CHAPTER 15. General Principles of Trauma Management
Reneé Semonin Holleran and Steven W. Neher
Competencies
1. Demonstrate the ability to perform scene safety and trauma triage.
2. Perform a primary and secondary assessment of the injury.
3. Initiate critical interventions for the injured patient before and during transport.
T rauma is defined as injury to human tissue and organs from the transfer of energy from the environment. Injuries are caused by some form of energy that is beyond the body’s resilience to tolerate. 1,2 Regardless of gender, race, or economic status, unintentional injury is the fifth leading cause of death for all ages in the United States and the leading cause of death for those aged 1 to 44 years. 1,2 Approximately 164,112 deaths annually result from trauma. 3 Traumatic events are rarely accidental; most are actually preventable. 3 Thus, the term accident is no longer used in the trauma literature. Unintentional injuries are a major source of morbidity and mortality. For this reason, injury prevention has become a major public health goal. 24
The cost of trauma-related injuries has exceeded $400 billion annually in the United States. 4 These costs are accounted for by lost wages, medical expenses, insurance administration costs, property damage, fire loss, employer costs, and indirect loss from work. 4
INJURY DYNAMICS
The time elapsed from the actual injury to initiation of definitive care is key to patient survivability. One of the most important factors that has positively influenced morbidity and mortality rates of trauma is rapid transport; the addition of highly trained medical personnel has brought critical care management outside the trauma center to the rural hospital or the scene of the trauma.
The transport of the patient with multiple injuries requires in-depth knowledge and skills and expert prioritization and organization skills. A thorough understanding of the mechanisms of injury and the kinematics of trauma are essential for any transport team member caring for injured patients. Knowledge of these principles helps guide appropriate assessment and treatment.
History
One of the first steps in care of a patient with multiple injuries is a history of events preceding and following the traumatic event. With interfacility transfers, this information is most commonly obtained from other nurses, physicians, and family members. The history at a scene call generally comes from many individuals, including law enforcement, firefighters, and other emergency medical services (EMS) personnel and bystanders. 1
When responding via rotor-wing aircraft at the scene of a trauma, an aerial view of the situation helps the transport team to begin data collection about the patient (Figure 15-1). The transport team has the advantage of evaluating the entire scene, the damage sustained to the vehicles or the buildings, the extent of impact, and the objects thrown or blown out of the central area of impact.
 |
| FIGURE 15-1 When approaching a scene from the air, the transport team begins collecting information about the incident. |
At the scene, life-threatening injuries are always top priority, and a detailed history may be impractical in certain cases. However, the importance of a thorough history is vital to direct the patient’s care. Because time is a critical factor for survivability, the history should be obtained while gaining access to the patient or while simultaneously performing the primary assessment. If the patient has an altered level of consciousness, the only history obtained may be from the hospital or emergency personnel present, who may not be going to the receiving hospital. The history should be elicited during concurrent patient assessment because the team may never get another chance to obtain needed information. When appropriate, the mnemonic AMPLE is used to elicit a history from the patient.
A: Allergies
M: Medications currently used
P: Past illness or Pregnancy
L: Last meal
E: Events or Environment related to the injury
Additional important information includes time of incident, mechanism of injury, any alteration in the patient’s level of consciousness, and the patient’s medical history, current medications, and allergies.
A further detailed history may be obtained from the patient during the secondary survey as time and patient condition allow and can be routinely performed in the transport vehicle.
Mechanism of Injury
Injuries occur when external forces are applied to the body. The type and amount of injuring force and the tissue response to the force determine the extent of injury. 2 When the body’s tissue cannot withstand any additional force, destruction occurs, as evidenced by common injuries seen in the patient with multiple injuries: fractures, lacerations, and ruptured internal organs. A complete understanding of a force and the way it is applied is necessary to predict potential injuries and thus adequately care for the injured patient.
Newton’s first law of motion states that a body at rest tends to remain at rest and a body in motion tends to remain in motion until acted on by an outside force. When the body contacts an object, energy is transferred, and damage occurs (Figure 15-2).
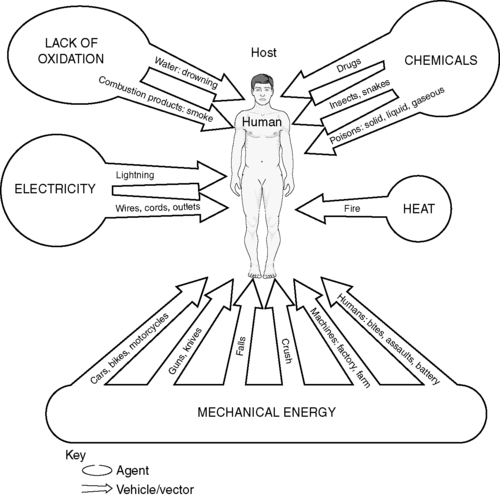 |
| FIGURE 15-2 Energy forces that can affect the human body. |
Force is a result of energy transference, which can be explained by the laws of physics.
1. Energy can be neither created nor destroyed; it can only change form.
2. Kinetic energy (KE) = (Mass × Velocity 2) / 2
3. Force = Mass × Acceleration
Because energy is neither created nor destroyed, it is transferred, and its transference is dependent on the mass of the object multiplied by the speed squared over a common denominator of 2. For example, an automobile that weighs 3000 lbs is traveling at 40 mph when it strikes a telephone pole.
The kinetic energy transferred in this impact to both objects is 2,400,000 units.
The same force is applied to destruction of the body. Energy is transferred from the automobile to the human. Several factors determine the amount of energy the human absorbs, including the following:
1. The amount of energy absorbed by the objects that initially collide (e.g., the telephone pole and the automobile).
2. The amount absorbed by protective factors, such as seat belts, helmets, padded steering wheels, dashboards, and airbags.
The forces involved in the impact cause varying degrees of destruction. The more slowly the force is applied, the less energy transference and the lower the degree of destruction. The extent of injury is also dependent on which body parts receive the impact. 19 For example; the skull can take more force before damage occurs than can the abdomen.
Force can be delivered via compression, acceleration, deceleration, or shearing. 19
Compression: Direct pressure on a structure is the most common type of force applied. The amount of injury sustained is dependent on the length of time of compression and the area compressed. 19
Acceleration/deceleration: Acceleration is the increase in the velocity of a moving object. Deceleration is the decrease in velocity of an object. 19 In an automobile crash, the body is thrown forward (accelerates) by the impact and decelerates as it comes in contact with the steering wheel, seatbelt, or dashboard. The internal organs initially also accelerate and decelerate as they come into contact with internal structures such as ribs, which causes destruction to the tissues and vasculature.
Shearing: Shearing forces occur when the tissues or organs or both are pushed ahead of underlying or overlying structures. The most common mechanism that causes a shearing injury occurs when a pedestrian is run over by a vehicle. As the vehicle grabs a part of the body, the area is pushed forward until it can no longer take the force, and it tears. Degloving routinely occurs from shearing forces.
The viscoelastic properties of tissues in the body help to absorb energy. When the energy delivered is below the limit of injury, the energy is absorbed and causes no damage. When the forces applied deliver more energy than the body can absorb, strains occur. 19 Strains may be classified as tensile, shearing, or compressive. Table 15-1 displays the characteristics and examples of each type of strain.
| Type | Reaction | Examples |
|---|---|---|
| Tensile | Stretching | Bony fractures, aortic tears |
| Shearing | Movement of tissue in opposite directions | Brain injuries, lacerations/avulsions |
| Compressive | Crushing force | Compartment syndrome, ruptures |
KINEMATICS OF TRAUMA
Patterns of injury have been identified with evaluation of the type of trauma that has occurred and the amount of force generated. Although all patients should be evaluated individually, certain injuries are common to certain forces. Prediction of these injuries is referred to as kinematics. Age, preventive measures taken, and velocity are factors in the alteration of injury patterns, and the caregiver should consider these factors in evaluation of a patient. 15
Blunt Injuries
Motor Vehicle Crashes
Motor vehicle crashes account for most injuries and deaths in 70% of the 39 countries for which data are available (Figure 15-3). 4
 |
| FIGURE 15-3 Motor vehicle crash. |
Head-on Collisions
As an automobile collides with another automobile or with any object head on, energy is transferred to the vehicle. The front of the vehicle routinely stops less than one-half second after impact. The rear of the automobile continues to move forward until all the energy is dispersed. Although the front end of the car is destroyed, the rear of the vehicle causes the destruction by its continued forward movement. The same principle of injury occurs with the body during a head-on collision. The initial impact occurs in the front of the vehicle. The unrestrained driver hits the steering wheel with the thorax, the head may hit the windshield, and the knees contact the dashboard (Figure 15-4). Predictable injuries from initial impact are fractured ribs, pneumothorax, or hemopneumothorax; concussion; skull fractures; patella and femur fractures; dislocated hips; and acetabular fractures. The progression of injury proceeds, as does the automobile, and the person’s internal organs are thrown from the rear forward until all energy is dispersed. Common injuries include ruptured spleens (direct compression from the steering wheel), lacerated livers (stretching of hilum until the tensile strength is exceeded), and ruptured thoracic aortas (heart and aorta are forcibly thrown forward, stretched, and then compressed against the ribs).
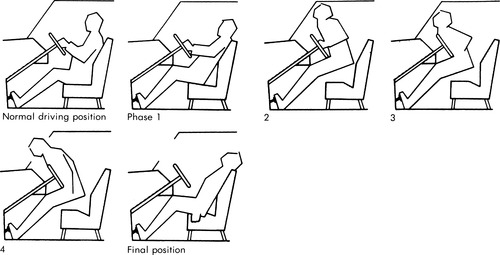 |
| FIGURE 15-4 Phases of movement of the unrestrained occupant during frontal collision. |
The restrained driver in a head-on collision has much of the energy absorbed by the seat belt and air bag, if present. The seat belt may impose a load 20 to 50 times as great as the body weight. The only portion of the human body capable of incurring this load is the pelvis. Unless the patient has the belt properly applied securely over the pelvis, direct compression of the abdomen may occur. The first indicator of these injuries is often the presence of abrasions over the abdomen from the seat belt. Other injuries associated with seat belt use include sternal fractures, breast injuries, and lumbar vertebral body fractures. As seen with abdominal seat belt injuries, abrasions or ecchymosis or both are important indicators. Lap belts should be worn with a diagonal shoulder strap to stop forward movement of the upper body. Diagonal straps worn alone can cause severe neck injuries, including decapitation. Air bags cushion forward motion only. They are effective in a first collision; but because they deflate immediately, they are not effective in multiple-impact collisions. When the air bag deploys, it can produce injury to the patient. The most common injuries seen are abrasions of the arms, chest, and face, which can include injuries caused by the patient’s eyeglasses. 12,19,23
Rear-end Collisions
An automobile hit from behind rapidly accelerates, which causes the car to move forward under the patient. Predictable injuries are to the back (T12-L1 is the most common area of injury), legs (femur, tibia/fibula, and ankle fractures), and neck (cervical strain, cervical fractures caused by hyperextension), if the head restraint is not in the proper position. If the automobile undergoes a second collision by striking a car in front of it, the predictable head-on injuries also need to be evaluated.
Side Impact
An automobile hit on the side routinely causes lateral injuries to the patient. An unrestrained driver hit on the side can have initial injuries to the left clavicle, ribs, femur, and tibia/fibula. Abdominal injuries, such as ruptured spleens, are seen in these crashes, usually because of the fractured lower lateral ribs, but also because of direct compression on the abdomen. 19 Secondary injuries occur when the patient is propelled to the other side of the car, which causes injuries to the opposite side.
Rollovers
Predictable injuries caused by vehicle rollovers are more difficult to define (Figure 15-5). The unrestrained patient tumbles inside the vehicle, and injury occurs to the areas of the body that are hit. The caregiver should always care for these patients judiciously and realize the potential for multiple-system injuries.
 |
| FIGURE 15-5 Rollover motor vehicle crash. |
Motorcycle Crashes
Because motorcycles offer minimal or no initial energy transference, energy is directly absorbed by the rider, and injuries are substantially more severe than with other motor vehicle crashes. The predicted injuries during a motorcycle crash, like those during other motor vehicle crashes, depend on the type of collision that occurs.
Head-on Collisions
For accurate prediction of injuries that involve the motorcycle rider, an understanding of the design of a motorcycle is helpful (Figure 15-6). The center of gravity is located in front of the driver’s seat. As the cycle strikes an object head on, the rear (or lighter) portion tips upward from the weight under the handlebars, which prevents the driver, who is propelled over the handlebars, from total ejection. Associated injuries with this type of crash are fractured femurs, tibias, and fibulas (from the handlebars); chest and abdominal injuries (from direct compression against the handlebars or tire); and head and neck injuries (from impact with the tire or any object in front of the cycle). Any motorcycle crash can cause the rider to be ejected, but ejection is most common during head-on collisions. As with ejection from any vehicle, the head acts as the missile. Suspicion of and intervention for major head and cervical spine injuries are imperative with any ejected patient.
 |
| FIGURE 15-6 Construction of a motorcycle places the center of gravity in front of the driver’s seat. Head-on collision causes the cycle to tip up and throw the occupant over the front. |
Side Impact
Injuries associated with a side-impact motorcycle crashes are related to the body parts crushed between the cycle and the second object. Most commonly seen injuries involve the leg and foot on the impact side. Open fractures of the femur, tibia/fibula, and malleolus are predictable.
Laying Down the Motorcycle
Motorcycle riders have learned the technique of laying down the bike and sliding off to the side before colliding with another object. The energy transference is a result of sliding away from the bike. Commonly seen are abrasions on the affected side. Fractures may occur if the patient hits the road hard or comes in contact with another object. Preventive clothing, such as leather jackets, pants, and gloves, absorb more energy than average clothing; in this type of impact, they may prevent abrasions.
Falls
Falls from heights greater than 15 to 20 ft are associated with severe injuries. In predicting injuries associated with falls, caregivers should understand the following:
1. The average roof of a one-story house is approximately 15 ft off the ground; a two-story fall is approximately 30 ft.
2. With a fall greater than 15 ft, adults usually land on the feet. At less than 15 ft, adults land as they fall; that is, if they fall head first, they land on the head.
3. Because small children have proportionally larger heads, no matter what the distance, they tend to fall head first.
The caregiver must estimate the distance fallen. Second, what the patient landed on must be determined. A soft landing surface, such as dirt or sand, absorbs much more energy than a hard surface, such as concrete.
Three predictable injuries are seen in falls. The forces involved are deceleration and compression. The first injury, calcaneus fractures, is caused by compression of the feet on impact. Second, as the energy dissipates after impact and the top of the body pushes down toward the point of impact, compression fractures to T12-L1 are seen. Finally, as the body moves forward and the patient puts out both arms to complete the fall, bilateral wrist fractures occur.
Penetrating Trauma
All objects that cause injury from penetration deliver the same two types of force: crushing and stretching.13,1,4,16 Depending on the velocity of the penetrating object, the wound can be small or massive.
Stab Wounds
Stab wounds are considered low velocity and produce the major damage by crushing tissues as the penetrating object enters. An object that is narrow at the beginning and thicker at the end crushes the tissues as it enters and stretches them apart as the thicker part is inserted. The area of injury for stab wounds is typically localized to the area of insertion. The penetrating instrument might remain embedded in the patient or might have been removed; embedded penetrating objects should be stabilized with bandages for transport and not removed (Figure 15-7).
 Only gold members can continue reading. Log In or Register to continue
Related posts:
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|


