CHAPTER 15 Interscalene block
Clinical anatomy
The cervical nerves exit from the cervical spine through gutters in the transverse processes that run in an anterolateral direction, immediately posterior to the vertebral artery. The cervical nerves enter a facial space in the posterior triangle of the neck between the anterior and middle scalene muscles called the interscalene compartment (Fig. 15.1). The interscalene block is performed at the level of the cricoid cartilage (C6). Important anatomic relations (Fig. 15.2) include the external jugular vein, which crosses the posterior border of the sternocleidomastoid muscle at this point, the phrenic nerve on the anterior scalene muscle, and the vertebral artery.


Surface anatomy
The main landmarks for the interscalene block (Fig. 15.3) include clavicle; sternal notch; cricoid cartilage; sternal and clavicular heads of the sternocleidomastoid muscle – these can be accentuated by asking the patient to perform a head lift; interscalene groove – both scalene muscles descend to the first rib and can be identified by asking the patient to inhale deeply, because they contract before the sternocleidomastoid muscle; and the external jugular vein –which can be accentuated by asking the patient to perform a Valsalva maneuver. A skin marker should routinely be used to delineate the anatomic structures before performing the block.

Sonoanatomy
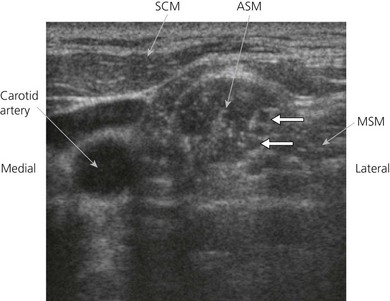
Perform a systematic anatomical survey from medial to lateral and superficial to deep. The carotid artery and internal jugular vein are seen medially. Medial to the vessels, the thyroid and trachea are identified. The ultrasound-guided intrascalene block is performed at the lateral border of the clavicular head of the sternocleidomastoid at the level of the cricoid cartilage. Here the brachial plexus is a superficial structure and a high frequency ultrasound transducer (6 to 13 MHz) is used. A high frequency transducer allows good visualization of structures to a depth of 4–5 cm. The ultrasound transducer is placed in an axial oblique plain (Fig. 15.4) and the most superficial structure consistently encountered is the sternocleidomastoid muscle. This appears as a triangular structure with the apex pointing laterally. Immediately deep to the sternocleidomastoid muscle are the anterior and middle scalene muscles. These can be accentuated by asking the patient to sniff. The roots of the brachial plexus appear between these two muscles in the interscalene groove. At this level it is common to identify between one and five hypoechoic structures (roots or trunks) and, depending on the position of the ultrasound transducer, these may appear oval or round. The brachial plexus at this level lies at a depth of around 1 cm from the skin (Fig. 15.5).

Technique
Landmark-based approach
The patient is placed in the supine position with the head facing away from the side to be blocked. The patient is asked to elevate the head slightly to bring the clavicular head of the sternocleidomastoid muscle into prominence. The palpating finger is placed behind the sternocleidomastoid muscle and the patient is instructed to end the head lift (Fig. 15.6). The finger now lies on the belly of the anterior scalene muscle, and with lateral movement of the finger to the lateral edge of this muscle, the groove between the anterior and middle scalene muscles (interscalene groove) is encountered (Fig. 15.7). The injection site in the interscalene groove lies at the level of the cricoid opposite the transverse process of C6 (Chassaignac tubercle).

Figure 15.6 Locating the interscalene groove. The palpating fingers are placed deep to the sternocleidomastoid muscle.







Full access? Get Clinical Tree


