KEY POINTS
Many patients with ventilatory failure can be successfully managed with noninvasive positive pressure ventilation (NIPPV).
NIPPV improves gas exchange, reduces the work of breathing, and relieves dyspnea.
Patients most likely to benefit include those with acute hypercapnic exacerbations of chronic obstructive pulmonary disease (COPD) or hypercapnic forms of acute cardiogenic pulmonary edema.
In selected patients with acute hypoxemic nonhypercapnic respiratory failure, NIPPV may obviate the need for endotracheal intubation. Selection may require exclusion of patients with hemodynamic instability, central neurologic dysfunction, or inability to protect the upper airway.
In severely hypoxemic patients, undiscerning use of NIPPV may inappropriately delay intubation. In these patients, the decision to switch to endotracheal intubation should be made in the first hours.
The use of NIPPV to treat postextubation respiratory distress has not been found to be superior to conventional management. Preventive use of NIV in selected group of patients may, however, be useful.
The first hour on NIPPV is important in predicting the outcome and requires experience from clinicians and to spend time at the bedside with the patient.
A favorable response to NIPPV is usually apparent within the first 2 hours. Absence of improvements in dyspnea, respiratory rate, and gas exchange in this period strongly suggests a need for endotracheal intubation.
Typical settings in a patient with COPD include pressure support of 10 to 15 cm H2O above a positive end-expiratory pressure (PEEP) of 5 cm H2O.
In appropriately selected patients, NIPPV allows a shorter hospital stay and produces better outcomes than does endotracheal mechanical ventilation.
Noninvasive positive pressure ventilation (NIPPV) has emerged as a valuable tool in the treatment of acute respiratory failure (ARF). NIPPV can substantially reduce the need for endotracheal intubation (ETI) and mechanical ventilation (MV). In selected patients, the benefits of NIPPV include decreased rates of adverse events associated with MV, shorter time spent in the intensive care unit (ICU) and hospital, and lower mortality rates. Patients with hypercapnic forms of ARF are most likely to benefit, but NIPPV may also improve outcomes of carefully selected patients with hypoxemic respiratory failure. This chapter reviews the evidence supporting NIPPV use in patients with ARF.
RATIONALE AND OBJECTIVE
When MV was first developed for widespread clinical use during the poliomyelitis epidemic, attention focused on replacing the failing respiratory muscles by a perithoracic pump. This led to the development of the “iron lung,” the first form of noninvasive ventilation, which saved many lives.1,2 Nevertheless, the device was cumbersome and impeded patient care. In addition, the iron lung proved of limited efficacy in the treatment of parenchymal lung disease. Thus delivery of mechanical assistance through an endotracheal tube that provided access to the lower airway was considered a significant advance, and positive pressure ventilation became the standard for MV.
Soon after the introduction of endotracheal MV, many complications of positive pressure ventilation were identified.3,4 These complications were found to be common and generated concern about the invasiveness of MV. ETI itself has been implicated in a large number of complications. Of these, some are directly related to the procedure, such as cardiac arrest following ETI and laryngeal or tracheal injury leading to long-term sequelae. Others are ascribable to the fact that the endotracheal tube bypasses the barrier of the upper airway: An important example is nosocomial pneumonia, which carries its own risk of morbidity and mortality. Other complications are indirectly related to ETI, such as the need for sedation, which often prolongs weaning and duration of MV. These major safety considerations prompted efforts to develop noninvasive methods for delivering positive pressure ventilation. Thus, in patients with ARF, the main goal of NIPPV is to provide ventilatory assistance while lowering the risk of adverse events by reducing the need for invasive MV. Convincing evidence that NIPPV diminishes the risk of infectious complications has been obtained not only from randomized controlled trials and meta-analysis, but also from multivariate analyses of large cohort studies and case-control studies, all of which show substantial decreases in all categories of nosocomial infection.5-7 NIPPV is indeed associated with a reduction in the overall invasiveness of patient management: Sedation is not given or at low levels, and the use of central venous lines, urinary catheters, and other invasive devices is considerably reduced, as compared to patients receiving endotracheal MV.8
Another important factor in promoting the use of NIPPV is the growing number of patients who are either unwilling to accept ETI or considered poor candidates for endotracheal MV because of their fragile underlying health status.9,10 In these patients, NIPPV can offer a chance of recovery with a low risk of complications. Last, by postponing ETI, NIPPV may provide a window of opportunity for the physician, family, and patient to make informed decisions about the goals of therapy in patients treated with palliative care.11
The use of NIPPV in the acute setting has increased markedly since the first small case-series were published in the last decade of the 20th century.12,13 Three multicenter international observational studies on the use of MV applied in the ICU have been performed in 1998, 2004, and 2010 by Esteban and colleagues in which 5.183, 4.968, and 8151 consecutive patients receiving MV over a 1 or 2 months period were evaluated, respectively.14-16 The surveys showed that the use of NIPPV progressively increased from less than 5% to around 15% of all admitted patients in the ICUs, with a constant success rate and therefore a higher number of patients avoiding the need for intubation. A greater number of patients with chronic obstructive pulmonary disease (COPD) or heart failure were also successfully treated with NIPPV out of the ICU. A limitation of these studies is that only patients who received MV in the ICU for longer than 12 hours were included. Thus, some patients treated with NIPPV for a shorter period and/or outside the ICU may have been excluded as well as patients treated outside the ICU.
Similar observational studies performed in France in 1997, 2002, and 2011,17-19 respectively, showed a major increase in NIPPV use as a first-line ventilation support for all ICU patients requiring mechanical ventilatory support (16%, 24%, and 31%; p <0.0001). Importantly, when comparing the three periods, a significant increase of NIPPV as first-line therapy (52% vs 35%; p <0.0001) was observed among those patients who were not intubated before or at ICU admission. The French survey published in 200618 indicated that Pressure Support was the most usual ventilatory mode (83%) during NIPPV (CPAP—8% and assist-control ventilation 7%). The last French observational19 study still showed a continuing increase in the overall use of NIPPV but interestingly, with a slight but significant decrease of its use in case of hypoxemic respiratory failure.
Although these results cannot be extrapolated to all ICUs worldwide, they indicate strong trends toward increasing use of NIPPV in ICU patients with a variety of conditions, and they also reflect the current approach trying to reduce the invasiveness of ICU management.
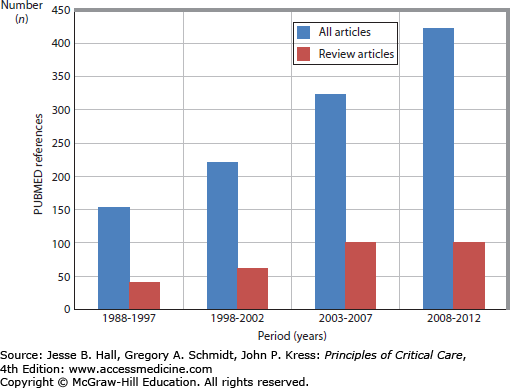
The progressive interest regarding NIPPV use can be evidenced by the number of articles concerning NIPPV published in the medical literature. Figure 44-1 illustrates the number of references concerning NIPPV and acute illness published in PUBMED over the years, using the keywords “noninvasive mechanical ventilation” or “noninvasive mechanical ventilation” or “NIPPV” and “acute respiratory failure.”
Despite the growing interest regarding NIPPV use in acute critical situations, great care should be taken to identify patients who will most benefit from NIPPV, especially those with acute-on-chronic respiratory failure and acute cardiogenic edema.20 It is also essential to identify the patients who require immediate or rapid ETI, since delaying this procedure may reduce the chances of recovery, especially, in the subgroup with acute de novo respiratory failure (free of chronic lung disease, suffering from community-acquired pneumonia, gastric content aspiration, atelectasis, and mild acute respiratory distress syndrome [ARDS]). In these patients, NIPPV failure has been shown to be independently associated with death in a observational study.20
Several types of ventilators can be used to deliver NIPPV to patients with ARF. Turbine ventilators specifically designed for NIPPV have been specifically developed to work with leaks, but standard ICU ventilators and transport ventilators can be used as well especially when they have dedicated software. Turbine ventilators designed for NIPPV deliver two levels of positive airway pressure synchronized on patient’s effort (flow or pressure trigger) or time triggered, reproducing pressure support ventilation or pressure control ventilation plus PEEP.21
Α distinguishing feature of turbine ventilators is the compensation for air leakage, which is the main cause of patient-ventilator asynchrony during NIPPV.22 Indeed, as much as 43% of patients receiving NIPPV with ventilators without NIV modes manifest patient-ventilator asynchrony, mainly attributed to leakage.23 Expiratory leaks can be falsely interpreted as patient efforts leading to autocycling. Inspiratory leaks, by hampering flow rate deceleration, prevent the ventilator from recognizing the end of patient’s effort. This can cause prolonged insufflation, triggering delay and, if excessive, ineffective efforts. Notably, the level of support during NIPPV tends to exacerbate the incidence and severity of leakage-related asynchrony.
ICU ventilators initially manufactured to function without leaks were subsequently equipped with a special adaptive algorithm, as well as some modern transport ventilators, referred to as the NIV mode, designed to mitigate the impact of leaks. Bench comparisons assessing in vitro ventilator performance suggest that both turbine ventilators specially designed for NIPPV and late-generation standard ICU ventilators equipped with NIV modes are satisfactory for delivering NIPPV to ICU patients with severe dyspnea.21,22,24-26 In a clinical study, the activation of the NIPPV algorithm in modern ICU ventilators significantly reduced the incidence of all types of asynchronies associated with leaks and this effect was more pronounced at higher levels of pressure support.27 ICU ventilators, transport ventilators, and NIPPV-dedicated turbine ventilators have been compared in terms of patient-ventilator asynchrony in the presence of leaks. Dedicated NIPPV ventilators ensured better patient-ventilator synchronization than ICU and transport ventilators, even after NIV algorithm activation. The algorithm ameliorated triggering and cycling synchronization albeit in a heterogeneous manner among ventilators.28 Turbine ventilators were, in general, much better at avoiding autocycling. No outcome data, however, like NIV success or failure, have been shown to be associated with specific asynchronies. Therefore, if an ICU ventilator is used it seems of good common sense to use the dedicated NIV algorithm.
Adequate patient monitoring may be essential to assess patient-ventilator interaction, to detect leaks, and to fine-tune pressure levels. Careful observation of the airway pressure and flow-time curves on the ventilator screen can detect patient-ventilator asynchronies which, if adequately corrected, might fasten PaCO2 normalization and accelerate patient’s adaptation.29 Whether this also ensures higher NIPPV success rates remain to be determined.
Airway gas conditioning, that is, the warming and humidification of the inspired gas, constitutes a physiological procedure performed by the human airway during normal breathing. When the upper airway is bypassed, as during invasive MV, it is indispensable to artificially heat and humidify gas prior to delivery. During NIPPV, gas is transferred to the alveoli through the mouth and nose, but the normal airway gas conditioning mechanisms can be defeated in case of high flow of the inspired air, high inspiratory airway pressure settings, high inspired oxygen fraction for turbines. All these factors contribute to the necessity of artificial heating and humidification during NIPPV. Other associated effects including structural and functional damage to the nasal mucosa, high nasal airway resistance, increased work of breathing, poor patient tolerance, and difficult intubation in case of NIPPV failure reinforce these requirements regarding gas delivery during NIPPV sessions.30,31 ICU ventilators provide much lower level of humidity compared to turbine or piston NIPPV ventilators due to the exclusive use of dry gases.30 In this case gas humidification is mandatory. Two types of humidification systems can be used to overcome the problem: heated humidifiers (HH) or heated and moisture exchanger filters (HME).
Firm recommendations cannot be made between the two systems, but the humidification ability of HME is reduced in the presence of leaks31 and their internal volume imposes an additional workload on the patient by generating CO2 rebreathing. In patients with hypercapnic respiratory failure, this can diminish the effectiveness of NIPPV in reducing blood CO2 levels and correcting respiratory acidosis.32,33 Leaks, however, may markedly reduce the importance of this problem by washing the circuit from CO2 contaminated gas. A similar problem of CO2 rebreathing occurs when turbine ventilators (using ambient room air), equipped with a one-line circuit, are used with the minimal level of PEEP allowed on these ventilators.34,35 The expiratory flow generated to create the PEEP level is indeed used to flush the exhaled CO2 from the circuit. With low PEEP levels, high minute ventilation, and/or a high respiratory rate, this can have adverse clinical effects that may require addition of a nonrebreathing valve to the circuit.
The interface used to connect the patient to the ventilator is usually a full face mask covering both the nose and the mouth. Although nasal interfaces are available, their use in ICU patients frequently results in major leakage through the mouth that diminishes the effectiveness of NIPPV and promotes patient-ventilator asynchrony and discomfort.36,37 Full face masks could be either oronasal or total face masks, both appearing similar in terms of efficacy and patient tolerance.38 Full face masks are responsible for unwanted effects including skin breakdown over the nose, conjunctivitis related to leakage of air directed toward the eyes, rebreathing, claustrophobia, and overall discomfort.13,39
These problems prompted efforts to design improved interfaces. The first improvement consisted in varying the pressure sites on the face to achieve better tolerance during prolonged use, and subsequently much larger masks enclosing the entire face or head were developed.40,41 Use of a helmet has been suggested, primarily for patients with acute hypoxemic respiratory failure.42-44 Because helmets may induce more rebreathing than other masks, they may be less suitable for patients with hypercapnic respiratory failure. The helmet probably improves patient comfort and tolerance, at the price, however, of decreased effectiveness in CO2 clearance and possibly respiratory muscles unloading.45 It was shown, however, that the helmet required higher pressures than conventional masks to reproduce the same efficacy.46 A good clinical tolerance is crucial to successful NIPPV. In their large observational survey, Carlucci and colleagues identified two independent predictors of failure: the severity score (as assessed by the Simplified Acute Physiology Score (SAPS II) and clinical tolerance.17 Interestingly, clinical physiologic studies with integral masks compared to standard full face masks seem to indicate comparable efficacy in terms of respiratory muscle unloading, suggesting that the theoretical risk of rebreathing associated with the large internal volume may be small or nonexistent in clinical practice.47,48
Numerous studies concerning NIPPV have been performed in patients with obstructive pulmonary disease, and the prevalence of COPD is high and increasing. NIPPV has demonstrated over the years important positive clinical results for treatment of acute exacerbations of COPD.13,49-53 A Cochrane database review54 showed a decrease in mortality, a reduced need for intubation, less treatment failure, faster clinical improvement, as well as reduction in treatment complications and length of hospital stay associated with NIPPV in this indication.
Pathophysiology: Exacerbation of COPD is a common cause of admission to the hospital and ICU. In addition to worsening of dyspnea and acute bronchitis symptoms, rapid and shallow breathing with hypoxemia and hypercapnia are usually present and can lead to the development of right ventricular failure and encephalopathy. The pathophysiologic pathway involves an inability of the respiratory system to maintain adequate alveolar ventilation in the presence of major abnormalities in respiratory mechanics despite a high stimulation of the respiratory centers. This can be modified by NIPPV, which allows the patient to take larger volumes with less effort, thus reversing the clinical abnormalities resulting from hypoxemia, hypercapnia, and acidosis.49,55 At baseline, the transdiaphragmatic pressure generated by these patients can be considerably higher than normal and represents a high percentage of their maximal diaphragmatic force, a situation that carries a major risk of respiratory muscle fatigue.49,56,57 The main role of NIPPV is to offer the patient a way to increase the tidal volume at a lower work level. The use of ventilatory modalities working in synchrony with the patient’s efforts allows larger breaths to be taken with less effort. As a result of the increased alveolar ventilation, arterial partial carbon dioxide pressure (PaCO2) and pH values improve, and this in turn reduces the patient’s ventilatory drive, thereby lowering the respiratory rate and improving the dyspnea.
Clinical Evidence: An international consensus conference58 published in 2001 has recommended that NIPPV should be considered as a first-line treatment in patients with acute COPD exacerbation and, more recently, different national guidelines advocated this practice.59,60 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) in 2013, reinforced the importance of NIPPV when treating COPD exacerbations with a high level of evidence (Evidence A) based on its considerable rate of success (80%–85%) in this clinical situation.61
The first evidence that NIPPV markedly reduced the need for ETI came from case-control series reported in 1990.49 Subsequently, several prospective randomized trials confirmed that NIPPV reduced the need for ETI and the rate of complications, shortened the length of stay, and improved survival in patients with COPD.50,52,53,62-65 Studies conducted in the United Kingdom established that NIPPV was also effective in non-ICU settings.50,65 In the largest ICU study reported to date, Brochard and colleagues randomized 85 patients with COPD to treatment with or without face mask pressure-support ventilation.52 The ETI rate was 74% in the controls given standard medical treatment and 26% in the NIPPV group. Benefits in the NIPPV group included a decreased rate of complications during the ICU stay, a shorter length of hospital stay and, more importantly, a significant reduction in mortality (from 29% to 9%). The overall decrease in mortality was ascribable to reductions in the need for ETI and in various ICU-related complications. In the United Kingdom, Plant and colleagues conducted a prospective multicenter randomized trial comparing standard therapy alone (control group) to NIPPV in 236 COPD patients admitted to general respiratory wards for ARF.65 Treatment failure (defined as fulfillment of criteria for ARF) was more common in the control group (27%) than in the NIPPV group (15%), and NIPPV was associated with a lower in-hospital mortality rate. Because of admission policies in the United Kingdom, patients who failed NIPPV were not routinely transferred to the ICU.
These studies made clear that early NIPPV to prevent further deterioration need to be an important component of the first-line therapy for COPD exacerbation.66
A recent database67 analyzed 7,511,267 admissions for acute exacerbations of COPD in the United States from 1998 to 2008, of which 612,650 (8.1%) required respiratory support. The authors showed an increase in the use of NIPPV (from 1.0% to 4.5% of all admissions) and a 42% decline in invasive MV (from 6.0% to 3.5% of all admissions). Intubation and in-hospital mortality have declined during this period. By 2008, NIPPV was used more frequently than invasive MV as the first-line therapy for acute exacerbations of COPD.
Whether the results of randomized controlled trials entirely apply to everyday ICU practice must be evaluated. This is particularly important with NIPPV, since there is a learning curve, as shown at least in two studies. In a single-center study by Carlucci and colleagues, the NIPPV success rate remained stable over the study period, but the patients treated with NIPPV during the last few years of the study period had more severe disease with higher PaCO2 levels and lower pH values.68 In fact, progressively, more severe exacerbations could be treated with NIPPV out of the ICU. In an 8-year study performed in a French university referral hospital, it was found that NIPPV use increased gradually, in lockstep with a decline in conventional treatment with ETI.69 In parallel with this gradual increase in NIPPV use, the nosocomial infection and mortality rates have significantly diminished.
Attention should be paid when using NIPPV in the most severely affected patients, such as those with an arterial pH <7.30 on admission,65 especially outside the ICU, if the staff is not experienced in NIPPV application and not aware of its limitations. A very low pH, marked mental status alterations at NIPPV initiation, presence of comorbidities, and a high severity score are associated with early NIPPV failure17 or late secondary failure after an initial improvement.70 Several of these factors seem to indicate that a longer time from onset of the exacerbation to NIPPV initiation may reduce the likelihood of success. Every effort should be made to deliver NIPPV early, and close monitoring is in order when NIPPV is started late, a situation where NIPPV is less effective.71
Some controversies exist concerning the use of NIPPV to treat patients with hypercapnic encephalopathy due to ARF associated with COPD exacerbation. Several observational studies showed positive clinical results72,73; however, caution might be taken when applying NIPPV in patients with altered level of consciousness.74 Close monitoring is mandatory and any delay in consciousness improvement should be interpreted as NIPPV failure and lead to prompt intubation.
The need for invasive MV after NIPPV failure in acute COPD exacerbations represents a challenging context and this subgroup of patients has a relatively high mortality rate and a greater length of hospital stay, as shown in a large observational study.67 Patients requiring invasive MV after NIPPV failure had 61% greater odds of death compared with patients directly placed on invasive MV (95% CI, 24%-109%) and 677% greater odds of death compared with a patient treated with NIPPV success without transition to invasive MV (95% CI, 475%-948%).
In conclusion, NIPPV offers many advantages over invasive MV to treat exacerbations of COPD and there is strong evidence that NIPPV is cost effective, being both more efficient and cheaper compared to standard therapy alone during the treatment of these group of patients.75,76
Long-Term Survival: A few studies have suggested that NIPPV use may be associated with higher 1-year survival rates, as compared to standard ICU therapy or invasive MV.71,77-79 Although these studies have a number of methodological flaws, the consistency of their results suggests an interesting benefit of NIPPV. Some authors argue for continuing home NIPPV after exacerbations. One of the benefits could be a reduction of the readmission rate, as suggested in one small randomized controlled trial.80,81
Other Forms of Chronic Respiratory Failure: All forms of acute-on-chronic ventilatory failure share several common pathophysiologic pathways, although major differences also exist. NIPPV may be slightly less effective in patients with chronic restrictive lung disease than in patients with COPD in the acute phase, but it remains an interesting option to propose, especially when compliance is still preserved.82
Negative Pressure Ventilation: This technique is available in very few centers in the world. In acute exacerbations of COPD, it seems to provide better outcomes than conventional invasive MV and may be similar to face mask NIPPV.83-85
Location: During the last decade, health care providers became increasingly confident in applying NIPPV, since, contrasting with invasive MV, it can be realized outside the ICU, freeing up ICU beds. The study by Plant and associates cited above was performed in respiratory wards, where the staff received 8 hours of training over the 3 months preceding the study.65
The feasibility of treating patients with COPD out of the ICU has been demonstrated, but an appropriate training of the ward staff is necessary. NIPPV usage will probably continue to increase outside the ICU in the coming years, since now NIPPV is largely available in several medical services. Hence, some hospitals have created special nursing units to assist NIPPV delivery, located commonly next to the ICU.86
Helium-Oxygen Mixture: The use of a helium-oxygen mixture for NIPPV has received much enthusiasm due to the physical properties of helium gas in reducing resistance by promoting a more laminar flow profile, with early promising results when a helium-oxygen mixture was used for COPD exacerbations.87,88 Relatively large recent clinical trials have evaluated patients with known or suspected COPD and acute dyspnea, hypercapnia, and several signs of decompensation. Unfortunately, these studies were unable to demonstrate a significant clinical benefit when a helium-oxygen mixture compared to conventional gas mixture for NIPPV was applied.89,90 One possible reason for these nonpositive results is that the rate of ETI has progressively declined in the groups treated with air-oxygen mixtures, making more difficult to evidence a difference in favor of helium.
Pathophysiology: Continuous positive airway pressure (CPAP) and NIPPV elevates intrathoracic pressure, decreases shunting, and improves arterial oxygenation and dyspnea in patients with cardiogenic pulmonary edema (CPE). Interestingly, NIPPV can both substantially lessen the work of breathing and improve cardiovascular function by decreasing the left ventricular afterload in nonpreload-dependent patients91 and also reducing the right and left ventricular preload.92 Most patients with CPE improve rapidly under medical therapy. A few, however, develop severe respiratory distress and/or refractory hypoxemia/hypercapnia and require ventilatory support until the medical treatment starts to work. This is particularly common in elderly patients, who may also have a mild degree of associated chronic bronchitis.93,94 Several NIPPV modalities have been used successfully, with the mainly goal being to avoid ETI and or hasten the improvement provided by medical therapy.
Clinical Evidence: Positive pressure applied at the mouth was already shown in the 1930s to improve patients’ dyspnea in case of CPE.95 Evidence of therapeutic efficacy of positive pressure use during acute CPE was also shown in 1985, by Räsänen et al96 randomized 40 patients with acute CPE and respiratory failure to conventional therapy or CPAP of 10 cm H2O administered by face mask. The interventional group showed a better improvement of gas exchange, a decrease of respiratory work, and a tendency for less intubation rate. Subsequently, other randomized trials comparing either CPAP or pressure support plus PEEP (PSV and PEEP) to standard therapy found similar benefits with the two techniques in terms of arterial blood gases and breathing rate improvement. Both NIPPV modes used in the emergency department or in the ICU significantly reduced the rate of ETI.94,97-99
Recently published guidelines100 recommended NIPPV use in patients with acute CPE, dyspnea, and respiratory rate >20 breaths/min to improve clinical symptoms. Nevertheless, attention should be paid in patients with low blood pressure (systolic blood pressure <85 mm Hg), vomiting, altered level of consciousness, and suspected pneumothorax. In more recent European guidelines, the level of evidence (level B-class IIa) for NIPPV use to treat acute CPE100 was lower than that formerly recommended.101
This decrease in the level of recommendations was mainly due to the publication of the 3CPO trial,102 the larger clinical multicenter, controlled study performed in the emergency department, which evaluated the possible benefits of NIPPV use in acute CPE. Patients admitted with a clinical diagnosis of acute CPE, chest radiography of pulmonary edema, respiratory rate >20 breaths/min, and pH <7.35 were randomized to conventional pharmacological therapy plus NIPPV (CPAP or PSV and PEEP) or standard oxygen therapy. The study included 1069 patients and it showed that NIPPV was associated with higher reduction in dyspnea, heart rate, and earlier resolution of metabolic abnormalities than standard oxygen therapy. Intubation rates, 7 and 30 days mortality rates (9.8% vs 9.5%, and 16.4% vs 15.2%) were similar in the control and NIPPV groups, respectively. It should be noticed that a high incidence of crossover (15%) was observed in the oxygen group, as a rescue therapy, and consequently without this cross over possibility, a much higher rate of intubation might have been observed in the oxygen group. This study has other limitations. Severely ill patients, who required “lifesaving or emergency intervention” were excluded and could have benefited from NIPPV, patients had mild hypoxemia and a very low intubation rate (3%) was observed in this study.
A more recent multicenter clinical trial103 evaluated the potential clinical benefit of CPAP use, with 7.5 to 10 cm H2O, when initiated out-of-hospital setting and continued in-hospital ICU to treat acute CPE compared to oxygen therapy at 15 L/min in the control group. Two hundred and seven patients were included over 3 years. The CPAP intervention group demonstrated significantly better and faster resolution of clinical symptoms as well as a lower presence of intubation criteria and a tendency for a lower death rate at day 7 although this last parameter was not statistically different.
CPAP or PSV and PEEP CPAP is often considered cheaper and easier to apply in clinical practice compared with PSV and PEEP. One trial104 suggested that acute myocardial infarction was more common with PSV and PEEP than CPAP but this has not been subsequently confirmed. This difference was probably ascribable to randomization bias but it invites caution in patients with coronary heart disease.99,105,106 One study compared intravenous bolus therapy of high-doses of nitrates to a more conventional medical therapy plus NIPPV.107 High-dose nitrate bolus therapy was far more effective clinically than NIPPV and resulted in better outcomes. These studies draw attention to the vulnerability of patients with CPE, particularly those with coronary heart disease and to the fact that NIPPV cannot replace adequate medical therapy.98,105
In some small studies, NIPPV was more effective regarding improvement in physiologic parameters92 or faster to improve respiratory failure108 compared to CPAP in patients with acute CPE, but no difference regarding mortality rate or tracheal intubation was demonstrated.
The 3CPO trial102 also compared both modes of NIPPV and clinical outcomes were similar in both groups, including mortality and intubation rates, myocardial infarction, mean length of hospital stay, and clinical changes at 1 hour after start of treatment. Similar results comparing both modes of NIPPV were observed in another clinical study.109
It is important to draw attention to the fact that most of the studies indicating benefits of CPAP or PSV and PEEP included patients who, on average, had marked hypercapnia and acidosis indicating acute frank ventilatory failure.94,98,99
Related posts:






Full access? Get Clinical Tree


