![]() Used as emergent vascular access for fluid resuscitation and drug infusion when unable to obtain peripheral venous access
Used as emergent vascular access for fluid resuscitation and drug infusion when unable to obtain peripheral venous access
![]() Primarily used in pediatric cardiac arrest—generally a faster access than central line in infants or children
Primarily used in pediatric cardiac arrest—generally a faster access than central line in infants or children
![]() Used in adult resuscitation if other forms of vascular access cannot be established
Used in adult resuscitation if other forms of vascular access cannot be established
CONTRAINDICATIONS
![]() Absolute Contraindications
Absolute Contraindications
![]() Fracture at the insertion site
Fracture at the insertion site
![]() Relative Contraindications
Relative Contraindications
![]() Previous attempt to place intraosseous (IO) needle on the same bone
Previous attempt to place intraosseous (IO) needle on the same bone
![]() Osteogenesis imperfecta
Osteogenesis imperfecta
![]() Osteoporosis
Osteoporosis
![]() Overlying infection, burn, or skin damage at insertion site
Overlying infection, burn, or skin damage at insertion site
RISKS/CONSENT ISSUES
![]() Pain (local anesthesia can be given)
Pain (local anesthesia can be given)
![]() Local bleeding and hematoma
Local bleeding and hematoma
![]() Growth plate injuries or fractures
Growth plate injuries or fractures
![]() Extravasation of fluid or drugs through iatrogenic fracture/puncture site
Extravasation of fluid or drugs through iatrogenic fracture/puncture site
![]() Osteomyelitis and cellulitis
Osteomyelitis and cellulitis
![]() General Basic Steps
General Basic Steps
![]() Sterilize
Sterilize
![]() Anesthesia
Anesthesia
![]() Place IO
Place IO
LANDMARKS
![]() Standard placement of the IO line is 1 to 2 cm distal to the tibial tuberosity on the anteromedial aspect of the tibia (FIGURE 25.1)
Standard placement of the IO line is 1 to 2 cm distal to the tibial tuberosity on the anteromedial aspect of the tibia (FIGURE 25.1)
![]() Alternate sites for placement
Alternate sites for placement
![]() Medial aspect of the distal tibia approximately 1 to 2 cm proximal to the medial malleolus (FIGURE 25.2)
Medial aspect of the distal tibia approximately 1 to 2 cm proximal to the medial malleolus (FIGURE 25.2)
![]() Anterior aspect of the distal femur just proximal to the junction of the femoral shaft and the lateral and medial condyles
Anterior aspect of the distal femur just proximal to the junction of the femoral shaft and the lateral and medial condyles
TECHNIQUE
![]() Sterilize the insertion site with povidone–iodine solution, chlorhexidine, or alcohol
Sterilize the insertion site with povidone–iodine solution, chlorhexidine, or alcohol
![]() If the patient is awake, administer a local anesthetic to the skin and periosteum
If the patient is awake, administer a local anesthetic to the skin and periosteum
![]() For manual IO insertion:
For manual IO insertion:
![]() Grasp the IO needle in the palm of the hand using the index finger and thumb to guide and stabilize the needle
Grasp the IO needle in the palm of the hand using the index finger and thumb to guide and stabilize the needle
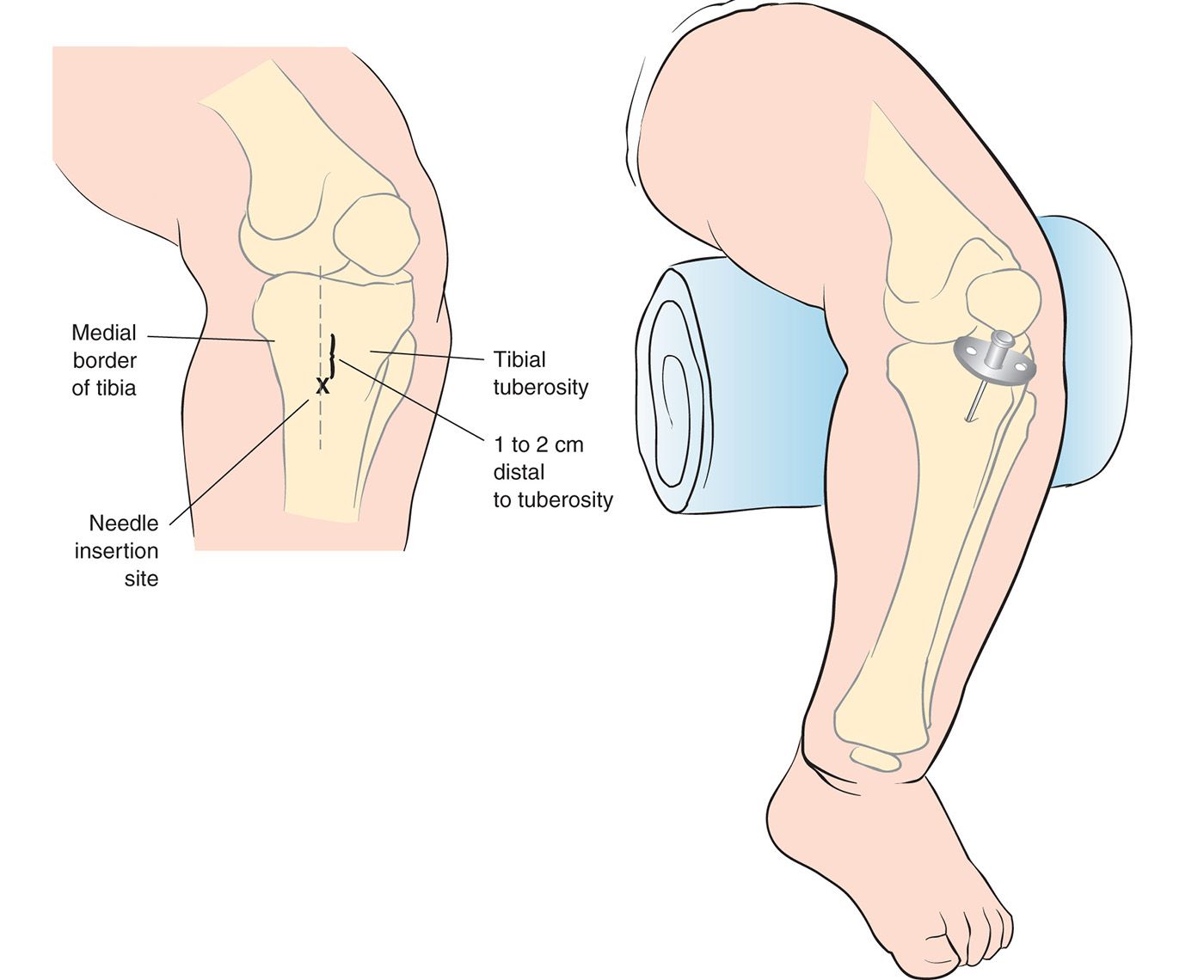
FIGURE 25.1 Entry site at the proximal tibia. (From Hodge D III. Intraosseous infusion. In: King C, Henretig F, eds. Textbook of Pediatric Emergency Procedures. Baltimore, MD: Williams & Wilkins; 2008.)

Full access? Get Clinical Tree


