CHAPTER 33 Intercostal block
Clinical anatomy
The intercostal nerves contribute and receive sympathetic fibers. Shortly after exit from the intervertebral foramina, the dorsal rami become a posterior cutaneous branch to skin and muscles in the paravertebral region (Fig. 33.1). At the angle of the ribs, a lateral cutaneous and a collateral branch arise. The collateral branch follows the lower border of the space in the same intermuscular interval as the main trunk, which it may or may not rejoin before it is distributed as an additional anterior cutaneous branch. The lateral branch accompanies the main trunk for a time before piercing the intercostal muscles obliquely. The main trunk continues anteriorly as the anterior cutaneous branch.
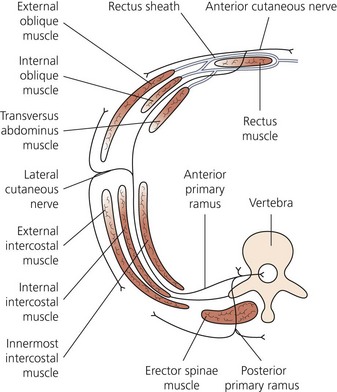
The interior lower edge of the ribs provides a channel for the intercostal nerve and its companion artery and vein. The nerve lies just behind the lower border of the rib. Near the midaxillary line, the groove becomes less well defined, and the nerve migrates away from the rib (Fig. 33.2). The structures between skin and intercostal nerve vary, depending on body wall location on the nerve’s path. At the back of the chest, the nerve lies between the pleura and the posterior intercostal membrane (extension of internal intercostal muscle), but in most of its course it runs between the internal intercostal muscles and the intercostalis intimi. Where the latter muscles are absent, the nerve lies in contact with the parietal pleura. In the intercostal groove, the vein lies superior, with the artery and nerve more inferiorly. This relation is not consistent, particularly in the paravertebral region.

Surface anatomy
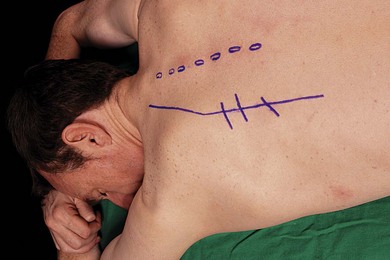
Important bony structures relevant to the intercostal nerve block include the thoracic spinous processes, paraspinal muscles, posterior angulation of ribs, spine, and inferior tip of scapula. The lateral edge of the paraspinal muscles is identified and marked. This is at the posterior angle of the ribs. These lines angle medially in the upper thoracic region so as to parallel the medial edge of the scapula. The midline spinous processes are also marked. The inferior edges of the ribs are palpated and marked. At the intersection of lines are the needle insertion points (Fig. 33.3).
Sonoanatomy
The chest wall is best imaged in a coronal (vertical) plane. Using a 6–13 MHz linear transducer, the relevant intercostal space is visualized. The ribs appear as dense dark oval structures with a bright surface (periosteum; Fig. 33.4). A dark shadow is cast deep to the rib on ultrasound, illustrating the phenomenon of echo shadowing. Echo shadowing is an echo-free zone immediately behind a structure of high absorbance or reflectivity, such as bone, calculi or metal prosthesis. The pleura and lungs are visualized deep to the intercostal space between the echo shadows (Fig. 33.4).
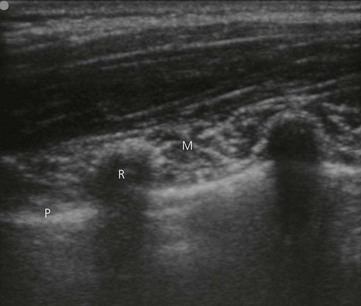
Figure 33.4 Ultrasound appearance of the intercostal space. R: rib; M: intercostal muscle; P: pleura.







Full access? Get Clinical Tree


