Initial resuscitation.
Identification, where possible, of likely agent.
Specific treatments or antidotes.
General supportive measures.
Pharmaceutical products including ‘over-the-counter medications’:
E.g. paracetamol (and paracetamol-containing products), aspirin (and other analgesics/NSAIDs), opiates/opioids, benzodiazepines and ‘Z-drugs’ (e.g. zopiclone), antidepressants (including SSRIs and tricyclics), and barbiturates
Recreational drugs (including alcohol, the most common drug to be co-ingested either with recreational drugs or as part of self-poisoning):
Industrial chemicals, household chemicals, and environmental toxins including inhaled poisons (e.g. carbon monoxide and cyanide):
E.g. organophosphates, paraquat, methanol, ethylene glycol, household products (e.g. batteries, cleaning agents and detergents)
Animal, fish, and insect bites/stings.
A history of attempted suicide, psychiatric illness, or substance abuse.
Airway or respiratory signs and symptoms:
Respiratory depression
Aspiration, pneumonitis, or bronchospasm
Oropharyngeal burns
Cardiovascular:
Hypotension, hypertension, cardiovascular collapse, cardiac arrest
ECG: tricyclics and antidepressants, amongst other drugs, cause conduction defects and arrhythmias, which may be resistant to treatment
Neurological:
Agitation, confusion, or hallucinations
Unexplained unconsciousness, especially if associated with compartment syndrome or prolonged contact burns
Convulsions
Profound weakness, or conversely muscle rigidity or dystonia
Ataxia or nystagmus
GI: vomiting or diarrhoea; liver failure.
Renal: renal failure, rhabdomyolysis.
Hypo- or hyperthermia.
Self-harm injuries.
Trauma, burns, drowning, and head injuries.
Electrolyte imbalance, especially sodium, potassium, or glucose.
Metabolic acidosis, especially with a raised osmolar or anion gap (see p.205).
p.205).
ABGs (hypoxia, hypercapnia, metabolic acidosis, raised anion gap).
FBC, coagulation studies (coagulation may be deranged).
Blood methaemaglobin concentration (see p.453).
p.453).
RBC cholinesterase activity (in organophosphate poisoning).
Serum calcium (in ethylene glycol poisoning) and phosphate.
Serum CK (raised in rhabdomyolysis).
Serum glucose.
Blood alcohol levels (or expired air levels if possible).
Paracetamol and salicylate levels (important to check timings).
Specific drug serum levels may be indicated for other substances (e.g. ethylene glycol, digoxin, valproic acid, phenytoin, theophylline, iron, lithium, carbamazepine).
Carboxyhaemoglobin (by co-oximetry).
Urine for myoglobin.
Consider taking blood, urine, and gastric aspirate samples for toxicology, or for storage in case later analysis is required.
12-lead ECG (may show ischaemia, evidence of hyperkalaemia or QT prolongation).
CXR (if aspiration suspected or prior to hyperbaric oxygen therapy).
AXR may be useful if ingestion of radiopaque substances is suspected (chloral hydrate, heavy metals, iron, enteric coated or sustained release preparations, ‘body packing’).
Conditions causing altered consciousness, altered behaviour, or respiratory depression (e.g. head injuries, meningitis/encephalitis, hypoglycaemia and post-ictal state).
Conditions causing cardiovascular collapse (e.g. anaphylaxis).
Conditions causing muscle weakness (e.g. Guillain-Barré and botulism)
Conditions causing non-specific symptoms such as vomiting or hypothermia (e.g. infections/sepsis, neurological injury/SAH).
Table 14.1 Cardiorespiratory changes and associated poisons | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 14.2 Temperature, skin, and oral changes | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 14.3 Neurological and eye changes | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 14.4 Gastrointestinal and renal changes | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 14.5 Toxidromes and combinations of symptoms and the likely associated poisons | |||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
History from patient, family, other witnesses, or paramedics.
History of repeat prescriptions from GP.
Examination of patient for signs associated with certain drugs.
Examination of pill bottles or tablets; a pill identification system such as the computer-aided tablet and capsule identification program (TICTAC) may be required.
Endotracheal intubation may be required if the following is present:
Hypoxia
Diminished consciousnes (GCS ≤9, or rapidly deteriorating)
The patient is at risk of aspiration
The patient is agitated, or combative and not mentally competent
Any corrosive substances have been ingested
Ensure ventilation is adequate, use mechanical ventilation if necessary:
Respiratory stimulants are unhelpful
In conditions where there is extreme acidosis it may be appropriate to hyperventilate the patient for a short period
Fluid loading may be required to treat hypotension:
Tachypnoea, sweating, and prolonged unconsciousness can lead to fluid depletion
Inotropes are occasionally required, but may interact with overdoses of cardiovascular drugs; where there is doubt discuss their use with an expert in poisonings
Hypotension may be the result of arrhythmias requiring treatment; treat any cardiac arrhythmias and conduction defects which may compromise the circulation (see p.132 and 138).
p.132 and 138).
Correction of hypoxia, acidosis (both metabolic and respiratory), and electrolytes will be required
Where tricyclic antidepressants are involved a bolus of 50-100 ml sodium bicarbonate 8.4% IV may help
Where drugs have prolonged the QT interval resulting in torsade de pointes, it may be treated with magnesium sulphate 8 mmol (2 g) in 100 ml 5% glucose IV over 2-5 minutes followed by an infusion of 2-4 mmol/hour (0.5-1 g/hour) (10 mmol) and potassium supplementation (40 mmol in 100 ml 5% dextrose over 1-4 hours via a central line aiming for a plasma concentration of 4.5-5.0 mmol/L)
Profound bradycardia may be caused by certain agents, and may be unresponsive to drug therapy, requiring:
Early transvenous or transcutaneous pacing
Chemical pacing with adrenaline or isoprenaline
β-blocker toxicity may require treatment with glucagon 2-10 mg IV/IM, and calcium channel antagonist toxicity may require calcium chloride 10 ml 10% IV; additional treatment for bradycardia and/or hypotension may also be necessary (see pp.104 and 132)
pp.104 and 132)
In digoxin overdose treatment with Fab fragments may help
Hypertension can occur with some drugs, particularly amphetamines and cocaine- hypotensive agents may be required.
Convulsions are mostly brief and non-sustained; where status epilepticus occurs first-line treatment is with a short-acting benzodiazepine such as lorazepam 4 mg IV (see p.160):
p.160):
Be aware that many patients will have taken benzodiazepines as part of their overdose ‘cocktail’
Dystonic reactions can occur and may require treatment with procyclidine 5-10 mg IV.
50-100 g PO of activated charcoal can be used if patients have ingested a potentially toxic dose of a poison within the past 1 hour:
Activated charcoal is contraindicated in patients at risk of aspiration, e.g. patients with ↓consciousness or after hydrocarbon ingestion; it is also relatively contraindicated in patients at risk of GI bleeding or perforation
In patients with diminished consciousness, charcoal can be safely delivered via a NGT if the airway is protected by cuffed ETT and the NGT position has been positively confirmed
It is ineffective against alcohols, solvents, metal salts (e.g. iron and lithium), petroleum distillates, DDT, and malathion
Do not give alongside an oral antidote
Multiple-dose activated charcoal may be used for certain drugs, (phenobarbital, carbamazepine, dapsone, quinine, and theophylline) at a rate not less than 12.5 g/hour.
Gastric lavage is not routinely recommended. It should only ever be considered in case of extreme risk from recent ingestion (<1 hour) of very toxic substances:
It is contraindicated in patients at risk of aspiration, and if corrosive substances or hydrocarbons (e.g. petrol) have been ingested due to the risk of gut perforation or pneumonitis
Forced emesis (e.g. with ipecacuanha) is no longer recommended.
Look for and treat causes of agitation, e.g. hypoxia or full bladder.
Sedation may be required in profoundly agitated patients, but may provoke a drop in consciousness requiring endotracheal intubation; sedation may also worsen any hypotension.
Antipsychotics are sometimes used to treat agitation, but may lower the seizure threshold.
Hypothermia is common following prolonged unconsciousness; or it can occur as a result of certain drugs (classically barbiturates).
 p.250
p.250 p.132
p.132
Hyperthermia is associated with stimulants, neuroleptic and antimuscarinic drugs; cooling and specific antihyperthermic therapy may be required ( p.248).
p.248).
Catheterization and urine output measurements may be required.
Regular blood sugar measurements may be required in order to monitor/treat any hypoglycaemia.
Invasive monitoring and continuous ECG monitoring are required for many poisonings and overdoses.
Antidotes or treatments may be available for certain drugs and chemicals (see Table 14.6).
Haemodialysis or haemoperfusion may be useful in the removal of certain toxins (see p.457).
p.457).
Urinary alkalinization (often known as forced alkaline diuresis) using sodium bicarbonate can be used to encourage the renal excretion of specific acidic drugs (moderately severe aspirin/salicylate overdoses not requiring haemodialysis; 2,4-dichlorophenoxyacetic acid and chlorphenoxy herbicides; mecoprop):
Different regimens exist for achieving urinary alkalinization, an example is the infusion of 1000 ml 1.4% sodium bicarbonate in
water solution over 2.5 hours; urine should be tested to ensure a pH of 7.8-8.5
Urinary alkalinization may also be of benefit in methotrexate, fluoride, or diflunisal poisoning, although the evidence for this is not clear
It is not recommended for phenobarbital (multiple-dose activated charcoal is superior), or chlorpropamide (supportive care with glucose infusion mostly adequate)
It is associated with hypokalaemia and alkalotic tetany (electrolytes should be monitored and replaced)
It is relatively contraindicated in patients with incipient renal failure or significant pre-existing heart disease
Urinary acidification has previously been considered for drugs such as amphetamines, quinine, and phencyclidine, but is generally not recommended because of associated complications.
Whole bowel irrigation using balanced polyethylene glycol electrolyte solution (1500-2000 ml/hour NG) to promote bowel transit and liquefy stool has only limited evidence of effectiveness, but has been used in the following circumstances:
For sustained release drug preparations, and drugs not absorbed by charcoal (e.g. iron and lithium)
For ‘body-packers’ (drug couriers who have ingested packages/condoms filled with drugs)
Contraindications include: unprotected airway; bowel perforation, obstruction, or haemorrhage; haemodynamic instability
Table 14.6 Specific antidotes and treatments | ||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||
 p.493
p.493
If a deliberate release of toxic agents, or a mass poisoning event, is suspected follow the guidelines on p.496.
p.496.
Accidental or deliberate self-poisoning is commonly associated with other injuries, including trauma.
The use of multiple agents is common in self-poisoning, and signs and symptoms are often a mixture of those caused by various drugs.
The combination of stimulant and sedatives (particularly GHB) taken together can result in profound fluctuations in consciousness.
Where there is any doubt as to the aetiology of ↓consciousness or seizures a CT scan is indicated:
Alcohol is associated with head trauma and intracranial bleeding
Paracetamol and salicylate are extremely common ingredients in overdose ‘cocktails’, check plasma levels for these agents in cases of self-poisoning, even if there is no evidence of ingestion.
Prior to blood levels being available, or where no blood tests exist, treatment can be based upon the calculated maximum dose (e.g. if all the available pill bottles were full at the time of ingestion).
Blood levels of toxins taken soon after ingestion may be falsely low.
Identification of tablets, plants, or snakes brought in to hospital is often wrong, expert advice may be required either via direct contact or via programs such as TICTAC.
Activated charcoal may sometimes be of use in cases where ingestion took place >1 hour prior to admission, or where the timing of ingestion is unknown; where there is doubt discuss the case with a poisons expert.
‘Body-packers’ (drug couriers who have ingested packages filled with drugs), require a surgical referral, treatment will depend upon the risks posed by the drug(s) involved and their position within the GI tract.
Self-poisoning requires appropriate evaluation of any future suicide risk; ideally this should be arranged prior to ICU discharge.
Deaths from poisoning should be reported to the coroner.
Most patients will cooperate with treatment though some, particularly those who have attempted suicide, may refuse it:
Patients who are mentally competent have the right to refuse any, and all, treatment, even if they risk death in doing so
Mental competency requires the ability to understand, retain, believe and evaluate information
Life-saving treatments may be administered to patients against their will only if they are not mentally competent and have no legally binding advance directive.
When in doubt ask for senior advice or psychiatric advice early.
Carefully document any refusal of treatment, or any treatment against a patient’s wishes.
 <http://tictac.vhn.net/home/>.
<http://tictac.vhn.net/home/>. <http://www.spib.axl.co.uk/>.
<http://www.spib.axl.co.uk/>.
Paracetamol poisoning occurs when healthy individuals take moderate to large overdoses (10 g/20 tablets or 150 mg/kg within 24 hours).
Certain patients have depleted stores of glutathione and are susceptible to hepatotoxicity at much lower doses, including:
Malnourished: anorexia, alcoholism, HIV
Taking enzyme inducing drugs: carbamazepine, phenobarbital, phenytoin, primidone, rifampicin, St John’s wort
In rare cases in high-risk individuals, poisoning may occur at normal doses administered over a prolonged time.
Initial presentation is mostly asymptomatic unless other agents are also involved, although nausea and vomiting may occur.
In exceptionally high overdoses (>5000 µmol/L or 800 mg/L) acute deterioration in GCS may occur accompanied by lactic acidosis.
Delayed presentation (12 hours-4 days) can be accompanied by RUQ pain with liver and/or renal failure.
Liver damage is maximal at 4 days after the overdose, and may result in encephalopathy, cerebral oedema, haemorrhage, and hypoglycaemia.
 p.449.)
p.449.)
ABGs, if compromised (acidaemia).
Serum glucose (hypoglycaemia may occur).
Serum paracetamol levels (at 4 hours post ingestion if possible).
 p.454.)
p.454.)
Give O2 and support airway, breathing, and circulation as required.
Treatment is guided by plasma levels taken >4 hours after ingestion, levels (earlier levels are misleading); high-risk patients require treatment at lower plasma levels (see Fig. 14.1).
If history is suggestive of an overdose in the past 36 hours requiring treatment then commence IV N-acetylcysteine whilst awaiting levels.
Methionine can be given if poisoning is <12 hours with no vomiting
IV N-acetylcysteine (best started <8 hours after ingestion):
150 mg/kg IV (diluted in 5% glucose) over 15 minutes, then
50 mg/kg IV (diluted in 5% glucose) over 4 hours, then
100 mg/kg IV (diluted in 5% glucose) over 16 hours
Discontinue if overdose occurred <8 hours ago and serum paracetamol levels are under treatment levels, or
Overdose occurred >8 hours ago (or was staggered), serum paracetamol levels are under treatment levels, and AST normal.
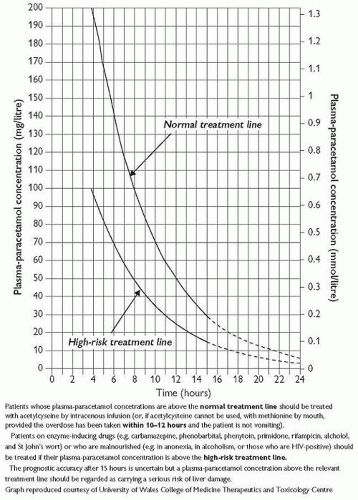 Fig. 14.1 Paracetamol poisoning nomogram. Patients whose plasma-paracetamol concentrations are above the normal treatment line should be treated with acetylcysteine by IV infusion (or, if acetylcysteine cannot be used, with methionine by mouth, provided the overdose has been taken within 10-12 hours and the patient is not vomiting). |
Those taking liver-enzyme-inducing drugs (e.g. carbamazepine, phenobarbital, phenytoin, primidone, rifampicin, efavirenz, nevirapine, alcohol, St John’s wort).
Those who are malnourished (e.g. anorexia or bulimia, cystic fibrosis, hepatitis C, in alcoholism, or those who are HIV positive); or who have not eaten for a few days.
 p.456
p.456
Medications may contain co-drugs needing treatment, in particular co-proxamol (available but no longer licensed).
Aspirin ingestion.
Salicylic acid ingestion.
Oil of wintergreen.



