A strategy of time separation between the administration of a dissociative induction agent and the neuromuscular blocker to allow preintubation optimization.
INTRODUCTION
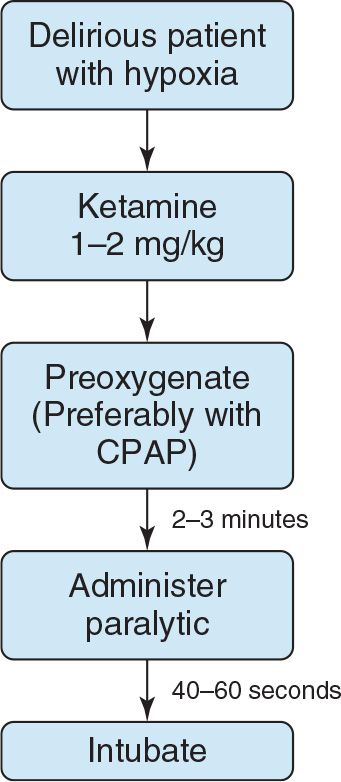
Delayed sequence intubation (DSI) differs from rapid sequence intubation (RSI), in that it separates the induction and paralysis to allow preintubation procedures such as preoxygenation in patients who are noncompliant (e.g. delirious) (FIGURE 3.1). It can be thought of as procedural sedation where the procedure is preoxygenation. In indicated situations requiring further preoxygenation, DSI is an alternative to precipitous intubation without full paralytic effect or bag-mask ventilation in the sedated and paralyzed patient. Respectively, these two traditional options increase the risk of first-pass failure or the risk of gastric insufflation and passive regurgitation in sick, nonfasted patients. Both options ensure an abbreviated period before critical levels of hypoxemia.
CLASSIC INDICATIONS
![]() Preoxygenation prior to intubation in a delirious or otherwise uncooperative hypoxemic and/or hypercapnic patient
Preoxygenation prior to intubation in a delirious or otherwise uncooperative hypoxemic and/or hypercapnic patient
![]() Adequate oxygenation but need for further denitrogenation of the lungs and bloodstream in order to prolong the safe apnea period in a delirious or otherwise uncooperative patient
Adequate oxygenation but need for further denitrogenation of the lungs and bloodstream in order to prolong the safe apnea period in a delirious or otherwise uncooperative patient
EXTENDED INDICATIONS
![]() Need for an additional procedure or further optimization of physiologic parameters prior to intubation in a delirious or otherwise uncooperative patient
Need for an additional procedure or further optimization of physiologic parameters prior to intubation in a delirious or otherwise uncooperative patient
![]() Nasogastric tube placement for a patient with upper gastrointestinal bleed and stomach filled with blood
Nasogastric tube placement for a patient with upper gastrointestinal bleed and stomach filled with blood
![]() Need to optimize patient’s blood pressure secondary to hypotension
Need to optimize patient’s blood pressure secondary to hypotension
![]() Need to optimize patient’s respiratory and metabolic status secondary to metabolic acidosis
Need to optimize patient’s respiratory and metabolic status secondary to metabolic acidosis
CONTRAINDICATIONS
![]() Need for a “crash” airway
Need for a “crash” airway
![]() Patient unable to breathe spontaneously
Patient unable to breathe spontaneously
![]() Patient unable to protect his/her own airway
Patient unable to protect his/her own airway
![]() Relative contraindications—situations in which ketamine would be less than favorable and absence of alternative agents e.g.dexmedetomidate or droperidol
Relative contraindications—situations in which ketamine would be less than favorable and absence of alternative agents e.g.dexmedetomidate or droperidol
![]() Elderly patients with coronary artery disease
Elderly patients with coronary artery disease
![]() Patients with elevated blood pressure or tachycardia
Patients with elevated blood pressure or tachycardia
EQUIPMENT
![]() Equipment for preoxygenation
Equipment for preoxygenation
![]() Nasal cannula (NC)
Nasal cannula (NC)
![]() Nonrebreather (NRB) mask
Nonrebreather (NRB) mask
![]() Consider methods for positive-pressure ventilation if the patient is exhibiting physiologic shunt
Consider methods for positive-pressure ventilation if the patient is exhibiting physiologic shunt
![]() Ventilator and noninvasive ventilation (NIV) mask
Ventilator and noninvasive ventilation (NIV) mask
![]() Bag-valve mask (BVM) with adjustable positive end-expiratory pressure (PEEP) valve
Bag-valve mask (BVM) with adjustable positive end-expiratory pressure (PEEP) valve
![]() Induction medication that maintains ventilatory drive and airway reflexes
Induction medication that maintains ventilatory drive and airway reflexes
![]() That is ketamine (1–2 mg/kg) given over approximately 30 seconds
That is ketamine (1–2 mg/kg) given over approximately 30 seconds
![]() Standard equipment and medications for airway management
Standard equipment and medications for airway management
STANDARD TECHNIQUE
![]() Administration of induction agents that do not blunt spontaneous ventilations or airway reflexes
Administration of induction agents that do not blunt spontaneous ventilations or airway reflexes
![]() Give a dissociative dose of ketamine (1–2 mg/kg) over approximately 30 seconds
Give a dissociative dose of ketamine (1–2 mg/kg) over approximately 30 seconds
![]() Alternative agents
Alternative agents
![]() Dexmedetomidine 1 μg/kg over 10 minutes
Dexmedetomidine 1 μg/kg over 10 minutes
![]() Droperidol 5 to 10 mg
Droperidol 5 to 10 mg
![]() After intubation, check electrocardiogram (ECG) to determine whether any QT prolongation
After intubation, check electrocardiogram (ECG) to determine whether any QT prolongation
![]() For these two latter agents, a separate induction agent should be administered just prior to neuromuscular blocker administration
For these two latter agents, a separate induction agent should be administered just prior to neuromuscular blocker administration
![]() Preoxygenation and denitrogenation in standard manner with oxygen saturation >95% for 2 to 3 minutes or at least eight vital capacity (VC) breaths (note: patients who have received a DSI agent cannot take VC breaths)
Preoxygenation and denitrogenation in standard manner with oxygen saturation >95% for 2 to 3 minutes or at least eight vital capacity (VC) breaths (note: patients who have received a DSI agent cannot take VC breaths)
![]() NRB
NRB
![]() Alternatives in patient exhibiting shunt physiology (saturation not improving with increased FIO2)
Alternatives in patient exhibiting shunt physiology (saturation not improving with increased FIO2)
![]() BVM with PEEP valve
BVM with PEEP valve
![]() NIV—PEEP/Continuous positive airway pressure (CPAP)
NIV—PEEP/Continuous positive airway pressure (CPAP)
![]() PEEP levels between 5 and 15 cm H2O
PEEP levels between 5 and 15 cm H2O
![]() Follow with apneic oxygenation
Follow with apneic oxygenation
![]() Concurrent preparation for definitive airway management in standard manner
Concurrent preparation for definitive airway management in standard manner
EXAMPLE OF PROCEDURE
![]() Delirious hypoxic patient not tolerating an NRB for preoxygenation
Delirious hypoxic patient not tolerating an NRB for preoxygenation
![]() Ketamine 1 to 2 mg/kg by slow intravenous push
Ketamine 1 to 2 mg/kg by slow intravenous push
![]() Preoxygenation and denitrogenation with NRB/NC or NIPPV (Non-Invasive Positive Pressure Ventilation) for 2 to 3 minutes
Preoxygenation and denitrogenation with NRB/NC or NIPPV (Non-Invasive Positive Pressure Ventilation) for 2 to 3 minutes
![]() Administer NMB (Neuromuscular blockade)
Administer NMB (Neuromuscular blockade)
![]() 45 to 60 seconds of apnea with apneic oxygenation
45 to 60 seconds of apnea with apneic oxygenation
![]() Intubate
Intubate
COMPLICATIONS
Complications from DSI are no different from complications inherent in attempts to intubate hypoxic/hypercapnic, delirious and/or otherwise unstable patients, with the exception being the establishment of a prolonged safe apnea period:
![]() Aspiration
Aspiration
![]() Gastric distention
Gastric distention
![]() Emesis with ketamine—occurs after emergence and is a concern if the patient is allowed to emerge from the dissociated state prior to endotracheal intubation
Emesis with ketamine—occurs after emergence and is a concern if the patient is allowed to emerge from the dissociated state prior to endotracheal intubation
SAFETY/QUALITY TIPS
![]() Procedural
Procedural
![]() Administering ketamine as a quick bolus will often cause 15 to 30 seconds of apnea; this can be avoided by pushing ketamine more slowly (over 30 seconds)
Administering ketamine as a quick bolus will often cause 15 to 30 seconds of apnea; this can be avoided by pushing ketamine more slowly (over 30 seconds)
![]() Application of a NC at high flow, in addition to either a face mask or NIV oxygenation, will optimize oxygenation and facilitate apneic oxygenation after the paralytic is given
Application of a NC at high flow, in addition to either a face mask or NIV oxygenation, will optimize oxygenation and facilitate apneic oxygenation after the paralytic is given
![]() Avoid very high positive pressure (>15 cm H20) when using NIV
Avoid very high positive pressure (>15 cm H20) when using NIV
![]() Cognitive
Cognitive
![]() The intubating provider should be at bedside during the entire DSI procedure, prepared to abort DSI at any point and commence with RSI (by giving the paralytic)
The intubating provider should be at bedside during the entire DSI procedure, prepared to abort DSI at any point and commence with RSI (by giving the paralytic)
![]() Although the goal of DSI is to optimize intubating conditions, in some cases, the underlying insult can be adequately addressed during the dissociated period, and intubation avoided. We recommend that a full intubation setup be prepared for every DSI case, however.
Although the goal of DSI is to optimize intubating conditions, in some cases, the underlying insult can be adequately addressed during the dissociated period, and intubation avoided. We recommend that a full intubation setup be prepared for every DSI case, however.
![]() Current alternatives to ketamine are inferior to ketamine for facilitating DSI; be cautious if using any other agent
Current alternatives to ketamine are inferior to ketamine for facilitating DSI; be cautious if using any other agent

Full access? Get Clinical Tree


