Fig. 15.1
Denver Health Medical Center (DHMC) algorithm for the management of hemodynamically unstable patients with mechanically unstable pelvic fractures (ATLS Advanced Trauma Life Support, CXR chest radiograph, FAST focused abdominal sonographic examination for trauma, ED emergency department, REBOA resuscitative endovascular balloon occlusion of the aorta, OR operating room)
Resuscitative Endovascular Balloon Occlusion
Currently, there is mixed opinion as to the sequence of therapies and optimal timing of adjunctive maneuvers while transfusing patients presenting in refractory shock with a severe pelvic fracture . Arguably the most significant development in modern vascular surgery is the emergence of endovascular techniques for managing vascular disease, and these techniques are now being extended to traumatic injuries. Although initially applied to injuries for which open repair was highly morbid (thoracic aorta) or provided limited exposure (distal carotid, subclavian artery), endovascular techniques for temporizing acute control of hemorrhage or as definitive management can be applied to a wide array of arterial injury patterns [6–9]. A national analysis demonstrated a 27-fold increase in the use of endovascular therapy, and this was associated with a decrease in morbidity, hospital stay, and mortality [10]. Technical success of these procedures is 90–100% and provides a definitive, minimally invasive treatment option [11]. Resuscitative endovascular balloon occlusion of the aorta (REBOA) has recently emerged as a viable adjunct in the management of patients with non-compressible torso hemorrhage (NCTH) [6, 7]. This intervention is less invasive and may effectively increase central blood pressure (cardiac and cerebral perfusion) and control active pelvic bleeding, potentially obviating the need for resuscitative thoracotomy.
Placement of the REBOA catheter requires femoral arterial (open or percutaneous) access to insert a balloon into the aorta with or without a supporting wire; radiologic imaging is used to confirm proper placement. Enthusiasm for this technique has prompted a reappraisal of aortic balloon occlusion introduced nearly six decades ago during the Korean War. Based on several animal models and an increased number of recent publications, many level I trauma centers in the United States have now opted to use REBOA in patients with refractory hypotension from pelvic hemorrhage.
It appears that REBOA deployed in zone III (Fig. 15.2) may prove to be the optimal means of immediate hemorrhage control in the patient with pelvic fractures in hemorrhagic shock [12]. Transfer of patients to the interventional radiology suite for angioembolization is only appropriate when other sources of major hemorrhage have been excluded, as ongoing hemorrhage in an uncontrolled environment can be disastrous. Moreover, the arterial catheter allows for immediate hemodynamic monitoring and performance of arteriography in the operating room (OR) and eliminates the need for transport to interventional radiology.
Fig. 15.2
Aortic zones related to REBOA . Zone I extends from the origin of the left subclavian artery to the celiac artery and is a potential zone of occlusion. Zone II extends from the celiac artery to the lowest renal artery and is a no-occlusion zone. Zone III exists from the lowest renal artery to the aortic bifurcation (Reproduced from Stannard et al. [7])
Immediate percutaneous femoral arterial cannulation with a 7 French Pinnacle Precision Access System (Terumo Medical, Elkton, MD) is performed on patients in severe shock with either ultrasound guidance or manual palpation of the femoral artery. Partial responders with systolic blood pressure less than 80 mmHg are treated by placement of the REBOA catheter through the femoral artery sheath. Prepare the device by connecting the monitoring system, flushing the catheter, and removing air from the balloon. A mixture of saline and contrast should be drawn up in a 20 cc syringe for balloon inflation and opacification by digital radiograph (Fig. 15.3). The insertion length of the ER-REBOA™ Catheter is based upon the groin to umbilicus distance for zone III (just above the aortic bifurcation) occlusion. This should be measured externally with the bottom of the balloon located at the umbilicus. One should document the intended location of catheter delivery, which is essential for confirming placement at the intended location. Insert the peel away into the hemostatic valve of the sheath and advance the ER-REBOA™ Catheter under sterile conditions to the appropriate insertion length through the sheath (noted by the external length marks on the catheter shaft). Slide the peel away to the back end of the catheter. Obtain and document pre-inflation vital signs. Flush arterial monitoring port with saline, and inflate ER-REBOA™ balloon using the mixture of saline and contrast. Maximum balloon inflation is 26 mL, but typical volumes used to occlude the aorta are less than 15 mL. Following balloon inflation, vital signs, insertion length, and time of inflation for the catheter are documented. Portable radiography or fluoroscopy is used to confirm the location of the ER-REBOA™ balloon. The femoral sheath and REBOA catheter should be secured prior to patient transport (Fig. 15.3b). Based upon hemodynamic stability, the patient is quickly transferred to the CT scanner or the OR for pelvic packing and external fixation [13]. The REBOA balloon is usually quickly deflated with a goal of less than 3 h of occlusion time. Pelvic arteriography can easily be performed in the OR using portable fluoroscopy along with other necessary procedures avoiding the additional transportation to a radiology suite.
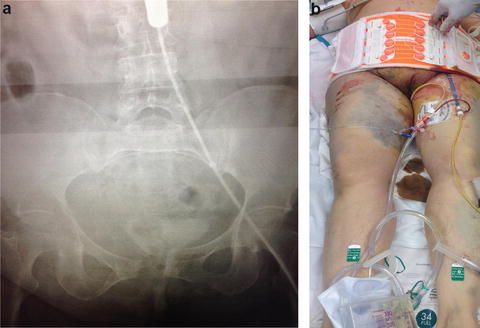
Fig. 15.3
Plain radiograph in ED demonstrating REBOA balloon inflated in REBOA zone III (a). The REBOA catheter should be externally secured to the patient prior to transport (b)
ED Triage Decision-Making
Assuming the patient has now undergone emergent endotracheal intubation, the anticipated injury pattern and response to the REBOA are important in deciding the next step. As mentioned above, many of these patients harbor additional life-threatening injuries. Thus, if the patient has a robust, sustained response to the REBOA (SBP > 120 mmHg), optimally, a rapid CT scan of the head, cervical spine, chest, abdomen, and pelvis should be considered on the way to the OR. Conversely, if the patient is hemodynamically unstable, they should be taken promptly to the OR for preperitoneal pelvic packing (PPP) , external skeletal fixation of the pelvis, and an assessment for the need for a laparotomy .
Preperitoneal Pelvic Packing
Control of pelvic hemorrhage in patients with unstable pelvic fractures can be accomplished with preperitoneal pelvic packing (PPP) . Originally described in Europe [14, 15], the technique was modified to directly pack the pelvic space through a preperitoneal approach [16]. Because 85% of pelvic fracture-related bleeding is venous or bony in origin, hemorrhage can be tamponaded within the retroperitoneal space. The combination of pelvic fracture stabilization via external fixation and tamponade of venous bleeding via PPP addresses the two major sources of bleeding. Additionally, the overall potential pelvic space can be reduced by closing down the pelvic volume with surgical stabilization and by filling the pelvic space with packing.
Related posts:
 Extremity Trauma Hemorrhage: More than Just a Tourniquet
Hemorrhage in the Critical Care Environment: Do We Have to Go Back to the OR?
Extremity Trauma Hemorrhage: More than Just a Tourniquet
Hemorrhage in the Critical Care Environment: Do We Have to Go Back to the OR?
 Hemorrhage in Prehospital and Extreme Environments: We Can’t Just Go Home
Laparoscopic Hemorrhage: Do We Have to Open?
Hemorrhage in Prehospital and Extreme Environments: We Can’t Just Go Home
Laparoscopic Hemorrhage: Do We Have to Open?
 Vascular Damage Control Techniques: What Do I Do When All Else Fails?
Vascular Damage Control Techniques: What Do I Do When All Else Fails?
 Endoscopic Hemorrhage: This is Even Harder than the Laparoscope!
Endoscopic Hemorrhage: This is Even Harder than the Laparoscope!

Full access? Get Clinical Tree


