CHAPTER 9 Which block for which surgery?
Introduction
A recent editorial highlighted that ‘Regional anesthesia always works, provided we put the right dose of the right drug in the right place’.1 Locating the right place is key to providing a successful block. With recent developments in peripheral nerve blockade this has become easier. We now have high quality peripheral nerve stimulators in addition to portable ultrasound technology to aid us in nerve location.2–4 While accurate nerve location is key to successful peripheral nerve blockade, equally important is choosing an appropriate block for the planned surgery. This can only be obtained by discussing and understanding the planned surgery with the surgeon. With central neuraxial blockade we are aware that a low lumbar epidural would be of limited benefit for upper abdominal surgery, a thoracic epidural being of more benefit. Similarly, for wrist surgery, accepting ulnar nerve stimulation for an axillary block may be of limited benefit, if the surgical incision is on the dorsum of the wrist, where it would have been better to identify the radial nerve either with nerve stimulation or ultrasound, in addition to blocking other branches of the brachial plexus. Hence, it is not only important to block the correct plexus, but equally important to consider and ensure we block the necessary nerve branches for the surgical procedure. It is therefore essential that anesthetists have a comprehensive knowledge of applied anatomy for regional anesthesia.
Utilization of regional anesthesia has increased hugely over the last 20 years, with a recent study suggesting that it is now used in 37% of surgical cases amenable to a regional technique.5 This is likely to increase further in coming years. In recent years, we have seen a large number of peripheral nerve blocks described in the literature, with several descriptions for each approach for a given nerve block. Thankfully, the introduction of ultrasound has somewhat simplified this. While the ability to perform a wide variety of peripheral nerve blocks is desirable for successful regional anesthesia, the majority of regional anesthesiologists use only a limited number of blocks regularly. In addition, their block choice may also depend on the nerve location technique they use. For example, when performing brachial plexus anesthesia above the clavicle using nerve stimulation, many regional anesthesiologists will use an interscalene approach, while if they use ultrasound they may opt for an ultrasound guided supraclavicular approach. With experience, the anesthetist will be able to select the most appropriate technique (or combination of techniques) in addition to making the regional anesthesia technique work.
Applied anatomy
A thorough understanding of anatomy relevant to regional anesthesia is essential if it is to be performed with precision and accuracy and to avoid complications. While the exact location of nerves is important, the surrounding tissues and fascial planes are equally important, as the local anesthetic is placed in close proximity to the nerves. Traditionally, doctors have focused particularly on dermatomes, in addition to osteotomes and myotomes, when performing regional anesthetic techniques (Ch. 4). However, with peripheral nerve blocks it is more useful to think what nerve branches supply the surgical site and to ensure that we block these nerves.
Upper limb peripheral nerve blocks
The upper limb is supplied by nerves of the brachial plexus. The brachial plexus is formed by the anterior primary rami of the lower four cervical nerves (C5–C8) and the first thoracic nerve (T1).6,7 In some individuals there may also be contributions from the C4 and T2 nerve roots. The plexus supplies motor innervation to all the muscles of the upper limb with the exception of the trapezius and levator scapula muscles. It supplies cutaneous innervation to the upper limb with the exception of the area of the axilla (upper inner arm), which is supplied by the intercostobrachial nerve. Above the shoulder is supplied by the supraclavicular nerve (cervical plexus), and the dorsal scapular area is supplied by cutaneous branches of spinal nerves. The plexus has five terminal branches (median, ulnar, radial, musculocutaneous and axillary nerves) in addition to a number of smaller branches. The innervations of the major joints of the upper limb are highlighted in Table 9.1. A more detailed description of upper limb anatomy can be found in Chapter 14. It is possible to block the brachial plexus at various levels as it leaves the intervertebral foramina and traverses towards the periphery. The most proximal approach at the level of the nerve roots is the interscalene approach; the supraclavicular block is performed at the level of the trunks, while the infraclavicular block is performed at the level of the cords, with axillary approach at the level of the terminal branches. All of these blocks can be successfully performed with either nerve stimulation or with ultrasound guided techniques (Ch. 7).2–4
Table 9.1 Innervations of the major joints of the upper limb
| Acromioclavicular joint | Suprascapular, axillary and lateral pectoral nerves |
| Shoulder joint | Suprascapular, axillary and lateral pectoral nerves |
| Elbow joint | Musculocutaneous, radial, ulnar and median nerves |
| Wrist joint | Radial, ulnar and median nerves |
Notes: Median, ulnar, radial, musculocutaneous and axillary nerves are five terminal branches of the brachial plexus. The suprascapular nerve is a branch from the upper trunk while the lateral pectoral nerve is a branch from the lateral cord of the brachial plexus.
The interscalene approach is suitable for surgeries of the shoulder and upper arm, and can be performed with the arm in almost any position. It blocks the plexus close to the nerve roots at about the level of the cricoids cartilage (C6).6 This may help explain why there is less spread to the lower roots, resulting in poor block of the ulnar nerve (C8, T1). The posterior shoulder will not be anesthetized, requiring wound infiltration for the port site for shoulder arthroscopies. Equally, the anterior port for arthroscopy may also be missed because the skin is supplied by T2. A supplemental skin infiltration needs to be made over the distribution of T2 to ensure the anterior port or the lower end of a total shoulder incision is adequately anesthetized. The phrenic nerve is paralyzed with this approach as it lies on the anterior scalene muscle, so caution should be exercised in patients with severe respiratory co-morbidities. In addition, patients may develop hoarseness and ptosis. This is a superficial block and complications are rare. However, serious complications have been reported with this block, including spinal cord injury, vascular injection and pneumothorax.8
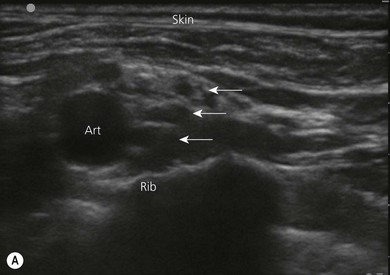
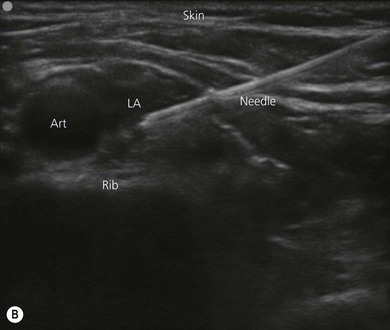
The supraclavicular approach is suitable for surgeries of the upper arm, elbow and hand, and is performed at the level of the trunks of the brachial plexus. It is frequently referred to as the spinal anesthetic of the upper limb as it can provide complete anesthesia of the limb below the shoulder in a consistent time-efficient manner. In the past, some anesthetists were cautious about performing this block because of the rare complication of pneumothorax, and the fact that the landmarks were not easy to ascertain, particularly in obese patients. However, the advent of ultrasound has resulted in a huge increase in the utilization of this block, where the plexus can be seen lying posterior and lateral to the subclavian artery on the first rib (Fig. 9.1). Local anesthetic can be preferentially injected around the lower trunk (C8, T1) of the plexus, particularly when used for hand surgery. Use of this block may still result in phrenic nerve paralysis (50%) and Horner’s syndrome.6 Placement of a continuous catheter at this site (supraclavicular fossa) for post operative analgesia is easy to secure and less likely to become dislodged (Fig. 9.2).


The axillary approach to the brachial plexus anesthetizes the terminal branches of the plexus, as they lie in close proximity to the axillary artery.6 It is ideal for surgeries below the elbow, particularly hand surgery. This block is safe and easy to perform and is therefore widely used. The anesthetist needs to be aware that there are multiple vessels (arteries and veins) in close proximity to the nerves and care should be taken to avoid intravascular injection. A single injection technique is associated with a significant failure, therefore a multiple injection technique should be used or the block performed under ultrasound guidance to ensure adequate spread of local anesthetic9 (Fig. 9.3). The musculocutaneous nerve lies between the biceps and coracobrachialis muscle and may be some distance away from the other branches of the plexus which lie close to the artery. It is critical to block the musculocutaneous nerve, as it supplies the flexor muscles of the arm and the skin over the lateral surface of the forearm.

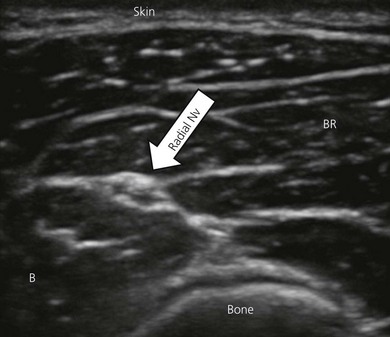
The utilization of elbow and forearm blocks is discussed in Chapters 21 and 22. These blocks are easy to perform, particularly when ultrasound guidance is used (Fig. 9.4). These techniques are useful both as the primary anesthetic, and also for postoperative analgesia. Consideration should be given as to whether the surgeon is using a tourniquet and in what location. Upper arm tourniquets can be used for short periods of time, but longer use will require anesthesia of the tourniquet location. In such cases, a distal forearm or elbow block performed with a long acting local anesthetic (to provide postoperative analgesia) can be used in combination with a more proximal block such as infraclavicular or axillary block, using a shorter-acting local anesthetic (lignocaine). The more distal block should be performed first to minimize the risk of unrecognized intraneural injection. These blocks are also frequently used as ‘rescue’ blocks, where following a more proximal block there is incomplete anesthesia in a branch of the plexus. This branch can then be blocked at the elbow or forearm. Again, caution should be exercised, as rescue blocks may be associated with a higher incidence of nerve injury.
The intercostobrachial nerve (T2) supplies the area of the axilla (upper inner arm) which is important for certain upper arm procedures. In addition, this is where an upper arm tourniquet is typically located. While tourniquet pain is largely related to muscle ischemia, anesthetizing the skin in this area will improve patient comfort. This is easily achieved using subcutaneous infiltration of local anesthetic around the medial aspect of the upper arm (Fig. 9.5). The supraclavicular nerve block (cervical plexus) can be performed by injecting local anesthetic along the posterior border of the sternocleidomastoid muscle (Ch. 11).
< div class='tao-gold-member'>








Full access? Get Clinical Tree


