CHAPTER 22 Wrist blocks
Clinical anatomy
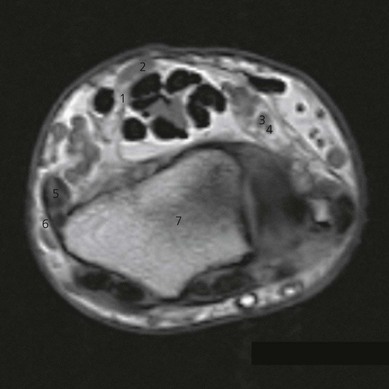
The hand is innervated by the three nerves that pass through the wrist (Fig. 22.1).
The median nerve approaches the wrist between the palmaris longus (if present) and the flexor carpi radialis. It can also lie beneath the palmaris longus (Fig. 22.2). The median nerve provides sensation to the lateral half of the palm, flexor aspect of the thumb, index finger, middle finger, and radial side of the ring finger.

The ulnar nerve, in the middle of the forearm between the flexor digitorum profundus and the flexor carpi ulnaris, gives off a dorsal and a ventral cutaneous branch. At the wrist, the ulnar nerve lies between the ulnar artery and the lateral border of the flexor carpi ulnaris (Fig. 22.2), which inserts on the pisiform bone. Near the pisiform bone, it passes superficial to the flexor retinaculum and ends by dividing into superficial and deep branches. The ulnar nerve provides sensation for the ulnar half of the back and front of the hand, little finger, and ulnar side of the ring finger.
The radial nerve at the wrist lies between the flexor carpi radialis and the radial artery (Fig. 22.3). The radial nerve provides sensation for the radial half of the dorsum of the hand, back of the thumb, and part of the dorsum of the index finger.

Surface anatomy
Bony landmarks include the ulnar styloid and the radial styloid carpal bones. Other landmarks include the wrist crease, flexor carpi radialis, palmaris longus, and flexor carpi ulnaris tendons (Fig. 22.4). These tendons can be accentuated by having the patient flex the wrist while making a fist. The radial artery can be palpated lateral to the tendon of the flexor carpi radialis, and the ulnar artery lateral to the flexor carpi ulnaris tendon.
Sonoanatomy
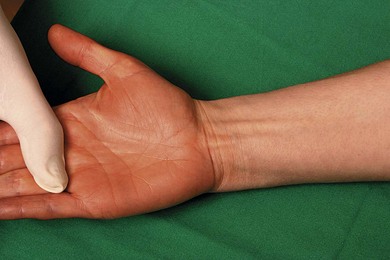
The examination begins with the patient supine, the arm abducted, the forearm and wrist in supination (Fig. 22.5). A systematic survey should be performed from superficial to deep and medial to lateral. A high frequency ultrasound transducer is used with a transverse orientation.

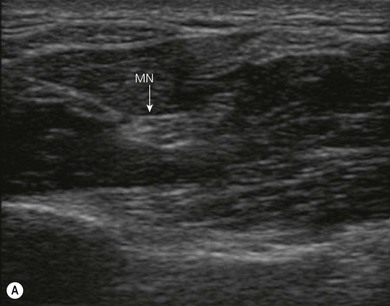
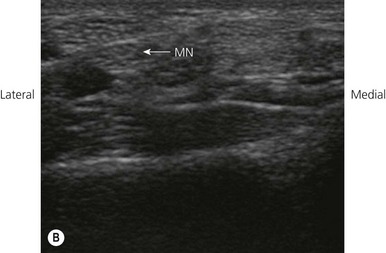
The median nerve passes distally in the volar aspect of the forearm between the flexor digitorum superficialis and the flexor digitorum profundus muscles (Fig. 22.6A). Approximately 5 cm proximal to the flexor retinaculum, the median nerve courses around the radial or lateral edge of the flexor digitorum superficialis, where its position becomes more superficial. Just proximal to the carpus, the nerve lies between the tendons of the flexor digitorum superficialis and the flexor carpi radialis, partially deep to the tendon of palmaris longus (if it is present; Fig. 22.6B). The nerve then passes deep to the flexor retinaculum into the carpal tunnel of the wrist.
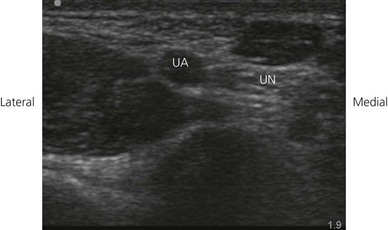
The ulnar nerve at the wrist lies within the Guyon canal, an oblique fibro-osseous tunnel, formed by the flexor retinaculum and palmar carpal ligaments, that lies within the proximal part of the hypothenar eminence. The canal contains the ulnar nerve, the ulnar artery with its venae comitantes, and loose fibrofatty tissue. On transverse sonograms, the ulnar nerve appears as a rounded structure with a location medial to the artery (Fig. 22.7).
< div class='tao-gold-member'>







Full access? Get Clinical Tree


