later, fever and leukocytosis are more likely to be caused by pulmonary or nonpulmonary (vascular catheter infection, gastrointestinal infection, urinary tract infection, sinusitis, or wound infection) infections, but even then, other events associated with an inflammatory response (eg, devascularized tissue, open wounds, pulmonary edema and/or infarction) can be responsible for these findings. Although the plain (usually portable) chest roentgenogram remains an important component in the evaluation of ventilated patients with suspected pneumonia, it is most helpful when it is normal and rules out pneumonia. When infiltrates are evident, the particular pattern is of limited value for differentiating among cardiogenic pulmonary edema, noncardiogenic pulmonary edema, pulmonary contusion, atelectasis (or collapse) and pneumonia, even when using computed tomographic scanning.24,32,147-151 Because the tracheobronchial tree of mechanically ventilated patients is frequently rapidly colonized by potential pathogens, the presence of bacteria at that level is not a sufficient argument to diagnose true lung infection, which constitutes another major obstacle for the diagnosis of VAP.24,152
In 1991, a composite clinical score, the Clinical Pulmonary Infection Score (CPIS) was proposed, based on seven variables (temperature, blood leukocyte count, volume and purulence of tracheal secretions, oxygenation, pulmonary radiography, and semiquantitative culture of tracheal aspirate) accorded 0, 1, or 2 points.153 This scoring system, however, is quite tedious to calculate and difficult to use in clinical practice, because several variables, such as progression of pulmonary infiltrates and results of semiquantitative cultures of tracheal secretions, can lead to different calculations depending on the observer.154 Furthermore, its value was not validated in several subsequent prospective studies, especially in patients with bilateral pulmonary infiltrates.155-163
Thus, as soon as a ventilated patient is suspected of developing pneumonia, a more complete diagnostic work-up should be undertaken, targeting two objectives. The first objective is the immediate recognition of a true VAP or of an extrapulmonary bacterial infection, in order to start effective antibiotics against the microorganisms responsible for infection as soon as possible.1,3 Numerous studies indicate that failure to initiate prompt appropriate antimicrobial treatment in this setting is a major risk factor for an increased morbidity and mortality.164-172 The second one is avoiding overusing antibiotics in patients with only proximal airways colonization and no ongoing bacterial infection. Epidemiologic investigations have clearly demonstrated that indiscriminate use of antimicrobial agents in ICU patients may have immediate and long-term consequences, which contribute to emergence of multiresistant pathogens and increase the risk of serious superinfections.173-178 This risk is not limited to one patient. Instead, the risk of colonization or infection by multidrug-resistant strains is increased in patients throughout the ICU and even the entire hospital. Virtually all reports emphasize that better antibiotic control programs to limit bacterial resistance are urgently needed in ICUs, and that patients without true infection should not receive antimicrobial treatment.173
To reach these objectives, all diagnostic strategies should follow three consecutive steps: (1) obtaining a respiratory tract sample (from proximal or distal airways) for microscopy and culture (qualitative, semiquantitative, or quantitative) before introduction of new antibiotics; (2) immediately starting empiric antimicrobial treatment, unless there are both a negative microscopy and no signs of severe sepsis; and (3) reevaluating treatment on day 2 or 3, based on microbiologic cultures results and clinical outcome.1,3
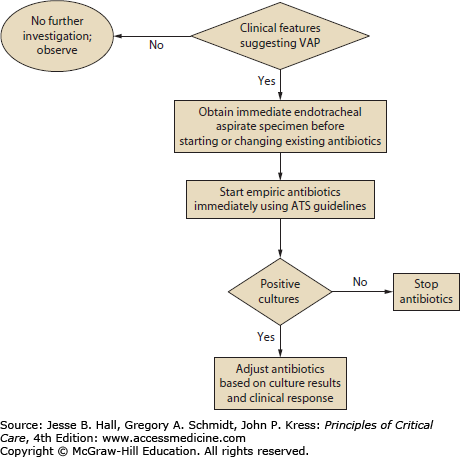
The first option is to use a clinical strategy and to treat every patient clinically suspected of having a pulmonary infection with new antibiotics (even when the likelihood of infection is low), arguing that several studies showed that immediate initiation of appropriate antibiotics was associated with reduced mortality.41,44,166,179-184 Using this strategy, all patients suspected of having VAP are treated with new antibiotics after having obtaining an endotracheal aspirate for microscopy and qualitative culture. The selection of appropriate empirical therapy is based on risk factors and local microbiological and resistance patterns, and involves qualitative testing to identify possible pathogens. The initial antimicrobial therapy is adjusted according to culture results and clinical response (Fig. 59-1). Antimicrobial treatment is discontinued if and only if the following three criteria are fulfilled on day 3: (1) clinical diagnosis of VAP is unlikely (there are no definite infiltrates found on chest radiography at follow-up and no more than one of the three following findings are present: temperature >38.3°C, leukocytosis or leukopenia, and purulent tracheobronchial secretions) or an alternative noninfectious diagnosis is confirmed, (2) tracheobronchial aspirate culture results are nonsignificant, and (3) severe sepsis or shock are not present.185
This clinical approach has two undisputable advantages: first, no specialized microbiologic techniques are required, and, second, the risk of missing a patient who needs antimicrobial treatment is minimal when all suspected patients are treated with new antibiotics. However, because tracheobronchial aspirate culture results are rarely negative secondary to the high rate of proximal airways colonization observed in patients receiving MV, discontinuation of antibiotics on day 3 is difficult to perform, leading to antibiotic overuse in many ICU patients. Qualitative endotracheal aspirate cultures contribute indisputably to the diagnosis of VAP only when they are completely negative for a patient with no modification of prior antimicrobial treatment. In such a case, the negative-predictive value is very high and the probability of the patient having pneumonia is close to zero.18 This is why some investigators have proposed to replace qualitative cultures of endotracheal aspirates by semi- or quantitative cultures of the same specimens.186
Several studies using quantitative culture techniques suggest that endotracheal aspirate cultures may have an acceptable overall diagnostic accuracy, similar to that of several other more invasive techniques.186 Not all studies, however, have confirmed this conclusion. To assess the reliability of that method, bronchoscopy with PSB and BAL was used to study 57 episodes of suspected lung infection in 39 ventilator-dependent patients with no recent changes of antimicrobial therapy.187 The operating characteristics of endotracheal aspirate cultures were calculated over a range of cutoff values (from 103 to 107 cfu/mL); the threshold of 106 cfu/mL appeared to be the most accurate, with a sensitivity of 68% and a specificity of 84%. When this threshold was applied to the study population, however, almost one-third of the patients with pneumonia were not identified. Furthermore, only 40% of microorganisms cultured in endotracheal aspirate samples coincided with those obtained from PSB specimens. Other authors have emphasized that, although quantitative endotracheal aspirate cultures can correctly identify patients with pneumonia, microbiologic results cannot be used to infer which microorganisms present in the trachea are really present in the lungs. In a study comparing quantitative endotracheal aspirate culture results to postmortem quantitative lung-biopsy cultures, only 53% of the microorganisms isolated from the former samples at concentrations >107 cfu/mL were also found in the latter cultures.188
The inherent advantage of quantitative cultures of endotracheal aspirates is that they are more specific, permitting the discontinuation of antibiotics in more patients than when using only qualitative cultures. But it must be kept in mind that this technique has several potential pitfalls. First, many patients may not be identified using the cutoff value of 106 cfu/mL. Second, as soon as a lower threshold is used, specificity declines sharply and overtreatment becomes a problem. Finally, selecting antimicrobial therapy solely on the basis of endotracheal aspirate culture results can lead to either unnecessary antibiotic therapy or overtreatment with broad-spectrum antimicrobial agents.
This strategy uses quantitative cultures of lower respiratory secretions (BAL or PSB collected with a bronchoscope) to define both the presence of pneumonia and the etiologic pathogen(s). Pathogens are present in inflammatory secretions of the lower respiratory tract at concentrations of at least 105 to 106 cfu/mL, whereas contaminants are generally present at less than 104 cfu/mL.189 The diagnostic thresholds proposed for PSB and BAL are based on this concept. Because PSB collects between 0.001 and 0.01 mL of secretions, the presence of greater than 103 bacteria in the originally diluted sample (1 mL) actually represents 105 to 106 cfu/mL of pulmonary secretions. Similarly, 104 cfu/mL for BAL, which collects 1 mL of secretions in 10 to 100 mL of effluent, represents 105 to 106 cfu/mL.190-192
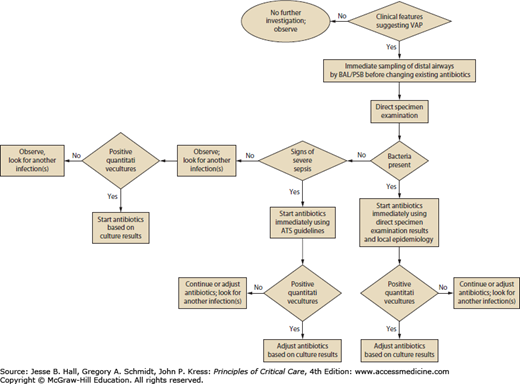
Using this strategy, therapeutic decisions are tightly protocolized, using the results of direct examination of distal pulmonary samples and results of quantitative cultures in deciding whether to start antibiotic therapy, which pathogens are responsible for infection, which antimicrobial agents to use, and whether to continue therapy (Fig. 59-2).
One major technical problem with all bronchoscopic techniques is proper selection of the sampling area in the tracheobronchial tree. Almost all intubated patients have purulent-looking secretions and the secretions first seen may represent those aspirated from another site into gravity-dependent airways or from upper-airway secretions aspirated around the endotracheal tube. Usually, the sampling area is selected based on the location of infiltrate on chest radiograph or the segment visualized during bronchoscopy as having purulent secretions.193 Collection of secretions in the lower trachea or mainstem bronchi, which may represent recently aspirated secretions around the endotracheal tube cuff, should be avoided. In patients with diffuse pulmonary infiltrates or minimal changes in a previously abnormal chest radiograph, determining the correct airway to sample may be difficult. In these cases, sampling should be directed to the area where endobronchial abnormalities are maximal.194 In case of doubt, and because autopsy studies indicate that VAP frequently involves the posterior portion of the right lower lobe, this area should probably be sampled as priority.195 While in the immunosuppressed host with diffuse infiltrates bilateral sampling has been advocated, there is no convincing evidence that multiple specimens are more accurate than single specimens for diagnosing nosocomial bacterial pneumonia in ventilated patients.
Because BAL harvests of cells and secretions from a large area of the lung and specimens can be microscopically examined immediately after the procedure to detect the presence or absence of intracellular or extracellular bacteria in the lower respiratory tract, it is particularly well suited to provide rapid identification of patients with pneumonia.191,196-201 Assessment of the degree of qualitative agreement between Gram stains of BAL fluid and PSB quantitative cultures for a series of 51 patients with VAP, however, showed correspondence to be complete for 51%, partial for 39%, and nonexistent for 10% of the cases.198 In 21 studies, pooled sensitivity and specificity of Gram stain for VAP was 0.79 and 0.75, respectively, with a negative predictive value of 91%, suggesting that VAP is unlikely with a negative Gram stain.202
Many groups have investigated the value of quantitative BAL culture for the diagnosis of pneumonia in ICU patients.191,203,204 When the results of the 11 studies evaluating BAL fluids from a total of 435 ICU patients with nosocomial pneumonia were pooled, overall accuracy was very close to that of PSB: the Q value was 0.84 (Q represents the intersection between the summary receiver-operating characteristics [ROC] curve and a diagonal from the upper-left corner to the lower-right corner of the ROC space).203 Similar conclusions were drawn in another meta-analysis, which pooled the results of 23 studies: sensitivity and specificity of BAL were 73 ± 18% and 82 ± 19%, respectively.204 When analysis in these studies was restricted to patients without prior antibiotics or when only lung tissue cultures were used as the reference standard, results of bronchoscopic techniques for determining pneumonia were much better, with a sensitivity always >80%.
Other studies have confirmed the accuracy of bronchoscopic techniques for diagnosing nosocomial pneumonia. In a study evaluating spontaneous lung infections occurring in ventilated baboons with permeability pulmonary edema, Johanson et al found excellent correlation between the bacterial content of lung tissue and results of quantitative culture of lavage fluid.96 BAL recovered 74% of all species present in lung tissue, including 100% of species present at a concentration ≥104 cfu/g of tissue. Similarly, in 20 ventilated patients who had not developed pneumonia before the terminal phase of disease and who had no recent changes in antimicrobial therapy, Chastre et al found that bronchoscopic BAL specimens obtained just after death identified 90% of all species present in the lung, with a strong correlation between the results of quantitative cultures of both specimens.191 These findings confirm that bronchoscopic BAL samples very reliably identify, both qualitatively and quantitatively, microorganisms present in lung segments, even when the pneumonia develops as a superinfection in a patient already receiving antimicrobial treatment for several days.
Values within 1 log10 of the cutoff must, however, be interpreted cautiously, and bronchoscopy should be repeated in symptomatic patients with a negative (<104 cfu/mL) result.205 Many technical factors, including medium and adequacy of incubation, and antibiotic or other toxic components, may influence results. Reproducibility of PSB sampling has been recently evaluated by three groups.206-208 Although in vitro repeatability was excellent and in vivo qualitative recovery 100%, quantitative results were more variable. In 14% to 17% of patients, results of replicate samples fell on both sides of the 103 cfu/mL threshold, and results varied by more than 1 log10 in 59% to 67% of samples.206-208 This variability is presumably related to both the irregular distribution of organisms in secretions and the very small volume actually sampled by PSB. As with all diagnostic tests, borderline PSB and/or BAL quantitative culture results should be interpreted cautiously, and the clinical circumstances should be considered before reaching any therapeutic decision.
The most compelling argument for invasive techniques coupled with quantitative cultures of PSB or BAL specimens is that they can reduce excessive antibiotic use. There is little disagreement that the clinical diagnosis of nosocomial pneumonia is overly sensitive and leads to the unnecessary use of broad-spectrum antibiotics. Because bronchoscopic techniques may be more specific, their use would reduce antibiotic pressure in the ICU, thereby limiting the emergence of drug-resistant strains and the attendant increased risks of superinfection.36,209 When culture results are available, BAL and/or PSB techniques facilitate precise identification of the offending organisms and their susceptibility patterns. Such data are invaluable for optimal antibiotic selection in patients with a true VAP. They also increase the confidence and comfort level of health care workers in managing patients with suspected nosocomial pneumonia.210 The more targeted use of antibiotics also could reduce overall costs, despite the expense of bronchoscopy and quantitative cultures, and minimize antibiotic-related toxicity. This is particularly true in patients who have late-onset VAP, in whom expensive combination therapy is commonly recommended. A conservative cost-analysis in a trauma ICU suggested that the discontinuation of antibiotics upon the return of negative bronchoscopic quantitative culture results could lead to a savings of more than $1700 per patient suspected of VAP.211
Finally, a major benefit of a negative bronchoscopy is to direct attention away from the lungs as the source of fever. Many hospitalized patients with negative bronchoscopic cultures have other potential sites of infection that can be identified via a simple diagnostic protocol. In 50 patients with suspected VAP who underwent a systematic diagnostic protocol designed to identify all potential causes of fever and pulmonary densities, Meduri et al confirmed that lung infection was present in only 42% of cases; the frequent occurrence of multiple infectious and noninfectious processes justifies a systematic search for the source of fever in this setting.150 Delay in diagnosis or definitive treatment of the true site of infection may lead to prolonged antibiotic therapy, more antibiotic-associated complications, and induction of further organ dysfunction.212
At least 15 studies have described a variety of nonbronchoscopic techniques using various types of endobronchial catheters for sampling distal lower respiratory tract secretions; globally, results have been similar to those obtained with bronchoscopy.213 Compared to conventional PSB and/or BAL, nonbronchoscopic techniques are less invasive, can be performed by clinicians not qualified to perform bronchoscopy, have lower initial costs than bronchoscopy, avoid potential contamination by the bronchoscopic channel, are associated with less compromise of gas-exchange during the procedure, and can be performed even in patients intubated with small endotracheal tubes. Disadvantages include the potential sampling errors inherent in a blind technique and the lack of airway visualization. Although autopsy studies indicate that pneumonia in ventilator-dependent patients has often spread into every pulmonary lobe and predominantly involves the posterior portion of the lower lobes, several clinical studies on ventilated patients with pneumonia contradict those findings, as some patients had sterile cultures of PSB specimens from the noninvolved lung.32,214 Furthermore, although the authors of most studies concluded that the sensitivities of nonbronchoscopic and bronchoscopic techniques were comparable, the overall concordance was only approximately 80%, emphasizing that, in some patients, the diagnosis could be missed by a blind technique, especially in the case of pneumonia involving the left lung.32
Performing microbiologic cultures of pulmonary secretions for diagnostic purposes after initiation of new antibiotic therapy in patients suspected of having developed VAP leads to a high rate of false-negative results, regardless of the method of obtaining the secretions. In fact, all microbiological techniques are of limited value in patients with a recent infiltrate who have received new antibiotics, even for less than 24 hours. A negative finding could indicate that the patient has been successfully treated for pneumonia and the bacteria are eradicated, or that the patient had no lung infection to begin with. Using both PSB and BAL, Souweine et al prospectively investigated 63 episodes of suspected VAP.215 If patients had been treated with antibiotics but did not have a recent change in antibiotic class, sensitivity of PSB and BAL culture (83% and 77%, respectively) were similar to the sensitivities achieved in patients not being treated with antibiotics. In other words, prior therapy did not reduce the yield of diagnostic testing among patients receiving current antibiotics given to treat a prior infection. Conversely, if therapy was recent, sensitivity of invasive diagnostic methods, using traditional thresholds, was only 38% with BAL and 40% with PSB.215 These two clinical situations should be clearly distinguished before interpreting the results of pulmonary secretion cultures, irrespective of how they were obtained. In the second situation, when the patient receives new antibiotics after the appearance of signs suggesting VAP, no conclusion concerning the presence or absence of pneumonia can be drawn if culture results are negative.215-217 Pulmonary secretions therefore need to be obtained before starting new antibiotics, as is the case for all types of microbiologic samples.
Procalcitonin (PCT), a 116-amino-acid peptide which is one of the precursors of the hormone calcitonin, has been described as a good diagnostic marker of bacterial infection in patients with community-acquired infections, especially in patients with lower respiratory tract infection.218-221 Moreover, several interventional trials have shown that PCT could be used to start or to postpone antibiotic treatment in community-acquired lower respiratory tract infections.222-226 In patients with nosocomial infections, and in particular in patients with VAP, its usefulness as a diagnostic marker is more doubtful.227-231 There are several reasons to explain why PCT is not a good diagnostic marker in patients with suspected VAP. First, pneumonia may be a localized infection; thus, as for other localized infections, PCT can be synthesized locally without systemic release, explaining its low serum level or apparent decrease in patients with true pulmonary infections. Second, ICU-patients may suffer from previous severe sepsis or septic shock, multiorgan failure, or may have developed a systemic inflammatory response syndrome after surgery or trauma, conditions known to increase blood level of biomarkers including PCT in the absence of infection.230 Thus, a high level of PCT the day VAP is suspected is not useful, because it is not possible to distinguish an elevation due to a previous noninfectious condition from an elevation due to an active infection. Third, it is known that a time lag of 24 to 48 hours can exist between bacterial infection onset and peak PCT release, and that may also explain the apparent low level of PCT on the day of VAP onset. Incorporating PCT values in clinical score (such as CPIS) did not improve its diagnostic value.229,230
The soluble Triggering Receptor Expressed on Myeloid Cells-1 (sTREM-1) molecule is known to be specifically released during several infectious processes.232 Although it was apparently a reliable marker of pneumonia, especially VAP, more recent studies obtained contradictory findings, thereby raising doubt as to its usefulness for VAP diagnosis.228,233-235 Pending additional studies, and because this marker is not routinely available, sTREM-1 is not recommended as an indicator to guide antibiotic use in such situations.
GNB cause >80% of VAP episodes and are associated with high mortality. Because GNB pneumonia might be diagnosed more rapidly by endotoxin measurement in BAL fluid, several investigators tested this hypothesis.236-239 Applying a threshold of >5 EU/mL in BAL fluid yielded the best operating characteristics for GNB-pneumonia diagnosis (100% sensitivity; 75% specificity; area under the ROC curve: 0.88) in a series of 63 hospitalized adults suspected of having lung infection.237 Three other studies confirmed the potential contribution of this tool.236,238,239 These findings suggest that endotoxin determination in BAL fluid might become an acceptable adjunct for the rapid diagnosis of GNB pneumonia in a near future, when it will be available at the bedside.
Aside from decision-analysis studies240,241 and a single retrospective study,210 five trials have used a randomized scheme to assess the effect of a diagnostic strategy on antibiotic use and outcome in patients suspected of having VAP39,40,242-244 In three randomized studies conducted in Spain, no differences in mortality and morbidity were found when either invasive (PSB and/or BAL) or noninvasive (quantitative endotracheal aspirate cultures) techniques were used to diagnose VAP.39,40,242 These studies were relatively small, ranging from 51 to 88 patients. Antibiotics were continued in all patients despite negative cultures, thereby offsetting the potential advantage of the specific diagnostic test in patients with suspected VAP. Several prospective studies have concluded that antibiotics can be stopped in patients with negative quantitative cultures, without adversely affecting the recurrence of pneumonia and mortality.196,245,246
In a French study in which 413 patients were randomized, those receiving bacteriological management using BAL and/or PSB had a lower mortality rate on day 14, lower sepsis-related organ failure assessment scores on day 3 and 7, and less antibiotic use.243 Pertinently, 22 nonpulmonary infections were diagnosed in the bacteriological strategy group and only 5 in the clinical strategy group, suggesting that overdiagnosis of VAP can lead to errors in identifying nonpulmonary infections. A randomized trial conducted by the Canadian Critical Care Trials Group investigated the effect of different diagnostic approaches on outcomes of 740 patients suspected of having VAP.244 There was no difference in the 28-day mortality rate in patients in whom BAL was used versus those in whom endotracheal-aspiration was used as the diagnostic strategy. The BAL group and the endotracheal-aspiration group also had similar rates of targeted antibiotic therapy on day 6, days alive without antibiotics, and maximum organ-dysfunction scores. Unfortunately, information about how the decision algorithms were followed in the two diagnostic arms once cultures were available was not provided, raising uncertainties about how deescalation of antibiotic therapy was pursued in patients with negative BAL cultures. Obviously, the potential benefit of using a diagnostic tool such as BAL for safely restricting unnecessary antimicrobial therapy in such a setting can only be obtained when decisions regarding antibiotics are closely linked to bacteriological results, including both direct examination and cultures of respiratory specimens.
Our personal bias is that use of bronchoscopic techniques to obtain BAL specimens from an affected area of the lung in ventilated patients with signs suggestive of pneumonia enables the formulation of a therapeutic strategy superior to that based exclusively on clinical evaluation. Bronchoscopic techniques, when performed before the introduction of new antibiotics, enable physicians to identify most patients who need immediate treatment, and help select optimal therapy in a safe and well-tolerated manner. These techniques also avoid resorting to broad-spectrum coverage of all patients who develop a clinical suspicion of infection.247 The full impact of this decision tree on patient outcome remains controversial.243,244 Yet, being able to withhold antimicrobial treatment from some patients without infection may constitute a distinct advantage in the long term: it minimizes the emergence of resistant microorganisms in the ICU and redirects the search for another (the true) infection site.248,249
In patients with clinical evidence of severe sepsis and rapid worsening organ dysfunction, hypoperfusion or hypotension, or patients with a very high pretest probability of disease, the initiation of antibiotic therapy should not be delayed while awaiting bronchoscopy. Patients should be given immediate antibiotics. In this situation, simple nonbronchoscopic procedures find their best justification, allowing distal pulmonary secretions to be obtained on a 24-hour basis, just before starting new antimicrobial therapy.
Despite broad experience with PSB and BAL, it remains unclear which should be used. Most investigators prefer BAL over PSB to diagnose bacterial pneumonia, because BAL: (1) has a slightly higher sensitivity to identify VAP-causative microorganisms; (2) enables better selection of an empiric antimicrobial treatment before culture results are available, based on microscopically examined cytocentrifuged preparations; (3) is less dangerous for many critically ill patients; (4) is less costly; and (5) may provide useful clues for the diagnosis of other types of infections. Nevertheless, a very small return on BAL may contain only diluted material from the bronchial rather than alveolar level, and thus give rise to false-negative results, particularly in patients with very severe COPD. In these patients, the value of BAL is greatly diminished and PSB is preferred.192
When bronchoscopy is not available, we recommend replacing bronchoscopy in the algorithm in Figure 59-2 by one of the simplified nonbronchoscopic diagnostic techniques, or following the strategy described by Singh et al.250 Such an approach avoids prolonged treatment of patients with a low likelihood of infection, while allowing immediate treatment of patients with VAP.
TREATMENT
Despite many advances in antimicrobial therapy, successful treatment of patients with nosocomial pneumonia remains a difficult and complex undertaking. No consensus has been reached concerning issues as basic as the optimal antimicrobial regimen for therapy or duration of treatment. Although some investigators have recommended two-drug parenteral therapy for most cases, recent data have demonstrated the efficacy of newer β-lactam antibiotics as monotherapy for some patients. Similarly, the efficacy of endotracheal or aerosolized antibiotics as either the sole or adjunctive therapy for gram-negative pneumonia remains controversial. In fact, to date, evaluation of various antimicrobial strategies for the treatment of bacterial pneumonia in mechanically ventilated patients has been difficult for several reasons.
First, as indicated earlier, obtaining a definitive diagnosis of pneumonia in critically ill patients is far from easy. Although clinically distinguishing between bacterial colonization of the tracheobronchial tree and true nosocomial pneumonia is difficult, nearly all previous therapeutic investigations have relied solely on clinical diagnostic criteria and therefore probably have included patients who did not have pneumonia. Second, most of these studies used cultures of tracheal secretions as the major source of samples for microbiologic analysis despite the fact that the upper respiratory tract of most ventilated patients usually is colonized with multiple potential pathogens. Finally, the lack of an adequate technique to directly sample the infection site in the lung has hampered study of both the ability or inability of antibiotics to eradicate the causative pathogens from the lower respiratory tract and therefore the ability to predict their bacteriologic efficacy.
Montravers and colleagues evaluated the bacteriologic and clinical efficacy of antimicrobial therapies selected on the basis of the etiologic microorganisms identified by cultures of PSB samples obtained during bronchoscopy for the treatment of nosocomial bacterial pneumonia in 76 patients receiving MV.217 Using follow-up PSB sample culture to assess the infection site in the lung directly, their results demonstrated that the administration of an antimicrobial therapy combining, in most cases, two effective agents was able to sterilize or contain the lower respiratory tract infection after only 3 days of treatment in 67 (88%) of the patients included in the study. The only two bacteriologic failures were observed in patients who did not receive adequate treatment because of errors in the selection of antimicrobial drugs. Early superinfection caused by bacteria resistant to the initial antibiotics was, however, documented in 7 (9%) patients, emphasizing the need to monitor carefully the impact of treatment on the initial microbial flora for optimal management of such patients when the clinical response is suboptimal. Furthermore, results of cultures of follow-up PSB samples were well correlated with the clinical outcome noted during the 15-day observation period, making this test a good prognostic indicator in patients with nosocomial bacterial pneumonia. Whereas the percentage of patients with clinical improvement was 96% and 82% in those with sterilized or persistent low-grade infection, respectively, it was only 44% in those with persistent high-grade infection. Using such techniques to sample the infection site in the lung directly therefore may provide a more rigorous evaluation of different antimicrobial strategies.
Failure to initiate prompt appropriate and adequate therapy (the etiologic organism is sensitive to the therapeutic agent, the dose is optimal, and the correct route of administration is used) has been a consistent factor associated with increased mortality.44,164-166 Because pathogens associated with inappropriate initial empiric antimicrobial therapy mostly include antibiotic-resistant microorganisms, such as P. aeruginosa, Acinetobacter species, K pneumoniae, Enterobacter species, and MRSA, patients at risk for infection with these organisms should initially receive a combination of agents that can provide a very broad spectrum of coverage.1,182 Several observational studies have now confirmed that the use of a regimen that combines initially a broad spectrum betalactam with an aminoglycoside increases the proportion of patients appropriately treated as compared to monotherapy or to a regimen combining a betalactam with a fluoroquinolone.171,251-253 Only patients with early-onset infection, mild or moderate disease severity, and no specific risk factors for multiresistant strains, such as prolonged duration of hospitalization (>5 days), admission from a health care–related facility, recent prolonged antibiotic therapy, and specific local epidemiological data, can be treated with a narrow-spectrum drug, such as a nonpseudomonal third-generation cephalosporin.1,3,254
When risk factors for multiresistant pathogens are present, the choice of agents should be based on local patterns of antimicrobial susceptibility and anticipated side effects. Having a current and frequently updated knowledge of local bacteriologic patterns can increase the likelihood that appropriate initial antibiotic treatment will be prescribed.62 The choice should also take into account which therapies patients have recently received (within the past 2 weeks), striving not to repeat the same antimicrobial class, if possible.255-257
Use of endotracheal aspirate surveillance cultures two or three-times weekly may also makes it possible to increase the proportion of patients receiving initially appropriate antimicrobial therapy.258-262 This strategy rests upon the observation that VAP caused by potentially multiresistant pathogens is typically preceded by colonization of the oropharynx and the proximal airways by the same strains. In order to be of clinical use in directing initial antibiotic therapy, surveillance cultures must be able to detect this colonization rapidly and with high sensitivity, as false-negative results would place the patient at risk for inappropriate therapy. Moreover, a focused antibiotic choice, with limitation of unnecessary broad-spectrum drugs, requires a low number of false-positive surveillance results. Patients with a prolonged hospital stay and numerous previous antibiotics will benefit the most. Thus, such a strategy can only be recommended when the local prevalence of multiresistant microorganisms is high, when current empirical therapy is suboptimal and cannot be easily increased through adaptation of a decision tree, and when the resources for the microbiological work-up are available.259
Because clinical signs of infection are nonspecific and can be caused by any condition associated with an inflammatory response, many more patients than necessary are initially treated with antibiotics. Thus, it is important to use serial clinical evaluations and microbiologic data to reevaluate therapy after 48 to 72 hours.1,263
The decision tree should contain an explicit statement that patients with a low probability of infection will be identified and therapy stopped when infection appears unlikely. The algorithm cannot be exactly the same for a “clinical” or an “invasive” strategy, depending on the general principles and microbiological techniques on which the diagnostic strategy is constructed (see section above on “Diagnosis”). Using a “clinical strategy” in which all patients with clinically suspected pulmonary infection are treated with new antibiotics, even when the likelihood of infection is low, the decision whether to continue antibiotics or not on day 3 will be based essentially on a combination of clinical signs.185 Briefly, antibiotics are discontinued if and only if the clinical diagnosis of VAP is unlikely (there are no definite infiltrates found on chest radiography at follow-up), tracheobronchial aspirate culture results are non-significant, and there is no severe sepsis or shock.
Related posts:






Full access? Get Clinical Tree


