KEY POINTS
Focusing burn care in centers with an entire team dedicated to the burn patient has resulted in burn research that has led to improved physical and psychosocial outcomes, fewer complications, better pain management strategies, and shorter lengths of hospital stay.
Airway evaluation and management strategies in patients with inhalation injury and/or a large thermal injury differ from nonburn patients.
Ventilator management strategies for burn patients must include the same ventilator-associated pneumonia (VAP) bundle and the daily sedation vacation to assess readiness for extubation that is used in nonburn patients. In addition, specific assessment of airway edema must be performed.
Burn shock is a physiologic insult combining hypovolemic and distributive shock. The optimal patient outcome is provided by proper fluid resuscitation using large bore peripheral intravenous access and urine output monitored by a Foley catheter.
Prophylactic systemic antibiotic therapy does not prevent systemic infection but daily wound cleansing with soap and water followed by topical antimicrobial therapy is efficacious.
Patients with burns >20% total body surface area who have a transpyloric feeding tube placed on admission and high-protein feedings continued throughout operative procedures have better wound healing and shorter length of hospital stay.
The primary goal for wound care is wound closure. Full-thickness burns should be excised within the first 7 days, and treated with autografting if appropriate or allografting/xenografting/dermal replacement therapy if the burn size is too great for immediate autografting.
Burn pain is best treated with intravenous opioids and longer acting analgesic agents. Anxiolytics should also be used to decrease pain and for procedures such as hydrotherapy.
Rehabilitation therapy begins at admission for optimal outcomes, including positioning, splinting, early mobilization even while on the ventilator, and strengthening to promote healing.
INTRODUCTION
The goal of this review is to provide an overview of some of the most important critical care issues and approaches that are unique to burn patients when compared to the general intensive care unit population. The critically burned patient differs from other critically ill patients in many ways, the most important being the necessity of a team approach to patient care. The burn patient is best cared for in a dedicated burn center where resuscitation and monitoring concentrate on the pathophysiology of burns, inhalation injury, edema formation, and potential complications associated with burn and inhalation injuries. Early operative intervention and wound closure, metabolic interventions, early enteral nutrition, and glucose control have led to continued improvements in outcome. Prevention of complications such as hypothermia, compartment syndromes, and contractures is part of burn critical care. While expert opinion may have been the driving force behind current burn care standards and guidelines, continuing research driven by level I data is the wave of the future in the care of the burn patient.
Major strides in understanding the principles of burn care over the last half century have resulted in improved survival rates, shorter hospital stays, decreases in morbidity and mortality rates due to the development of resuscitation protocols, improved respiratory support, support of the hypermetabolic response, infection control, early burn wound closure, and early enteral nutrition.1 Complete care of the burn patient requires the participation of most disciplines in the hospital for both the inpatient as well as the outpatient follow-up care. The optimal initial management of the severely burned patient follows guidelines established and refined by the American Burn Association (ABA) over the last 20 years. It is crucial that the patient be managed properly in the early hours after injury because the initial management of a seriously burned patient can significantly affect long-term outcome. Regionalization makes it common for the initial care of the seriously burned patient to occur outside the burn center. Burns are a specialized form of trauma, therefore, the first steps in emergency care, the ABCs (airway, breathing, circulation) are the same as for the trauma patient: airway with cervical spine stabilization if appropriate, breathing, circulation, disability, and exposure. Also, the burn patient could be a victim of other associated traumas. It is easy to be sidetracked by the obvious and often dramatic thermal injury. Only after the primary and secondary surveys have been performed should the severity of the burn injury itself be evaluated. It is important to obtain as much information as possible regarding the incident and about the patient. An easy way to remember the information is the mnemonic AMPLE: allergies, medications, past medical history, last meal, and events leading up to the burn. Universal precautions appropriate for each burn patient must be implemented by every member of the health care team.2
AIRWAY MANAGEMENT
Patients at risk of requiring early intubation include those with a history of being in an enclosed space with or without facial burns, history of unconsciousness, carbonaceous sputum, hoarseness, or complaints of a “lump in the throat.” In isolation, these factors do not predict the need for intubation, but the more signs present, the more elevated the risk of requiring early intubation. Patients presenting with stridor or in respiratory distress should be intubated on presentation. A carboxyhemoglobin level taken within 1 hour after injury is strongly indicative of smoke inhalation if >10%.3 Acute upper airway obstruction occurs in 20% to 33% of hospitalized burn patients with inhalation injury and is a major hazard because of the possibility of rapid progression from mild pharyngeal edema to complete upper airway obstruction.4 If there is a significant cutaneous burn requiring resuscitation, the need for intubation will be greater. The small cross-sectional diameter of the pediatric airway places children at higher risk of requiring emergent intubation. Intubation itself is not without risk so should not be undertaken routinely simply because there are facial burns. If intubation is needed, the most experienced clinician in airway management should perform the endotracheal intubation.4 Oral intubation is the preferred route, and given the concern for upper airway edema, having more advanced airway adjuncts such as awake fiberoptic intubation, a GlideScope, and the ability to perform an emergent surgical airway (cricothyrotomy) if needed should be readily available. Given that airway edema in this emergent setting tends to be at or above the vocal cords, the use of a laryngeal mask airway (LMA) is not a useful airway management device in this setting. Tracheostomy is not an emergency procedure and should only be performed in the elective setting for airway management.
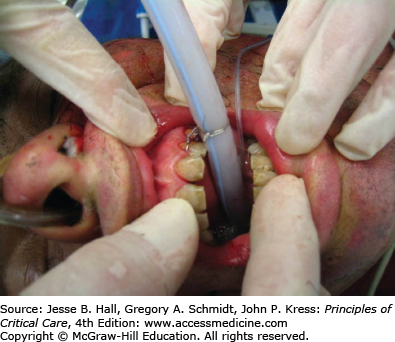
Once the patient is intubated, securing the airway is another issue that differs dramatically from other intubated patients. Most burn patients who require intubation have burns that involve the face, precluding use of the standard methods of securing the endotracheal tube. A safer method that prevents having anything in contact with the facial burns is to secure the endotracheal tube (ETT) to the teeth of the maxilla. Using 0.018-inch dental wire, secure the endotracheal tube around the base of the tube, wrapping the wire around the ETT just tight enough to indent the tube slightly without but not narrowing the tube significantly to preclude passing the suction catheter. A rubber bite block should be inserted and wired between the maxilla and mandible to prevent the patient from biting on the ETT (Fig. 123-1). If the patient is edentulous, the wire can safely be passed through the maxilla via an 18-gauge needle gently tapped through the maxilla and passing the wire through the needle. This method of securing the ETT allows care of the facial burns to be performed as needed, prevents decubitus ulcers from ties around the nasal septum, on the face, or over the ears, and allows for endotracheal suctioning and/or bronchoscopy. It also provides for a very safe airway protection method that allows the health care team to ambulate the patient while still intubated without putting the airway at risk. This patient population is one in which there cannot be inadvertent extubations, as regaining control of the airway may be impossible.
BREATHING
The care of inhalation injury largely remains supportive. Even the gold standard of bronchoscopy within the first 24 hours of admission cannot accurately predict the severity of inhalation injury, although work is in progress that grades the inhalation injury based on bronchoscopic findings for patients with inhalation injury and correlate those findings with outcomes. For patients with inhalation injury, no ideal ventilator strategy has emerged.4 According to the American College of Chest Physicians, recommendations for mechanical ventilation serve as general guidelines: Use a ventilator mode that is capable of supporting oxygenation and ventilation that the clinician has experience using, limit plateau pressures to 35 cm H2O, allow PCO2 to increase if needed to minimize plateau pressures, and use the appropriate level of positive end-expiratory pressure.5 Unless contraindicated, use of a daily sedation vacation to assess readiness to liberate from the ventilator should be performed. Roughly 70% of patients with inhalation injury will develop ventilator-associated pneumonia. Routine pneumonia prevention strategies should include elevating the head of the bed 30°, turning the patient side to side every 2 hours, oral care every 6 hours, and using endotracheal tubes with subglottic suctioning ports. Routine use of prophylaxis against gastrointestinal ulceration/bleeding raises some concern about changing the gastric pH and increasing the risk of pneumonia. However, in the critically burned patient, the risks of gastric ulceration and bleeding far outweigh the proposed concerns using stress ulcer prophylaxis, and its use is strongly recommended. Using the daily ventilator liberation protocols being used in nonburn critical care areas around the country should have the same benefits in burn critical care areas. The other assessment tool that is necessary for burn patients which may not be an issue in nonburn patients is assessing the airway patency and readiness to wean off the ventilator. The easiest and cheapest method to assess for airway patency is to briefly disconnect the patient from the ventilator, deflate the cuff on the endotracheal tube, and completely occlude the end of the ETT. If the patient is able to breathe around the occluded ETT, then the airway likely has enough space around the ETT for safe extubation. Prophylactic antibiotics have no role and actually increase infection rates. The diagnosis of pneumonia in burn patients has been described in a position paper by the ABA.6 For patients who fail to respond to maximal conventional therapy, one may consider extracorporeal membrane oxygenation (ECMO) as a rescue therapy for patients with acute hypoxemic respiratory failure who are expected to die otherwise.7 ECMO has been shown to have some success in pediatric patients with severe inhalation injuries but survival in adult burn patients is anecdotal. One problem with ECMO is that to be successful, the patient must have already undergone burn wound excision and application of xeno/allo/autografting prior to being placed on ECMO, which can last for up to 2 weeks. However, a conflicting criterion for successful ECMO is early intervention, for example, within 12 to 36 hours of burn injury.
The combination of a body burn and smoke inhalation produces a marked increase in mortality and morbidity8,9 and survival in patients >age 60 years with inhalation injury is very low.10 Burn patients with inhalation injury have been shown to require increased fluids during resuscitation.1,11-14 Navar et al15 found that the presence of inhalation injury was associated with a 44% increase in fluid requirements, which was remarkably uniform across all age groups and burn sizes. The degree of lung dysfunction caused by a smoke inhalation injury is accentuated by the presence of even a small body burn.9,14,16,17 Although it is not totally clear how much additional fluid will be required, be aware that somewhere between 40% and 70% additional fluid will be required, and resuscitation guidelines do not take inhalation injury into account.
CIRCULATION
Adequate resuscitation from burn shock is the single most important therapeutic intervention in burn treatment. Due to a paucity of evidence-based literature, burn resuscitation remains an area of clinical practice driven primarily by local custom of the treating burn units.18 The only issue exempt from debate is that fluid administration is universally advocated.13,19 Each patient will react uniquely to burn injury depending on age, depth of burn, concurrent inhalation injury, preexisting comorbidities, and associated injuries. Formulas should be regarded as a resuscitation guideline; fluid administration has to be adjusted to individual patient needs. Of the numerous formulas for fluid resuscitation, none is optimal regarding volume, composition, or infusion rate.12,20-26 Lactated Ringer solution most closely resembles normal body fluids. Factors that influence fluid requirements during resuscitation besides TBSA burn include burn depth, inhalation injury, associated injuries, age, delay in resuscitation, need for escharotomies/fasciotomies, and use of alcohol or drugs prior to injury.27
The modified Parkland formula is currently the most widely used resuscitation guideline, used in >90% of burn centers in the United States. The Advanced Burn Life Support curriculum supports the use of the Parkland formula for resuscitation in burn injury.26 Simply put, it is 4 mL/kg/percentage TBSA, this gives the amount of lactated Ringer solution required in the first 24 hours after burn injury, where kg represents the patient weight in kg, and percentage TBSA (total burn surface area) is the size of the burn injury. According to the Parkland formula, beginning at the time of burn injury, half of the fluid is given in the first 8 hours and the remaining half is given over the next 16 hours. The rapid determination of percentage TBSA burn and calculation of the fluid requirements can be difficult and often incorrect when the person treating these burns is an inexperienced clinician. The substantial errors in estimating burn extent and depth result in significant under- or overcalculation of fluid requirements.25,28-30 Most doctors outside burn centers have infrequent experience with major burn management and a relative lack of sufficient knowledge regarding such management.3,17,25,29 Even among burn center physicians, there is considerable variability in determining the amount of fluids to be administered during the resuscitation period.
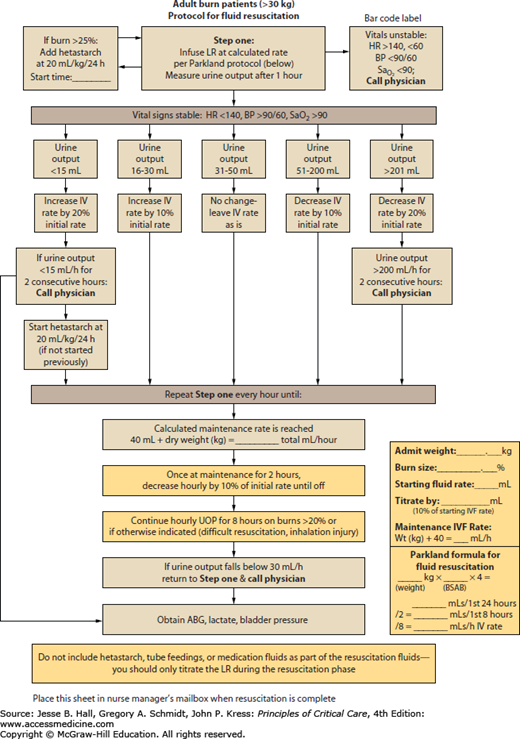
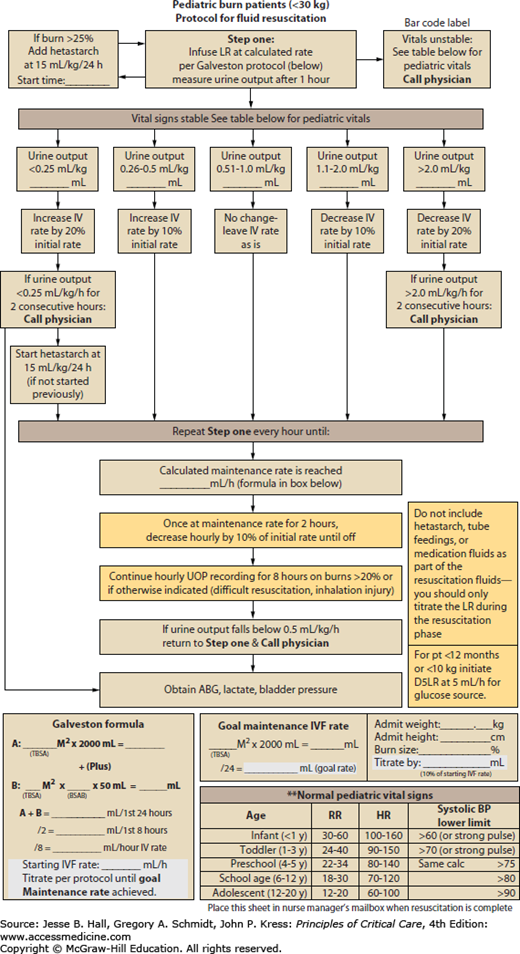
Outside of a computer generated and controlled resuscitation formula currently being investigated by military burn surgeons, the best resuscitation guideline is one that provides the optimal resuscitation and the least opportunity for disaster by the inexperienced clinician. The attached resuscitation guides have been successfully used in the 16-bed burn center at the University of Iowa (Fig. 123-2). The adult protocol utilizes a weight-based approach, with urine output and vital signs being monitored every hour during the resuscitation period. The pediatric protocol also utilizes a weight-based approach, adding glucose containing maintenance fluids for the child <30 kg (Fig. 123-3). These protocols have allowed us to use a protocol that provides adequate resuscitation but avoids overresuscitation and the attendant complications.
A clinical advantage with colloid administration during the resuscitation phase has not been identified.22,24,31 One study showed a decreased risk of death when albumin was used during resuscitation,18 but the difference did not achieve statistical significance. A meta-analysis comparing albumin to crystalloid showed a 2.4-fold increased risk of death with albumin.32 Hypertonic saline has also had disappointing results, with a fourfold increase in renal failure and twice the mortality of patients given lactated Ringer solution.33 Hypertonic saline does not routinely have a place in burn resuscitation.19 Fresh frozen plasma should not be used as a volume expander, according to new policies on blood product delivery.32 Due to the risk of blood-borne infectious transmission,22 the American Burn Association Practice Guidelines for Burn Shock Resuscitation do not recommend the use of fresh frozen plasma without active bleeding or coagulopathy outside of a clinical trial, when other choices are available.21 Depletion of limited blood bank reserves is another deterrent to using fresh frozen plasma in burn resuscitation.22 During resuscitation, development of unstable vital signs, inadequate response to fluids, or persistently high fluid requirements should prompt a call to an experienced burn care physician as noted in both adult and pediatric resuscitation protocols.
It is not possible to accurately predict who will fail resuscitation, but patients who routinely require additional fluids include those with inhalation injury, electrical burns, those in whom resuscitation is delayed, and those using alcohol or illicit drugs.34 Patients making methamphetamine have been found to be injured more seriously with larger, deeper burns43 and often require two to three times the standard Parkland formula resuscitation.35,36 There is significantly increased inhalation injury, nosocomial pneumonia, respiratory failure, and sepsis in this patient population.35,36
RESUSCITATION GOALS
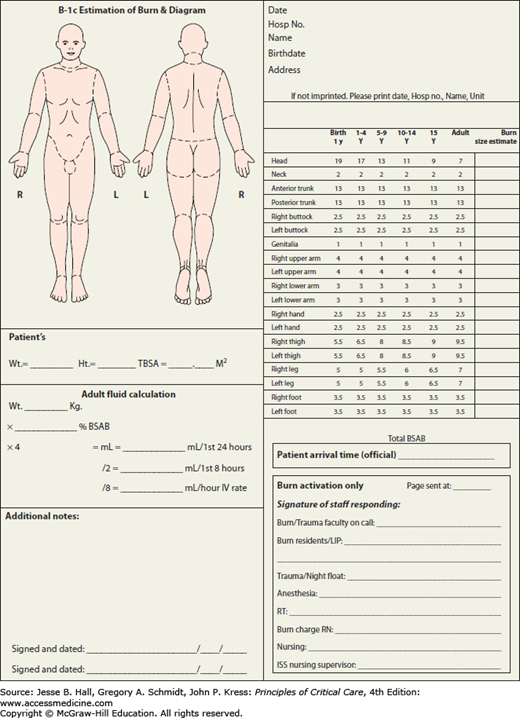
Effective fluid resuscitation is one of the cornerstones of modern burn care and perhaps the advance that has most directly improved patient survival. Proper fluid resuscitation aims to anticipate and to prevent rather than to treat burn shock.3,20,21 Resuscitation of burn shock cannot hope to achieve complete normalization of physiologic variables because the burn injury itself leads to ongoing cellular and hormonal responses. However, moving the patient toward a normal burned physiologic status during the resuscitation period is an appropriate goal. The obvious challenge is to provide enough fluid replacement to maintain perfusion without causing fluid overload.3,11,12,22-25,37-43 Without effective and rapid intervention, hypovolemia/shock will develop if the burns involve 15% to 20% TBSA.28 Delay in fluid resuscitation beyond 2 hours of the burn injury complicates resuscitation and increases mortality.37,43 The consequences of excessive resuscitation and fluid overload are as deleterious as those of underresuscitation: pulmonary edema, myocardial edema, conversion of superficial into deep burns, the need for fasciotomies in unburned limbs, and abdominal compartment syndrome.18,19,22,44,45 A Lund-Browder chart should be completed at the time of admission to calculate the TBSA burn (Fig. 123-4).
BURN SHOCK PATHOPHYSIOLOGY
Burn shock is a unique combination of distributive and hypovolemic shock16,19,22,32,46,47 manifested by intravascular volume depletion, low pulmonary artery occlusion pressures, elevated systemic vascular resistance, and depressed cardiac output.46,48 Reduced cardiac output is a combined result of decreased plasma volume, increased afterload, and decreased contractility.21 Studies suggest that impaired myocardial contractility is likely caused by circulating mediators such as tumor necrosis factor-α49,50; however impaired Ca+2 at the cellular level is most likely involved as well.51 The exact mechanisms of altered cardiac mechanical function remain unclear and are most likely multifactorial.22,51,52 Virtually all components that control fluid and protein loss from the vascular space are altered after a burn.16 Immediately after burn injury, the systemic microcirculation loses its vessel wall integrity and proteins are lost into the interstitium.22,25,26 This protein loss causes the intravascular colloid osmotic pressure to drop precipitously and allows fluid to escape from the circulatory system.22,26 There is a marked transient decrease in interstitial pressure caused by the release of osmotically active particles, causing a vacuum effect that sucks in fluid from the plasma space. There is a marked increase in fluid flux into the interstitium caused by a combination of the sudden decrease in interstitial pressure, an increase in capillary permeability to protein, and a further imbalance in hydrostatic and oncotic forces favoring the fluid movement into the interstitium.16 The outcome is a dramatic outpouring of fluids, electrolytes, and proteins into the interstitium with rapid equilibrium of intravascular and interstitial compartments.25 These changes are reflected in loss of circulating plasma volume, hemoconcentration, massive edema formation, decreased urine output, and depressed cardiovascular function.46 What actually changes is the volume of each fluid compartment, with intracellular and interstitial volumes increasing at the expense of plasma and blood volume.25 Functional plasma volume in burn tissue can be restored only with expansion of the extracellular space.53 Most edema occurs locally at the burn site and is maximal at around 24 hours postinjury.16,22,25,27,28,42,53 The rate and extent of edema formation in major burn injury far exceed the intended beneficial effect of inflammatory system activation.16,45 The edema itself results in tissue hypoxia and increased tissue pressure with circumferential injuries. Aggressive fluid therapy can correct the hypovolemia but will accentuate the edema process.16,17,45,54
FIRST-LINE MONITORING
Although urine output and heart rate are the primary modalities for monitoring, the current standards for monitoring fluid therapy in patients with large burns are not necessarily supported by data.12,13,24,55
Related posts:






Full access? Get Clinical Tree


