KEY POINTS
Of critically ill patients with conventional indications for a fluid bolus, only about half will respond with a meaningful increase in perfusion.
Fluid therapy that does not boost perfusion may cause harm by impairing lung function or producing edema in other organs.
Static hemodynamic parameters, such as central venous pressure, have little value in guiding fluid therapy.
Fluid responsiveness can be predicted using cardiopulmonary interactions to probe circulatory function or through passive leg raising.
Dynamic fluid-responsiveness predictors are accurate, but require careful attention to preconditions for validity.
Critical illness often cripples the circulation. For example, septic shock combines ventricular dysfunction; arteriolar dilation; vascular obstruction; and volume depletion due to transudation of fluid from the vascular space into tissues, venodilation, reduced oral intake, and heightened insensible loss. Trauma produces similar effects through hemorrhage, spinal injury, cardiac tamponade, tension pneumothorax, acidemia, and cardiac dysfunction. These join to compromise perfusion globally, threatening the function of vital organs. Urgent resuscitation improves outcome in shock, showing that time is of the essence, a concept captured in the phrase “the golden hour.”1,2 Treating hypovolemia has been a central tenet of shock management. Nevertheless, many controversies remain regarding the details of shock resuscitation, including the role and type of fluid therapy, metrics for assessing the response, and clinical end points.
Initial resuscitation transforms a hypovolemic, hypodynamic circulation into one where oxygen transport is normal or high, at least at the whole body level, in most septic adults2,3 and even following trauma and cardiac arrest.4 In contrast to the average patient entering the early goal-directed trial (EGDT),2 once fluids, antimicrobials, vasoactive drugs, and perhaps blood have been given, resuscitated patients typically display elevated central venous pressure (CVP), cardiac output, and mixed and central venous oxyhemoglobin saturations (SvO2SvO2 and ScvO2, respectively). There is no longer global hypoperfusion as judged by any measure of oxygen transport, even when hypotension, lactic acidosis, and organ dysfunction persist. Nevertheless, the circulation remains grossly impaired and mean arterial pressure is rarely restored to normal.
Indeed, persistent hypotension and progressive organ failures often prompt further fluid administration. When given additional fluid, some patients will respond: Blood pressure, cardiac output, oxygen delivery, ScvO2, or urine output increases. Other patients will not: Hemodynamics fail to improve and the fluid bolus is ineffective, at best.5 Moreover, ineffective fluid challenges often lead to additional boluses, culminating in a grossly edematous patient (still hypotensive and oliguric). Critically ill patients also receive nutrition, sedatives, analgesics, antimicrobials, vasoactive drugs, insulin infusions, and agents to reduce the risk of gastric hemorrhage, all of which contribute to a surprising degree of fluid overload. For example, in the liberal fluid arm of the fluid and catheter treatment trial (FACTT6) subjects received more than 4 L per day. The consequence was a 7-day net positive fluid balance of 7 L. Fluid balance in the earlier ARDS Network trials (where fluid therapy was at the discretion of the intensivist, not guided by a protocol) was found to be essentially superimposable on the liberal arm of the FACTT.6 Thus routine critical care appears to be associated with large fluid loads and a very substantial net positive fluid balance.
Just as too little fluid resuscitation risks harm, too much fluid may also be deadly. Identifying patients who are likely to respond to fluids (so that sufficient fluid can be given timely) and those who are not (focusing attention on effective treatment and sparing them useless fluids) is a daily challenge in the intensive care unit (ICU). Yet predicting fluid responsiveness is not a trivial task. This chapter reviews the association between fluid resuscitation and outcomes in critical illness; the limitations of static predictors of fluid response (such as CVP); the physiological underpinning of dynamic predictors (such as stroke volume variation [SVV]) and their role in guiding fluid therapy; and a clinical approach to the patient. Few patients in the first hours of sepsis, trauma, or other forms of shock have been studied with regard to endpoints of fluid therapy. For example, in the trial of early goal-directed resuscitation, the target was the central venous oxyhemoglobin saturation—CVP goals were identical between groups.2 Although the EGDT subjects were given more fluid in the first 6 hours (4981 ± 2984 vs 3499 ± 2438; p < 0.001), they also received more dobutamine and packed cell transfusion, making it difficult to attribute any particular benefit to the fluid, per se. Further, there is no evidence that goal-directed resuscitation after the first 6 hours confers any benefit.7-9 Moreover, concerns have been raised about the generalizability of the EGDT study in light of the atypical patient population and other problems.10 Thus we emphasize here the patient who is hypoperfused following initial resuscitation and for whom additional fluid therapy is considered.
EXCESS FLUID CAUSES HARM
Fluid infused into the vascular space ultimately equilibrates with other fluid compartments. Unnecessary fluid (ie, fluid that does not enhance perfusion) will cause or exacerbate edema in lungs, heart, gut, skin, brain, and other tissues. At times, this creates clinically obvious organ failure, such as respiratory failure, abdominal compartment syndrome,11,12 or cerebral edema and herniation. Multiple studies have correlated positive fluid balance with reduced survival in acute respiratory distress syndrome (ARDS) or sepsis.13-15 For example, in a large European observational cohort, positive fluid balance was among the strongest predictors of death, even after correcting for severity of illness.16 The Vasopressin in Septic Shock Trial (VASST) showed that positive fluid balance correlated with a higher risk of dying.17
Similar results have been shown in patients with acute renal failure.18 In a study of monitoring techniques in critically ill patients a secondary logistic regression analysis identified positive fluid balance as a significant predictor of mortality (OR 1.0002 for each mL/day; p = 0.0073).19 Similar results were seen in a prospective trial of goal-directed fluid therapy in patients undergoing major colorectal surgery.20 Those randomized to goal-directed treatment got significantly more fluid but did not have better outcomes. In fact, in aerobically fit subjects, outcomes were inferior. Positive fluid balance may also impede liberation from mechanical ventilation in general critically ill patients. In a study of 87 ventilated subjects, both cumulative and short-term positive fluid balance were associated with failure of a spontaneous breathing trial.21 Negative fluid balance was as predictive of weaning outcomes as the rapid shallow breathing index. This association has also been noted in critically ill surgical patients.22 Lastly, restrictive fluid strategies may reduce length of stay following major surgery.23
These retrospective or uncontrolled analyses leave open the question as to whether positive fluid balance contributed to deaths or was merely a marker of severity of illness, so further controlled study is warranted. Two prospective trials in subjects with ARDS have shown that diuresis improves outcome, including time on the ventilator and ICU length of stay.6,24 The second of these randomized 1001 subjects with acute lung injury or ARDS to conservative (CVP <4 or pulmonary artery occlusion pressure [PAOP] <8 mm Hg) versus liberal (CVP 10-14 or PAOP 14-18 mm Hg) fluid management. Although there was no difference in 60-day mortality (the primary outcome), the conservative fluid strategy improved lung function, increased ventilator-free days, and reduced ICU length of stay.6 Of course, all of these subjects had pulmonary edema, a condition expected to respond to diuresis, and active fluid management was only carried out when subjects were hemodynamically stable so it is not clear that these findings can be extrapolated to patients with shock.
The role of fluids in shock was further called into question in a study of hypoperfused children with severe infection.25 Designed largely as a comparison of crystalloid versus colloids, this study is remarkable for having included a third treatment arm that got no fluid bolus. While the saline and albumin groups had similar survival, the “no fluid bolus” arm had the best outcome. Although this study involved children cared for in hospitals unable to provide intensive care, it nevertheless raises questions about our presumptions regarding the benefits of volume resuscitation.
ASSESSING INTRAVASCULAR VOLUME AND PREDICTING FLUID RESPONSIVENESS
The most direct means to assess whether additional fluid will raise perfusion is to perform a “fluid challenge”: infuse a fluid bolus and measure cardiac output, ScvO2, or some other clinically relevant parameter reflecting perfusion (blood pressure reflects poorly whether perfusion truly rises26). It is not clear, however, how much fluid constitutes an adequate fluid challenge. Also, if the fluid bolus has no impact, renal dysfunction may impede reversing its contribution to fluid overload. If only rare patients failed to respond to a fluid bolus, this would not be a major problem. Across many studies, however, more than half of fluid boluses judged to be clinically indicated are actually ineffective and potentially harmful.5,27 For example, 150 fluid boluses were studied in 96 subjects mechanically ventilated for severe sepsis over a 3-year period.28 In only 65 instances (43%) did cardiac index rise at least 15%. These results are typical of prospective studies of fluid challenge.29-38
Since fluid challenge fails to help many hypotensive patients and may cause harm, predicting the likelihood of response should be of great clinical value. Historically, clinicians have generally used static hemodynamic values (eg, CVP or PAOP) to judge whether fluids are likely to boost the circulation. As discussed below, however, these measures have almost no ability to distinguish fluid responders from nonresponders. In contrast, dynamic indices such as SVV are quite accurate, having much higher positive and negative predictive values.
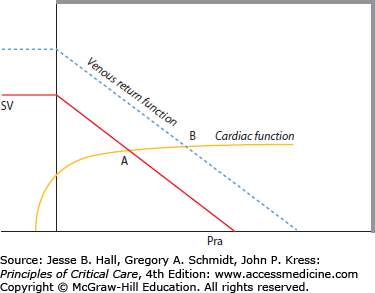
CVP or Right Atrial Pressure: CVP is probably the most used parameter for judging whether fluids should be given. Nevertheless, a large number of studies show that CVP fails to discriminate responders from nonresponders.29,39-41 Following the EGDT trial and publication of the original Surviving Sepsis Campaign guidelines (which proposed a CVP target of greater than 8 mm Hg for nonventilated patients and greater than or equal to 12 mm Hg for ventilated patients42) a group of French investigators examined the role of cardiac filling pressures as predictors of fluid responsiveness in 96 ventilated, septic subjects.28 Overall, the predictive power of the CVP was poor: When CVP was less than 12, the positive predictive value was only 47%. Even when CVP was much lower in these ventilated patients (less than 5 mm Hg), the positive predictive value was still only 47%. These results should not be surprising. Raising CVP can only augment perfusion when cardiac function is not limited, as can be seen by examining the relationship of CVP to cardiac output (Fig. 34-1). While “low” CVP tends to indicate a point on the steep portion of the cardiac function curve in a population, huge variation makes specific values of little use in any individual patient.
FIGURE 34-1
Right atrial pressure (Pra) is on the x-axis, while stroke volume (SV) is on the y-axis. For a patient with the venous return and cardiac function curves represented (solid straight and curved lines, respectively), their intersection at Point A shows the steady-state Pra and SV. Fluid therapy (which shifts the venous return function curve rightward producing a new intersection Point B) increases Pra but, because the cardiac function curve is so flat, will not raise stroke volume.
Wedge or Pulmonary Artery Occlusion Pressure: Pulmonary artery catheters (PAC) have been used widely for monitoring critically ill, heart failure, and perioperative patients. Although many clinicians consider the PAOP to be the gold standard for determining left ventricular (LV) preload (and judging volume status), the correlation of PAOP and LV end-diastolic volume is feeble.43 Surprisingly, even in normal volunteers, PAOP fails to reflect preload,39 thought due to wide variation in diastolic compliance even in health. More importantly, values of PAOP are no better than those of CVP in predicting the response to fluid challenge.29,40,44 In septic subjects, a PAOP less than 12 mm Hg predicts a rise in cardiac output with a positive predictive value of only 54%.28 Like the CVP, PAOP should not be used to judge the volume state in severe sepsis or to predict the role for further fluid administration.
Related posts:






Full access? Get Clinical Tree


