CHAPTER 13 Wound local anesthetic infusions
Crile, a surgeon from Cleveland, USA, was the first to describe, in 1913, the benefit of local anesthesia application to the surgical wound in providing analgesia and decreasing morbidity and mortality. Capelle, in 1935, described the use of an infusion apparatus to deliver local anesthesia to the wound.1 In 1950, Blades and Ford used a fine catheter to deliver local anesthetic to thoracotomy wounds.
Over the past 20 years, numerous papers have reported the use of local anesthesia in wounds of major abdominal incisions, gynecological and obstetric procedures, orthopedic operations, plastics procedures and mastectomy, among others. These studies have confirmed a decrease in pain scores at rest and during activity. They have, in addition, been associated with a decreased incidence of side-effects.2
Rationale for using local anesthetic infusion
Postoperative pain arises from the interaction of three factors:
Local anesthetics can be used peri-operatively to affect all three of the above.4 In addition, because these systems are relatively simple to use they can and have been used in the home setting postoperatively.5
Potential problems
It would appear that local anesthetic infusions have very few side-effects and as a result their risk–benefit ratio is positive.2
Positioning
The fact that surgeons place catheters has the added advantage of making them more aware of postoperative pain and empowering them to assist its palliation. Postoperative pain has up to recently not been seen as a complication in surgical terms. The incidence of post-surgical chronic pain is higher than many surgeons appear to realize.6
Orthopedic procedures
Shoulder surgery
Arthroscopic surgery
Wound catheter techniques decrease opioid requirements without significant side-effects.
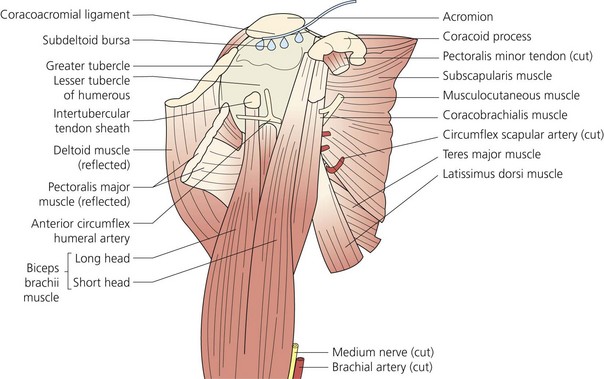
Subacromial catheter placement is recommended (Fig. 13.1) but intra-articular catheters have also been used. A flow rate of 2–5 mL/hr is adequate.
< div class='tao-gold-member'>







Full access? Get Clinical Tree


