CHAPTER 9. Safety and Survival
Gordon H. Worley
Competencies



Get Clinical Tree app for offline access
1. Identify the safety risks related to air and surface patient transport and methods to reduce those risks.
2. Describe the medical transport industry’s safety initiatives to improve safety and reduce accident rates.
3. Describe safe operations around helicopters, fixed-wing aircraft, and ground transport vehicles.
4. Understand and use Air Medical Resource Management.
5. Correctly perform emergency procedures, including emergency egress.
6. Identify the components of a Postaccident Incident Plan.
7. Identify the priorities in a survival situation and perform basic survival skills, including shelter building, fire building, water procurement, and signaling.
“Safety does not just happen, it is not a specific event or a ‘thing’ — it is an attitude.”
Dr. Ira Blumen and the UCAN Safety Committee, 20026
Most chapters in this book contain information intended to help the air medical or ground transport crew member provide care for the critically ill or injured patient. This chapter is different; its purpose is to encourage the development of a safety attitude. It seeks to foster an active awareness and commitment to safety in every aspect of every mission. In short, it is devoted to taking care of the transport team member.
A safety culture must exist within every transport program. Each member of the program must accept that they contribute directly to a safe environment. Every individual, whether they are a nurse, paramedic, physician, respiratory therapist, emergency medical technician (EMT), pilot, mechanic, communications specialist, or administrator, must accept personal responsibility for safety and be a safety advocate.
DEFINITION OF SAFETY
Webster’s Dictionary defines safety as “… the state of being safe from the risk of experiencing or causing injury, danger or loss.” Few human endeavors are completely safe from risk. The medical transport environment by its nature presents a wide range of potential risks. Medical transport exists at the unique interface of aviation, public safety, emergency medicine, and critical care medicine, all of which are complex technologic and human systems. In any complex system, human errors inevitably occur. 3 Effective risk management and safety programs recognize this and focus efforts on both reducing the rate of errors and, more importantly, reducing the consequences of the errors that do occur.
Safety may best be defined in the medical transport setting as: identifying risks and managing them in such a way as to eliminate or significantly reduce the possibility of accident or injury. The following sections explore some of the significant risks associated with air and ground medical transport and identify what has been, and is being, done to manage these risks and improve safety in the transport environment.
HAZARDS IN THE TRANSPORT ENVIRONMENT
Note: The use of the term accident in the following discussion reflects its use by the National Transportation Safety Board (NTSB) for an event “… in which any person suffers death or serious injury, or in which the aircraft receives substantial damage.”10 This does not suggest that these tragic events are or were unavoidable. Most, if not all, of the accidents discussed had controllable factors that could have potentially prevented the occurrence or lessened the severity of the event.
Air Medical Accidents
The first hospital air medical program was established in 1972. In the following years, the air medical industry underwent tremendous growth, from that one program in 1972, to 32 in 1980, and 101 by 1985. 6 With this growth came the realization that air medical helicopters had an accident rate far greater than that of helicopters engaged in general aviation.
From 1980 to 1985, the helicopter emergency medical services (HEMS) industry had an estimated accident rate of 12.3 accidents/100,000 patients transported. The accident rate for nonscheduled turbine-powered air taxi helicopter operators, a comparable non-HEMS population, was 6.9/100,000 for the same time period. 47 In 1988, the NTSB released the results of its investigation of 59 Emergency Medical Services (EMS) accidents that occurred between 1978 and 1986. The study concluded that weather-related accidents were the most common and most serious type of accident experienced by EMS helicopters. 47
The 1990s showed continued growth in the air medical industry, from an estimated 174 HEMS programs operating 232 helicopters in 1990 to 225 programs operating 360 helicopters in 1999. 6 In 1990, one accident occurred with no fatalities. During the next 5 years, an average of 5.5 accidents per year occurred. In 1996, only one HEMS accident again was seen, this one fatal, and three were seen in 1997. During the period from 1998 to 2001, the accident rate increased sharply to an average of 10.8 HEMS accidents per year. 6 A review of 121 air medical accidents from the late 1970s through the late 1990s found weather-related accidents to be the most common type, with an increase of 10% from the 1980s to the 1990s. 22.23. and 24.
In 2002, the Air Medical Physicians Association (AMPA) released A Safety Review and Risk Assessment in Air Medical Transport, which examined HEMS accidents from 1980 to 2001. 6 This report looked not only at the total yearly numbers of accidents but also at accident, injury, and fatality rates as functions of the number of EMS aircraft operating, the number of patients transported, and the estimated total flight hours for each year. The analysis showed a generally decreasing trend in number of HEMS accidents per 100,000 patient transports from the high in 1982 of 24.9/100,000 (a higher rate than that calculated by the NTSB in 1988) to a low in 1996 of 0.57/100,000. The average for the last 5 years of the study (1997 to 2001) was 4.6/100,000 patient transports. The most common recurrent factors in HEMS accidents were again found to be poor weather conditions and operations at night.
In 2003, the year after the publication of the AMPA study, there were 18 HEMS accidents, four of which were fatal. The year 2004 had 13 accidents, and 2005 had 17, with six fatal accidents each year. In January 2006, the NTSB released an Aviation Special Investigation Report that examined 55 EMS aircraft accidents that occurred between January 2002 and January 2005, 41 of which were helicopter accidents. 48 The investigation identified these recurrent safety issues:
▪ Less stringent requirements for EMS operations conducted without patients on board.
▪ A lack of aviation flight risk evaluation programs for EMS operations.
▪ A lack of consistent comprehensive flight dispatch procedures for EMS operations.
▪ No requirements to use technologies such as terrain awareness and warning systems (TAWS) and night vision imaging systems (NVIS) to enhance EMS flight safety.
Also in 2006, Baker et al5 reviewed HEMS accidents for the period from 1983 to 2005 to determine the factors related to fatal outcomes. They concluded that accidents that occur at night or in bad weather or that result in a postimpact fire have a higher risk of being fatal. 5
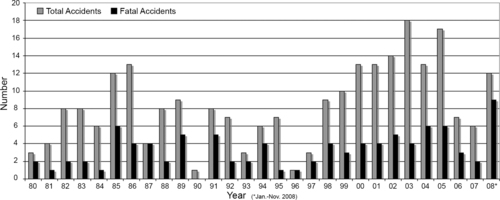
In 2006, a total of seven HEMS accidents occurred, three with fatalities, and in 2007, six accidents occurred, two of which were fatal. The year 2008 brought the worst year in the industry’s history for fatal accidents, with a total of 12 HEMS accidents from January to November 2008, including the first-ever mid-air collision of two helicopter air ambulances (included in these totals as two accidents). Nine of these accidents were fatal, claiming a total of 29 lives, including five patients. 11,26,46 In 2008, 264 HEMS programs were in the United States, operating 699 helicopter bases and a total of 840 helicopters, 4 more than twice the number of aircraft in operation in 1999. Figure 9-1 summarizes accidents from January 1980 to November 2008.
Fixed-wing air medical accidents have not been as well studied as HEMS accidents. In 2008, 108 air medical programs listed in the Atlas and Database of Air Medical Services (ADAMS) operated a total of 292 fixed-wing aircraft. 4 Sixty-two of these programs operated both fixed-wing aircraft and helicopters. A review of accident data from 2002 to November 2008 showed a total of 14 accidents from 2002 to 2006, six of which were fatal. In 2007, six fixed-wing air medical accidents occurred, four of which were fatal; none were found in 2008. 11,26,45,48
The data presented do not pretend to paint the whole picture of accident risk in air medical transport. The actual rates and the causes of air medical accidents are continuing topics of intense study and debate. 3 Although specific numbers and root causes may not always be clear, what is clear is that we continue to have accidents and that patients and flight crews continue to be injured and killed. Also clear is that recurrent factors continue to be involved in air medical accidents, most notably operations at night and in inclement weather. We need to maintain a respect for these hazards and promote (and use) every tool and practice available to reduce the risks of flight in the HEMS environment.
Ground Ambulance Accidents
The same level of attention paid to air medical accidents has not been paid to ground ambulance accidents. Unlike air medical accidents, which must be reported and are investigated by the NTSB, ground ambulance crashes are generally monitored on a state or local level, which makes consistent nationwide data difficult to obtain. In 2001, Kahn et al30 published a review of all reported fatal US ambulance crashes from 1987 to 1997. The 339 fatal accidents resulted in 405 fatalities and 838 injuries. Those victims in the rear compartment who were unrestrained or improperly restrained had the most severe injuries and fatalities. Most of the crashes (202/339), and fatalities (233/405), occurred during emergency operations. The most common crash location was at an intersection. 30 The Centers for Disease Control (CDC) reported in 2003 on 300 fatal ambulance crashes that occurred from 1991 to 2003. These crashes resulted in the deaths of 27 on-duty EMS workers, 55 other occupants of the ambulances, and 275 occupants of other vehicles and pedestrians. Most of the EMS worker fatalities (60%) occurred in the front of the vehicle. 39
These studies show that ground ambulance accidents also have recurrent contributing factors. Safety training programs should focus on awareness of these risks, safe driving, and proper use of safety equipment, such as seatbelts. Ground transport programs need to establish the same safety culture and have the same commitment to safety and risk reduction as air medical programs.
Reducing the Risks
Since the 1980s, efforts have been made to reduce the risks of flight in the air medical environment. These efforts at risk reduction have taken many forms, from safety policies and procedures, to training and new technologies.
Critical Thinking, Decision Making, and the Human Factor
The probable cause for many of the accidents described previously is listed as pilot error, which is another way of saying the pilot made a bad decision, or a series of bad decisions, that resulted in the accident. Decision making in the aviation environment is a complicated process, with many factors that need to be considered. To be able to make good decisions, pilots and flight crew members need to have training in critical thinking and decision making in the HEMS environment and have access to decision-making tools. 29 These tools may be technologies, policies, algorithms, or other processes. No single tool or practice ensures a good decision, but used together they can be effective in helping pilots and crews make safe decisions. The human factor, the ability of the pilot and crew to make informed safe decisions, remains the single most important factor in ensuring safety in the medical transport environment.
Weather Minimums
From the beginnings of the industry, weather and impaired visibility (instrument meteorologic conditions [IMC]) have been recognized as a significant cause of accidents. The Commission on Accreditation of Medical Transport Systems (CAMTS) accreditation standards require that programs have minimum cloud ceiling and visibility limits for operations under visual flight rules (VFR). 12 In November 2008, the Federal Aviation Administration (FAA) released draft revisions to Operations Specification that pertained to HEMS operations. The revisions include higher VFR ceiling, visibility and obstacle clearance requirements when a “flight or sequence of flights includes a part 135 segment.”19 These new Operations Specifications became effective in February 2009. Each program’s weather minimums must comply with FAA regulations, meet CAMTS requirements, and address the specific needs and hazards of the program’s operating area. Once a program’s weather minimums have been established, they need to be followed; “pushing the envelope” on minimums has been implicated in many weather-related HEMS accidents.
Another weather-related concern noted in the 2006 NTSB report was the lack of reliable information regarding weather conditions in many areas where HEMS programs operate, which increases the risk of an inadvertent entry into IMC. In an effort to find ways to reduce this risk, representatives of the HEMS industry, the FAA, and the University Center for Atmospheric Research (UCAR) conducted a HEMS Weather Summit in 2006. One result of this summit was the development of the Aviation Digital Data Service (ADDS) experimental HEMS Low Altitude Flight Tool (http://www.weather.aero/hems/). This online application is designed to enhance the safety of flight in the low altitude environment used by HEMS aircraft. It provides a visual representation of ceiling, visibility, convection, radar information, and geographic information system (GIS) data in areas between established weather reporting sites. 20,43
Mission Planning and Risk Assessment
The safe completion of any medical transport mission starts with mission planning. The first step in mission planning is an assessment of the potential risks involved, which leads to a decision about whether or not the mission should be accepted. Once the decision has been made to accept the mission, other aspects of mission planning must occur, including weight and performance planning, fuel management, destination considerations, pilot and crew duty time, and clinical factors.
Operational risk assessment begins with a daily or shift evaluation, which takes into account factors that remain relatively constant during the day. These factors can include prevailing weather patterns, pilot and crew experience, and the availability of safety technologies (discussed subsequently). Another risk assessment should be performed at the time of each mission request, evaluating the time of day, current weather conditions, weather forecasts, pilot and crew fatigue, and other variables. Some programs have established operational control centers to assist pilots in assessing the risks of certain missions by having the mission request reviewed and any identified risks evaluated by another individual (typically a senior pilot) before the request is accepted. Figure 9-2 shows an example of a computer-based risk assessment tool.
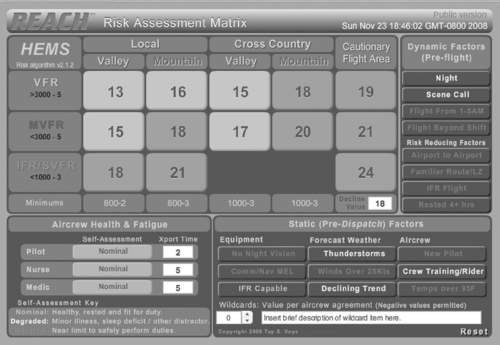 |
| FIGURE 9-2 A computer-based risk assessment tool. This computer program takes into account weather conditions, operating area, pilot and crew experience, pilot and crew fatigue, safety technologies (IFR, NVG, etc), and other factors to provide an objective measure of the risk presented by any individual transport request. (Image courtesy of Tay S. Voye, 2008, available at http://www.hemsrisk.com.) |
Risk assessment should be a fluid dynamic process. If conditions change as the mission progresses, then so should the risk assessment. Pilots and flight crews need to continuously observe and evaluate the mission environment and the potential risks. If changes in the mission environment can be anticipated, then decision thresholds and alternative plans can be discussed and decided on ahead of time.
Declined Missions
Although the pilot-in-command (PIC) has the ultimate responsibility for accepting or declining any mission request, all members of the flight team have the right, and the responsibility, to refuse to accept any mission where there is a legitimate safety concern. Each program should have a written policy for declining or aborting missions, so that individual crew members do not have to worry about disciplinary action or other negative action as a result of refusing to participate in a mission because of safety concerns. 1 The safety culture of the program should support the “Three to say go, one to say no” philosophy.
Air Medical Resource Management
Air Medical Resource Management (AMRM) is the operational practice of involving all members of the flight team (pilot and clinical crew members) in mission planning, decision making, and mission safety. It is the air medical industry’s adaptation of Crew Resource Management (CRM), used in the commercial aviation industry and by the US Air Force. CRM grew out of several significant accidents that resulted from poor decision making on the part of airline pilots, in some cases over the objections of other flight crew members. 52 The PIC was traditionally the sole decision maker in an airline cockpit. The rest of the crew followed the PIC’s instructions and did not offer input or question decisions. By encouraging crew members to pay attention, make suggestions, and voice concerns, CRM involves all of the crew members in the decision-making process. The PIC still has the ultimate authority and responsibility for the aircraft, but other crew members are able to offer suggestions or, more importantly, question decisions they feel are unsafe or unwise. 52
The essence of AMRM/CRM is teamwork, based on good communication between all crew members and the use of all available resources to maximize mission safety. 6 Mutual respect, trust, and an organizational culture that supports safety provide the best environment for effective communication and use of AMRM. AMRM classes should be a part of initial and recurrent training and should involve both pilots and clinical crew members in a group setting.
Helicopter Shopping
Fatal HEMS accidents have occurred when a HEMS program has accepted a mission that had been declined by another provider. 46 The International Association of Flight Paramedics (IAFP, formerly the National Flight Paramedics Association [NFPA]) published a position paper in 2006 that addressed the problem of local agencies placing sequential requests to different air medical programs in an attempt to obtain a response to a mission request that had been declined by one provider (or multiple providers) for reasons of weather, landing zone availability, or other safety factors. This practice in commonly referred to a helicopter shopping. 28
All programs need to educate the EMS agencies, dispatch centers, and hospitals in their service areas about the hazards of this practice and work with them to develop systems to prevent it. When any program declines a mission request, the reason should be clearly stated and communicated to any other program that may be asked to accept the mission. Air medical programs that serve the same areas should have interprogram communication pathways to permit each program to notify others when a mission is declined or to inquire whether another program has turned down a request. These pathways may include regional or national turndown reporting web sites or formal interprogram notification systems. If the nature of a flight request (location, etc) suggests that another program may have been contacted first, the dispatcher/communications specialist should inquire whether any other programs were contacted about the flight and the reasons for any declines.
Safety Technologies
All reviews of air medical accidents have identified the same two environments as significant contributing factors: operations at night and during bad weather. These two environments have one major factor in common: reduced visibility. A variety of technologies can reduce the risk of operating during reduced visibility conditions by supplying additional information about potential hazards in the flight environment. One of the recurrent safety issues identified in the 2006 NTSB report was the lack of requirements that air medical aircraft make use of these safety technologies to enhance flight safety.
Instrument Flight
Flight operations under instrument flight rules (IFR) are a common practice for fixed-wing aircraft but are less common in helicopter aviation. Many helicopter models used in air medical transport are not approved for instrument flight, except in emergency conditions. When operating under IFR, the pilot is flying under the guidance of the FAA air traffic control (ATC) system. The controller monitors the position of the aircraft on radar and provides routing instructions that keep the aircraft away from terrain and other air traffic. 51 For an IFR-capable aircraft and pilot, unexpected entry into IMC is an inconvenience, not an emergency. Many newer models of helicopters are designed and equipped to be IFR capable.
Night Vision Goggles
Night vision goggles (NVGs, also called night vision imaging systems [NVIS]) use an electronic system to amplify visible light and provide improved visibility during night operations. NVGs have been in use by the military for many years and have seen a rapid acceptance in the HEMS community in recent years. In 2008, the National EMS Pilots Association (NEMSPA) released a survey of 382 active HEMS pilots on the subject of NVG usage in the HEMS environment. The responses were overwhelmingly in favor of the use of NVGs in night HEMS operations. 41 NVGs are expensive and may necessitate that the aircraft be modified to be compatible with the system’s lighting requirements.
Terrain Awareness and Warning Systems
One of the common scenarios in air ambulance accidents is loss of adequate visibility and subsequent controlled flight into terrain (CFIT). Terrain awareness and warning systems (TAWS) provide the pilot with a visual display of the terrain along the flight path and alert the pilot with visual and audible alarms if the aircraft flies too close to the terrain. Some of these systems also include a traffic collision avoidance system (TCAS), which provides information about the location of other nearby air traffic.
Satellite Tracking and Position Reporting
Automated flight following with a satellite-based tracking system provides the flight communications center with up-to-the-minute information regarding the position and status of the aircraft. In the event of an emergency situation, the exact position of the aircraft is always known. Many of these systems also permit satellite-based voice and data communications.
Crashworthy Aircraft and Vehicle Systems
Design changes to improve the crashworthiness of the airframe, fuel system, and seats in US military aircraft have shown improved crash survival rates. 32 Newer civilian and military helicopters are equipped with crashworthy landing gear, crashworthy fuel systems, and crash attenuating seats that absorb energy and reduce the g force applied to the occupant in a hard impact to improve occupant survival in a crash. 5 Changes in ground ambulance design to enhance safety have included improved seat and seatbelt/harness restraint systems for occupants of the rear compartment, ergonomic interior designs that permit easier access to the patient and supplies while remaining restrained, padded ambulance interiors, and back-up camera systems.
INDUSTRY SAFETY INITIATIVES
When the disturbing HEMS accident rates of the 1980s were identified, the air medical industry recognized the need to improve safety and reduce accident rates. A great emphasis has been, and continues to be, placed on improving air medical safety and risk management techniques. A number of organizations have launched programs and established standards designed to improve safety practices, enhance the safety consciousness of the industry, and reduce or eliminate errors of consequence. 3
Air and Surface Transport Nurses Association
The Air and Surface Transport Nurses Association (ASTNA, formerly the National Flight Nurses Association [NFNA]) has long been a safety advocate and has published a series of position papers related to air medical safety. ASTNA is a professional nursing organization with a membership that includes transport nurses from throughout the United States and Canada. In 1988, the NFNA (ASTNA) published the position paper Improving Flight Nurse Safety in the Air Medical Helicopter Environment. In this paper, the organization endorsed many of the recommendations of the NTSB study published earlier the same year. The NFNA stated that “available knowledge and technology which could significantly enhance [a] flight nurse’s safety in the air medical helicopter environment is not consistently applied and utilized in all air medical transport programs.”42 The position paper proposed several corrective measures. The proposals dealt with: (1) crew scheduling and rest periods; (2) the right of flight nurses to refuse to participate in a flight as a result of concerns for personal safety; (3) the need for programs to develop written protocols for the use of physical and pharmacologic restraints when combative or potentially combative patients are transported; (4) the need for programs to critically evaluate hot-loading and unloading policies and procedures and to ensure personnel assigned to hot load or unload do so only after proper training; and (5) the adoption of measures to maximize safety and reduce the potential of serious injury with use of helicopter design changes such as energy-attenuating seats, addition of shoulder harnesses to lap belts at each position in the aircraft, and development and installation of crash-resistant fuel systems in aircraft as soon as possible.
The 1988 NFNA position statement also dealt with specific in-flight duties to be performed by flight nurses to ensure a safe aviation environment. These responsibilities included: (1) securing equipment during flight; (2) use of seat belts and shoulder harnesses; (3) properly securing patients within the aircraft; (4) judicious use of night lighting; and (5) isolation of the pilot and controls from potential patient movement.
In 1998, the NFNA position paper was updated and expanded to include the following recommendations: (1) that flight nurses interact more with the PIC, participating in recurrent safety, premission, and postmission briefings; being taught how to report aircraft position; and undergoing crew member emergency training; (2) use of appropriate personal protective gear, including helmets, flame-resistant flight uniforms, and protective footwear; (3) stress-management programs to enhance flight nursing performance; and (4) use of back-up aircraft that are similar to the primary aircraft in the flight program. 42 These recommendations have since become part of routine operations for a large portion of the air medical industry.
In 2006, a third revision, Transport Nurse Safety in the Transport Environment, was published. It reinforced the positions stated in the first two editions of the paper and updated them to reflect the safety concerns of the medical transport industry in the early 21st century. The paper also expanded its focus to apply to transport nurses in all practice settings, including helicopter, fixed-wing, and ground patient transport. 1
The Commission for Accreditation of Medical Transport Systems
In 1990, the Commission for Accreditation of Medical Transport Systems (CAMTS) was established. The CAMTS accreditation standards require that “There is evidence that safety issues are addressed specific to the operational environment (i.e., weather, terrain, aircraft performance).” CAMTS standards also contain recommendations and requirements for weather minimums, safety management programs, accident/incident reporting, and pilot and flight crew training. 12
The Air Medical Safety Advisory Council
The Air Medical Safety Advisory Council (AMSAC) was organized by the Association of Air Medical Services (AAMS) in 2002 at the request of the FAA to address the increasing rate of air medical accidents. AMSAC is composed of representatives from AAMS, NEMSPA, ASTNA, FAA, National Aeronautics and Space Administration (NASA), insurance companies, and other industry groups. It serves as a forum to discuss the safety issues and concerns of the air medical community, including flight and duty time, fatigue countermeasures, minimum flight time standards, AMRM, data collection, accident/incident reporting, and shared critical maintenance information. A focus area for AMSAC has been the potentially negative effect of interprogram competition. 35
Vision Zero
In 2005, AAMS, in cooperation with many other organizations, launched the Vision Zero Initiative “to reduce and eliminate errors of consequence—those events within the transport medicine environment that result in serious injury or fatality”3 by 80% in 10 years. The Vision Zero Initiative is intended to foster communication and cooperation between all aspects of the medical transport industry (safety organizations, professional associations, trade organizations, and regulatory agencies) to develop voluntary and regulatory measures to achieve the stated goals. 3
Voluntary Safety Reporting
Voluntary safety reporting systems encourage individuals, transport programs, and aviation certificate holders to voluntarily report safety issues, concerns, and events. By submitting voluntary reports, programs and individuals may identify safety issues that affect more than just their program or agency and permit others to learn from their experience. The CONCERN Network (http://concern-network.org) is a voluntary reporting system whose purpose is “to increase awareness of safety hazards in the medical transport community.” Transport programs submit reports of accidents or incidents, and bulletins are then distributed via e-mail to CONCERN Network subscribers and maintained in an online archive. 11 Transport team members may also submit anonymous reports. The FAA’s Aviation Safety Action Program (ASAP) is designed to improve safety throughout the aviation industry. It allows participants to submit confidential reports that “identify actual or potential risks throughout their operations.” All of the parties involved can then work together to develop or update operational practices to reduce the risk of accidents and other safety-related events. 18
SAFETY MANAGEMENT
An effective comprehensive Safety Management System (SMS) should be a major part of all transport programs. The commitment to safety must include “… all disciplines and processes of the organization.”12 Safety needs to be a core component of the organizational culture of every transport program, from the CEO to the newest front-line employee.
The Accreditation Standards published by CAMTS list the components of a Safety Management System, which include12:
▪ Involvement of senior management.
▪ A safety committee.
▪ A nonpunitive system for employees to report hazards and safety concerns.
▪ A system to track, trend, and mitigate errors or hazards.
▪ A safety manual.
▪ Operational risk assessment tools.
▪ Ongoing safety training for all personnel (including managers).
▪ A system to audit and review organizational policy and procedures.
▪ A mechanism to ensure compliance with safety policies and procedures.
The Safety Committee
The Safety Committee should be composed of representatives of all disciplines involved in the transport program: aviation, clinical, maintenance, communications, and administration. The committee should meet at least quarterly to address safety issues, practices, concerns, or questions. Reports of the committee’s discussions and actions should be sent to the program’s management and kept on file.
Other duties of the Safety Committee include planning and presenting annual safety training, interacting with the program’s continuous quality improvement (CQI) and risk management systems, and tracking safety-related events. Information that results from the decisions and recommendations made by the Safety Committee should be communicated appropriately and, when indicated, incorporated into the program’s policies, procedures, and operations.
Safety Training
Operational Safety Training
All regular transport team members, and members of specialty teams who may also participate in transports, should receive regular operational safety training. Operational safety training should include air medical resource management (AMRM), mission planning, use of the program’s operational risk assessment tools, aircraft and ground vehicle safety, emergency scene operations, and survival. In addition to scheduled didactic sessions, operational safety training should include regular aircraft or ground vehicle emergency drills.
Clinical Safety Training
Clinical safety training should review flight physiology and the stressors of flight, hazardous materials (HAZMAT) recognition and response, infection control, and the management of combative or violent patients. These subjects are addressed in detail in other chapters of this textbook. Other safety training topics may include employee wellness, injury prevention, and specific topics required by state, federal or local statutes.
Aircraft Safety Training
All flight crew members must be familiar with the aircraft in use by their program, including all regular and back-up aircraft operated by the program in which the crew member may be expected to fly. Specific items with which all crew members must be familiar for all aircraft include:
▪ Operation of seatbelts or harness.
▪ Operation of all doors and emergency exits.
▪ Emergency egress procedures.
▪ Emergency engine shutdown.
▪ Emergency communications.
▪ Oxygen and medical gas shut-off.
▪ Location and operation of onboard fire extinguishers.
▪ Location and use of other onboard emergency equipment, such as the survival kit, personal flotation devices, and aviation emergency oxygen systems.
▪ Hot-loading and offloading procedures and policies.
Ground Ambulance Safety Training
Ground ambulance safety should be a part of training of both ground and air transport providers. Air medical crews often are expected to transfer patients from an airport or other landing site to the hospital via ambulance. Ground vehicle safety training should include:
▪ Driver training (where applicable).
▪ Use of seatbelts by all crew members while the vehicle is in motion.
▪ Avoiding standing or kneeling in the patient compartment.
▪ Oxygen and medical gas shut-off.
▪ When to use red lights and siren (RLS) response.
▪ Securing equipment in the ambulance.
▪ Gurney operations and back/lifting safety.
Occupational and Workplace Safety Training
All crew members must be familiar with the safety procedures and requirements of the assigned workplace, whether in a hospital, at an airport, or at another location. Items with which all staff need to be familiar include the location and type of fire extinguishers, use of the fire extinguishers, the process for refueling aircraft or vehicles, HAZMAT or fuel spill response, electric and gas shut off, occupational injury or illness reporting, and site-specific procedures or practices, such as emergency evacuation routes.
Outreach Safety Education
Along with safety training for transport program staff, safety training and practice must be provided for first responders and others who may be asked to work around EMS aircraft. These personnel may include fire service, law enforcement, EMS, and park rangers or game wardens.
SAFETY IN THE TRANSPORT ENVIRONMENT
Personal Safety
Personal safety is an important aspect of the safety attitude. For the individual crew member, personal safety is the mindset, habits, and daily practices that keep that individual safe. Each member of the transport team also bears the responsibility for the personal safety of others, including partner, pilot, patient, and fellow responders. For the transport service, personal safety means providing a safe work environment, appropriate personal protective equipment, and safety training and also involves establishing and following safety standards and policies. The best safety training and equipment in the world are of little value if not used properly, and safety standards cannot be effective if they are not followed.
Fitness Standards
The transport environment is physically challenging and requires that transport team members maintain a high personal level of both physical and emotional fitness. Requirements of each program vary, and no industry-wide formal guidelines exist. 53 Minimal physical requirements of any person working in the medical transport environment should include the ability to work within the space limitations of the transport aircraft and vehicles operated by the program, to lift and carry a reasonable amount of weight, and to function in the typical work environments encountered by the program, such as scene calls. Transport team members must not have any preexisting conditions that could interfere with flexibility, strength, or cardiovascular fitness. Transport team members also must not have any condition that could cause altered mental or neurologic function.
Fatigue Policies
Studies on the effects of fatigue on performance have shown that they are similar to the effects of alcohol. Fatigue has been found to be a factor in a significant number of aviation mishaps and accidents. It should be addressed in the same fashion as other risks, especially during night operations. 52 Transport programs need to have policies in place to address crew fatigue. Crew members should have the right to call time out from flight duties if they or a fellow flight team member feel that continuing duty is unsafe because of fatigue, no matter what the shift length. No adverse personnel action or undue pressure to continue should occur. 2,12
Pregnancy
Many women of childbearing age work in the transport setting. No existing industry standard is found regarding pregnancy employment policies. 17 The effects of high altitude, high noise levels, and vibration and the increased risk for injury in mishaps have been identified as potential risks to the fetus and maternal health. 36 Transport team members who are considering pregnancy should discuss these risks with their personal physician and program administration.
Personal Protective Equipment
The 1988 NTSB study recommended that air medical personnel who routinely fly EMS helicopter missions wear protective clothing and equipment to reduce the chance of injury or death in survivable accidents. 25 The ASTNA position papers have also endorsed the use of protective equipment. Protective equipment consists of helmets, fire-resistant uniforms, and boots.
Helmets
In the military, the use of flight helmets has been shown to protect significantly against head injuries. 15 Despite the obvious advantages afforded by flight helmets, acceptance in civilian air medical programs was not initially widespread. Reasons cited for not wearing helmets included high cost, uncertain benefit, and negative public relations. 33 However, a survey performed to determine the public’s perception of helmet usage found that patients and family members positively viewed the use of helmets by air medical personnel. 50 In recent years, the use of helmets by EMS pilots and flight crew members has become the accepted standard.
The flight helmet must be approved for use in helicopters. The chinstrap should hold the helmet firmly in place, and the liner needs to fit comfortably. Some manufacturers use customized liners that are molded to the individual’s head. The helmet visor should be kept in the down position as much as possible during flight.
Fire-Resistant Clothing
The goal of fire-resistant clothing is to minimize skin exposure to the intense heat of an aircraft fire. The uniform should have long sleeves and be made of a flame-resistant heat-resistant material such as Nomex. Flame-resistant fabrics are designed to withstand high temperatures for a brief period, usually less than 20 seconds, which permits the wearer to evacuate a burning aircraft or vehicle. 27 The fabric can reduce the risk or severity of tissue damage but does not prevent thermal injury to the skin.
Undergarments worn under the fire-resistant flight suit (including briefs, t-shirt, or long underwear) should be made of natural fibers, such as cotton, silk, or wool. 25 When exposed to flames, synthetic materials such as polyester or polypropylene melt and become embedded into the skin. The uniform should also fit to allow 0.25 inch of air space between the flight suit and undergarments. Nomex gloves protect the hands and should be considered by persons who wear fire-resistant uniforms.
Protective Footwear
Boots should protect the foot from punctures, lacerations, and thermal injuries and provide stability to the ankle on rough or uneven ground. Boots should be constructed of leather, or leather and Nomex, and extend several inches above the ankle. The sole should be thick and oil-resistant, and the boot should have a safety toe and shank. The boot should also have adequate ventilation to prevent moisture from being trapped.
Hearing Protection
The average sound level produced by a running helicopter is between 90 and 100 dB. The Occupational Safety and Health Administration (OSHA) regulations require employers to provide hearing-conservation programs for employees exposed to time-weighted average sound levels of 85 dB or greater. Hearing protection, such as earplugs, earmuffs, or the flight helmet, should be worn during high decibel exposures such as engine start-up, hot loading and unloading, extreme noise levels at some scenes, and around running aircraft at airports. Earplugs are smaller and less expensive, but noise protection varies with fit; custom-fitted earplugs provide the most noise reduction. Earmuffs offer more uniform protection but are more expensive, are not as easily carried or stored, and may be less comfortable than earplugs. A properly fitted flight helmet provides adequate hearing protection for most individuals and should be worn at all times while in flight. Active noise reduction (ANR, or noise canceling) circuitry or communications earplugs (CEP) can be added to most flight helmets to provide further noise attenuation.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:




Full access? Get Clinical Tree
