CHAPTER 20 Midhumeral block
Surface anatomy
The main landmarks for the midhumeral block include the junction between the upper one-third and lower two-thirds of the humerus and the brachial artery. This can be approximated as three fingers’ breadth below the anterior axillary fold (Fig. 20.1).

Sonoanatomy
Ultrasound examinations of the brachial plexus through the humeral canal show that ulnar and median nerves are located superficially under the skin. The radial nerve, located beside the humerus, is the most dorsally located nerve of the plexus. The musculocutaneous nerve is situated midway between these two nerves. Images obtained from ultrasound examinations of the brachial plexus through the humeral canal can be illustrated on a graphical synthesis and can be divided into two compartments (Fig. 20.2). A superficial and a dorsal nerve can be found within each compartment. Median and musculocutaneous nerves are located inside the cephalic compartment, whereas the musculocutaneous nerve is located dorsally. Ulnar and radial nerves are located inside the caudal compartment; the radial nerve is located dorsally.
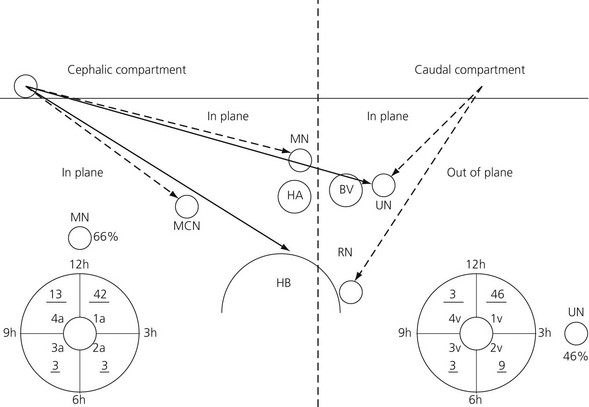
Figure 20.2 Graphical synthesis of the brachial plexus at the level of the humeral canal under ultrasound description. RN: radial nerve; UN: ulnar nerve: MCN: musculocutaneous nerve: MN: median nerve: HA: humeral artery: BV: basilic vein: HB: humerus. The dotted line separates the caudal compartment from the cephalic compartment. The underlined numbers correspond to volunteers. The MN is between 12 and 1 o’clock in 66% of the cases. The UN is situated at the 3 o’clock position in 46% of the cases. The UN and the RN cannot be blocked from a single point of puncture located on the cephalic side of the probe (long line arrows). The 2 points of puncture inside the 2 compartments are mandatory (broken line arrows).1
Technique
Landmark-based approach
The patient is placed supine and the arm abducted at 90°. At the junction between the upper and middle thirds of the arm, a line is drawn over the brachial artery. The needle insertion point is infiltrated with local anesthetic using a 25-G needle. A 50-mm 22-G insulated needle connected to a peripheral nerve stimulator is inserted almost tangentially to the skin, between the brachial artery and the palpating finger, in the direction of the axilla, in order to locate the median nerve (Fig. 20.3). The stimulating current is set at 1.0 mA, 2 Hz, and 0.1 ms. The needle is advanced slowly until the appropriate muscle response is obtained. The needle position is adjusted while decreasing the current to 0.35 mA with maintenance of the muscle response. Stimulation of the median nerve will produce contraction of the flexor carpi radialis and flexor digitorum superficialis of the fingers. Incremental injections of local anesthetic (6–8 mL) are made with repeated aspiration.
< div class='tao-gold-member'>








Full access? Get Clinical Tree


