Emergency Management of Life-Threatening Problems
The “ABC’s” of resuscitation must be addressed before wounds are evaluated. Open wounds are dramatic and often draw the attention of the emergency physician or resuscitation team away from more life-threatening injuries. It is rare that bleeding from even large tissue defects will immediately impact the patient’s survival. Secure the airway, ensure adequate ventilation, and stabilize blood pressure prior to assessing wounds.
The simplest and most common method used to achieve hemostasis is direct pressure. A bulky dressing wrapped firmly with an elastic bandage will usually stop venous, capillary, and arteriolar hemorrhage. Most smaller arterial bleeding can be temporarily stopped with this method and larger bleeding vessels may be controlled with digital pressure. Large arteries may ultimately require vascular repair or suture ligation.
The decision to ligate an artery should be made cautiously; any uncertainty as to the impact on distal tissue perfusion should prompt consultation of the appropriate surgical specialist. Proximal extremity arterial injuries require emergency vascular surgery consultation.
Simple tying or suture ligation is indicated for most vessels more than 2 mm (1/16 in)in external diameter. To avoid excessive tissue trauma, one must precisely identify and clamp the vessel end prior to ligation. Severed arteries usually require only simple tying. Veins, however, do not hold ligatures well, and suture ligation is preferable. Suture ligation may be performed by passing the suture needle through a portion of the vessel wall and then circumferentially tying the vessel. This method prevents slippage of the ligature. Caution: Do not ligate arteries and veins en masse, because this may predispose to arteriovenous fistula formation. Absorbable sutures are preferred for tying and suture ligation in the acute wound. Synthetic absorbable sutures (polyglycolic acid [Dexon] and polyglactin [Vicryl]) are advantageous because of their low reactivity and high friction coefficients. Chromic catgut is also satisfactory.
Inflatable cuff tourniquets can be used for temporary hemostasis during wound exploration and repair but are not recommended for periods over 20–40 minutes. Inflate the pressure cuff on the extremity proximal to the wound until hemostasis is achieved. Take particular care to remove tourniquets after 15–20 minutes and before the procedure is completed to check for residual bleeding. A tourniquet inadvertently left in place may cause permanent ischemic damage to the limb.
Epinephrine-containing local anesthetic agents such as lidocaine or bupivacaine are commonly used to control bleeding prior to wound repair. This can particularly be useful in highly vascular areas such as the scalp where bleeding can be difficult to control.
Surgical mono- and bipolar electrocautery units cause hemostasis through thermal coagulation of blood and tissue. The resulting tissue damage lessens the appeal of this technique. Disposable hand-operated electrocautery units are also available.
Rarely, bleeding from a scalp wound cannot be stopped using direct pressure or by infiltration of epinephrine-containing anesthetic agents. This is particularly true when tissue maceration has occurred due to blunt trauma. In this instance, it may be necessary to place deeper 2-0 or 3-0 absorbable sutures after wound cleansing to close the tissue defect and place an external pressure dressing. If a significant hematoma forms, it may be necessary to reexplore the wound and place an external drain.
When time allows, a closure with a running, locking 2-0 or 3-0 nonabsorbable suture may provide the best hemostasis and wound closure simultaneously.
Silver nitrate and other caustics achieve hemostasis through tissue coagulation but are not recommended for wound hemostasis because of the amount of tissue necrosis they produce. American military forces are testing newer forms of powdered and gel adhesive procoagulants. Some of these generate high temperatures due to an exothermic chemical reaction, and reports of thermal tissue damage may limit utility in the civilian sector.
1This chapter is a revision of the revision by David A. Fritz, MD, FACEP, from the 6th edition.
Wound Assessment
A detailed, thorough history is essential for assessing the extent of injury and for organizing appropriate wound management. Three basic questions are used to reconstruct the history of the injury.
The time of injury is important for determining the interval between injury and treatment. Most civilian injuries contain fewer than 105 bacteria per gram of tissue in the first 6 hours and are therefore relatively safe to close. Wound repair after 6 hours is dependent on many factors, including vascularity of the area, degree of contamination, and health status of the patient. The longer the wound has been present, the more likely an infection will occur after primary closure. As a rule, tissue resistance to infection is directly proportionate to blood supply. Facial lacerations may often be closed safely within 24 hours of injury, owing to the abundant blood supply in that area.
What were the possible contaminants associated with the injury? Contact with feces, pus, saliva, or soil greatly increases the risk of infection and should be considered when deciding on timing of closure.
The potential damage to deeper structures can be estimated by review of the mechanism of injury. Any high-velocity-missile injury has the potential to damage deeper structures, and the wound tract should be assessed carefully. Blunt injuries may crush tissue and fracture underlying bone, leaving an open fracture, compartment syndrome, or arterial disruption.
Lacerations cause minimal tissue injury and are relatively resistant to infection.
Puncture wounds may become infected, especially if they are contaminated or if a foreign body is present.
Stretch injuries can produce damage to blood vessels, nerves, ligaments, or tendons, which is not visible superficially.
Compression or crush injuries result in the greatest amount of tissue necrosis. Hemorrhage into the soft tissues is common, resulting in ecchymosis and hematoma formation. The crushed tissue has a markedly impaired ability to heal and resist infection. Depending on location, these injuries are at high risk to develop compartment syndrome.
Bites are heavily contaminated and may require delayed closure.
Complications arising from wound care are a common basis for malpractice claims against emergency physicians. Inspection should be conducted in an emergency care or surgical facility where adequate lighting and equipment are available. Wound hemostasis must be achieved for proper evaluation of involved structures and to rule out foreign bodies. The extra time spent in preparing the proper environment for wound examination often decreases total procedure time by facilitating the repair. Sterile technique and gentle handling of tissues are mandatory to avoid additional tissue injury or contamination.
If deep injuries cannot be assessed adequately through the existing surface defect, consider extending the laceration by undermining the skin beyond the wound edges with a scalpel. Obtaining sufficient exposure of the wound may reveal tendon injuries, joint capsule penetration, or foreign bodies.
In assessing the type and extent of injury, consider the following questions:
- Is there loss of function in the injured part?
- Are important underlying structures involved such as nerves, major blood vessels, ducts, ligaments, bones, or joints?
- What is the level of contamination in the wound?
- Are any foreign bodies present?
- What is the viability of the injured parts? Are any parts missing?
The viability of an avulsion flap depends not only on the vascularity of the flap but also on the length versus base ratio, maceration of the tissue involved, and vascularity of the surrounding tissue. A long flap of badly macerated tissue with a narrow base will probably not survive and should be excised while a clean, short flap on the face will almost certainly heal uneventfully.
The blood supply to the scalp is excellent and wound infections rarely occur. The physician should examine scalp wounds carefully to ensure that the galea is not involved. Galeal lacerations should be cleaned and sutured with absorbable suture to prevent subgaleal hematoma formation and subsequent infection.
Facial wounds can have dramatic effects on a patient’s appearance; every effort should be made to minimize scarring and to prevent tissue loss. Debridement of facial tissue is rarely necessary and may cause distortion of features as the scar matures. Take special care with ear, eyelid, and nasal lacerations. Experienced emergency physicians maintain a low threshold for consulting their plastic surgery colleagues on complicated facial wounds.
Deep injuries to the neck frequently involve important underlying structures (Chapter 23). These complex anatomic areas cannot be extensively debrided without major functional or cosmetic loss. Wound evaluation and repair are often best done in the operating room by a maxillofacial, otolaryngology, or general surgeon.
Wounds of the chest and abdomen must be evaluated for possible communication with a body cavity as well as internal organ injury (Chapters 24 and 25).
Hand injuries represent a significant proportion of emergency department patients and require special attention. Loss of function of even one digit can permanently impair a patient’s ability to perform their vocation or avocation. Apparently minor puncture wounds may injure nerves, tendons, or arteries and cause significant impairment if not diagnosed during the initial presentation. Perform a complete neurovascular examination of every significant hand injury including function of the median, ulnar, and radial nerves (motor, light touch, and two-point discrimination); intrinsic hand muscles; extensor and both deep and superficial flexor tendons; radial and ulnar artery pulses; capillary refill; and wrist flexors and extensors.
Wounds on the plantar surface of the foot are particularly prone to infection. After thorough wound cleaning many emergency physicians will allow these wounds to heal without primary repair.
After initial assessment, cover the wound with a sterile dressing until definitive management, or further evaluation can be performed. Obtain any necessary X-rays only after the wound has been protected from the possibility of additional contamination. If considerable delay in definitive evaluation and management is anticipated, the wound should be cleaned, conservatively debrided, and temporarily closed or covered. Extensive wounds—or minor ones involving major structures—are best evaluated and managed in the operating room.
Perform a careful sensory and motor neurologic examination before administering anesthetic.
Local anesthetics have varying attributes with regard to safety, potency, duration of action, and effects on the local wound milieu (Table 30–1). Lidocaine is perhaps the safest local anesthetic, because allergic reactions are rare. The major problem with all local anesthetics is systemic absorption resulting in cardiovascular and central nervous system toxicity. For an adult, the maximum safe dose of 1% lidocaine without epinephrine is 5 mg/kg (do not exceed 300 mg) and for 1% lidocaine with epinephrine, 7 mg/kg (do not exceed 500 mg). For children, the safety and efficacy of lidocaine and mepivacaine are known; child safety and efficacy of the other drugs in Table 30–1 are not known.
| Cocaine | Procaine (Novocain) | Tetracaineb (Pontocaine) | Lidocaine (Xylocaine, Many Others) | Bupivacaineb (Marcaine, Sensorcaine) | Mepivacaine (Carbocaine) | |
|---|---|---|---|---|---|---|
| Potency (compared to procaine) | 3 | 1 | 10 | 2–3 | 9–12 | 1.5–2 |
| Toxicity (compared to procaine) | 4 | 1 | 10 | 1–1.5 | 4–6 | 1–1.5 |
| Stability at sterilizing temperature | Unstable | Stable | Stable | Stable | Stable | Stable |
| Total maximum adult dose | 100–200 mg | 500 mg | 50–100 mg | 300 mg | 175 mg | 400 mg |
| Total maximum pediatric dose | — | — | — | 4 mg/kg | — | 5 mg/kg |
Infiltration
|
|
|
|
|
|
|
Nerve block
|
|
|
|
|
|
|
Topical anesthesia is especially useful in the management of small wounds in children who do not tolerate local infiltration. A commonly used combination solution is LET (lidocaine, epinephrine, and tetracaine). TAC (tetracaine, adrenaline, and cocaine) has been largely abandoned due to risks of systemic toxicity and potential abuse. To apply the solution, soak a gauze pad in it and place the pad directly over the wound for 20 minutes. Do not use over mucous membranes or areas with end-arterial circulation (fingers, toes, nose, and penis). Anesthesia can often be judged by the appearance of blanching at the wound site. Use the minimal amount of anesthetic necessary.
Inhalation anesthesia with nitrous oxide administered by experienced personnel can be a useful adjunct, especially for children.
Infiltration of a local anesthetic agent is performed gently near the edge of the wound or directly into the wound with a small (No. 25–30) needle (Figure 30–1). Pain associated with local infiltration is partly due to the stretching of sensitive nerve endings in the dermis and may also be due in part to the difference in acidity of some anesthetics (the pH of commercial preparations of lidocaine is 5–7). Associated pain can be reduced by using smaller amounts of more concentrated anesthetic solutions and slower infiltration rates or, in the case of lidocaine, by preparing it as a buffered solution (9 mL of 1% lidocaine, to which 1 mL of sodium bicarbonate solution, 44 mEq/50 mL, is added). Restrict the dose of anesthetic to the least amount that will provide adequate anesthesia. This is particularly true for facial lacerations, where infiltration distorts important landmarks and makes precise matching of wound edges difficult. Infiltration of anesthetic directly into the wound is less painful but may spread infection in heavily contaminated wounds.
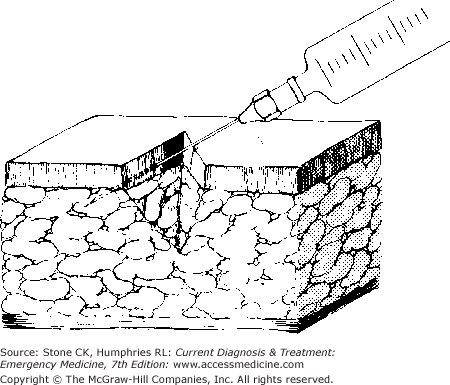
Injecting a small skin wheal and then advancing slowly, pausing to let each increment of tissue become anesthetized, is a more time-consuming method but less painful to the patient.
Regional anesthesia (sensory nerve blockage at a site proximal to the wound) is more technically challenging than local anesthesia, but it provides a larger anesthetic area and allows more extensive exploration and manipulation of the tissues. Because local wound anatomy is not distorted by regional block, more precise alignment of wound edges is possible. Onset of anesthesia is a function of the type of agent used and how close to the nerves the agent is injected. The duration of anesthesia can be prolonged with epinephrine; however, epinephrine should not be used for digital nerve blocks. Regional anesthesia is particularly suitable for extremity injuries complicated by heavy contamination or in extensive injury requiring long operating times for repair. It is also used in patients who are not good candidates for general anesthesia.
Pitfalls of regional anesthesia include difficulty in placing the anesthetic close to the supplying sensory nerve; loss of valuable time in waiting for it to take effect; and risk of permanent injury to the nerve from direct infiltration of anesthetic into the nerve.
Several techniques for regional blocks in hand surgery are described below. Whatever the method used, a thorough understanding of anatomy is crucial. Avoid probing injections because of the risk of paresthesias. Attempt to infiltrate the anesthetic without penetrating the nerve sheath, because this may injure the nerve.
Use a 25- or 27-gauge needle; larger needles may cause significant nerve injury. Wait about 10 minutes for the full anesthetic effect in digital blocks and 20 minutes for wrist blocks.
The technique requires two separate needle sticks with four injections of 1 mL of 1% lidocaine next to the nerve bundle of all four digital nerves. The needle is first inserted dorsally to block the dorsal digital nerve and is then redirected without removal toward the volar nerve and the anesthetic is injected. The procedure is repeated on the opposite side of the digit.
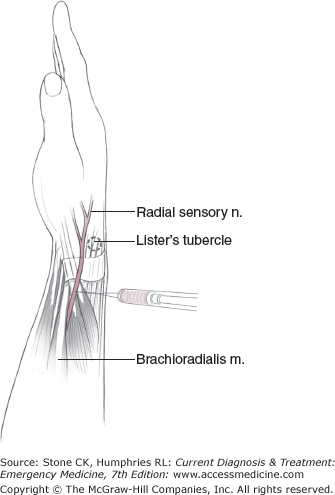
The radial sensory nerve emerges beneath the brachioradialis tendon (Figure 30–2) about 6 cm (2 ⅜ in) above the Lister tubercle. Inject about 4 mL of lidocaine in a 2-cm (¾ in) wide band 4 cm (1 in) above the Lister tubercle.
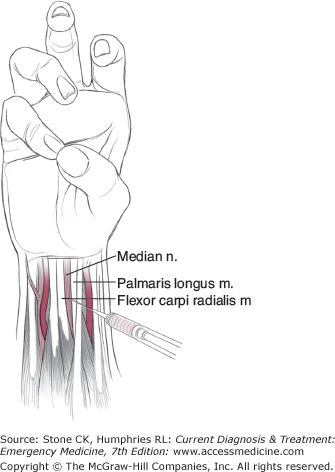
The median nerve at the wrist lies just radial and deep to the palmaris longus tendon and the transverse carpal ligament (Figure 30–3). The palmaris longus, when present, is easily identified by having the patient make a fist and flex the wrist. Insert the needle dorsally and distally between the palmaris longus and flexor carpi radialis, and inject 4 mL. The lidocaine can be milked into the carpal tunnel to achieve the maximum blocking effect.
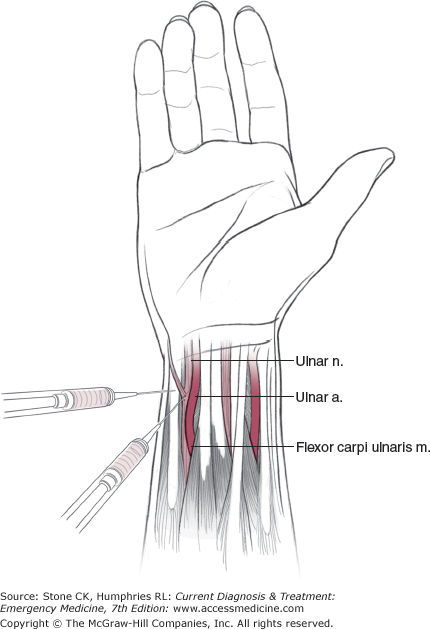
The ulnar nerve and artery course just dorsal to the flexor carpi ulnaris at the wrist (Figure 30–4). Avoid inadvertent injection of anesthetic into the artery by aspirating as the needle is advanced. Inject 2 mL on the ulnar side of the flexor carpi ulnaris. An additional 2 mL should be injected on the radial side to achieve a total block.
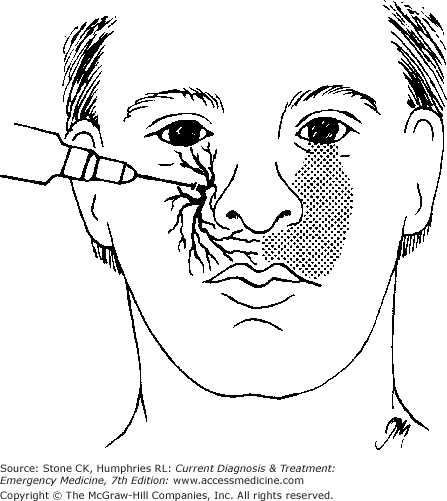
The infraorbital foramen can be easily palpated along the anterior maxilla and lies along a line drawn between the pupil and the maxillary canine. Inject about 1–2 mL as the needle is advanced from a lateral to a medial direction (Figure 30–5). Avoid penetrating the nerve by being careful not to enter the foramen. An intraoral approach may also be used. Wait for symptoms of numbness of the upper lip. Infraorbital nerve block provides anesthesia of the cheek, upper lip, and parts of the nose.
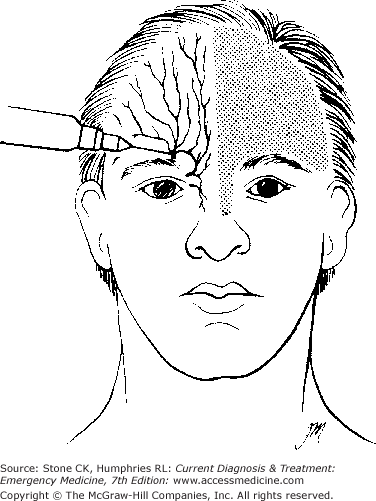
The exit of the supraorbital nerve from the orbit is readily identified by palpating the supraorbital notch. Inject a total of 1–2 mL of anesthetic about 0.5 cm (3/16 in) above the orbital rim (Figure 30–6). Advance the needle from a lateral to a medial direction, and avoid penetrating the nerve. If both supraorbital and infratrochlear blocks are needed, the wheal should be extended medially toward the midline. Supraorbital block is useful in anesthetizing the forehead.
Wounds in hairy areas are difficult to debride and suture, and hair in a wound acts as a foreign body, delaying healing, and promoting infection. Shaving hair around wound edges facilitates management but invites wound infection if the infundibulum of the hair follicle is injured. Contamination can be minimized by clipping the hair 1–2 mm (1/16 in) above the level of the skin. Depilatory agents and special razors equipped with recessed blades also allow safe removal of hair without infundibular injury.
A method of scalp laceration repair using the native hair to tie wound edges together has been described and seems to have no increased risk of infection when compared to standard suture repair. Reports of the hair spontaneously untying have led some physicians to place a drop of skin adhesive to the hair after tying.
Caution: Eyebrow and eyelash hair should never be removed, since removal destroys critical landmarks and makes accurate alignment of wound edges difficult. Misalignments may cause notch or step-off deformities in the brow line. Eyebrow hair also regrows slowly, creating a cosmetic problem.
As an adjunct to surgical debridement, mechanical cleansing of the wound by irrigation or scrubbing is quite effective. Soaps and detergents should not be used in the open wound in conjunction with mechanical cleaning.
The most reliable and well-tested method of emergency wound cleaning is high-pressure irrigation with normal saline. Pressures of 7–11 lb/in2 must be achieved to mechanically remove bacteria and particulate debris.
Numerous commercial devices are available for high-pressure irrigation, but the simplest and least expensive is syringe irrigation. A 35- or 50-mL syringe and a 19-gauge or blunt needle connected to a reservoir of irrigating fluid by a three-way stopcock are suitable. Commercial splash guards are also available, which attach to a syringe and allow for the requiredpressure while providing protection from bodily fluids.
Bulb syringe irrigation has been shown to be no more effective in preventing wound infection than no irrigation at all. Soaking wounds in saline does not remove bacteria and may allow for further contamination of the wound. The commonly used method of puncturing holes in the cap of a plastic liter bottle of saline and squeezing the contents into the wound does not achieve the necessary pressure to remove significant amounts of bacteria and should no longer be used.
Normal saline (or similar balanced crystalloid solution) is forcefully injected close to the wound surface and perpendicular to the surface of the skin. The amount of irrigant used depends on the size of the wound and the suspected extent of contamination.
Since large volume irrigation is preferred, when the wound can be placed under a faucet supplied by chlorinated city water, the wound may be irrigated in this fashion since studies have not shown an increased risk of infection as compared with sterile saline.
Sponge—Mechanical scrubbing of the wound surface is usually best performed with a highly porous sponge. Sponges routinely used for hand washing work well. Brushes and low-porosity sponges decrease the wound’s resistance to infection.
Brush—“Abrasion tattooing,” in which debris is embedded in the skin, requires vigorous scrubbing or dermabrasion to remove embedded debris. Soaps and detergents should not be used.
Cleanse the wound and surrounding skin to remove transient microflora, gross debris, coagulated blood, and the like.
In most instances, simply washing the open wound with saline under pressure (see above) removes most of the surface bacteria.
Related posts:






Full access? Get Clinical Tree


