Chapter 13 The complaint of weakness is common in emergency department (ED) patients and may be vague, subjective, and difficult to characterize. True loss of strength from a neurologic or muscle fiber lesion must be distinguished from other systemic conditions that result in fatigue, dyspnea, or imbalance because of inadequate substrate delivery to the nervous system or muscle unit. Such conditions may be described as weakness by the patient but are likely caused by cardiovascular, pulmonary, infectious, or metabolic processes. This chapter focuses on the evaluation of acute neuromuscular weakness; it may be focal or generalized and may originate in central or peripheral nerves, the neuromuscular junction (NMJ), or myofibers themselves. Other chapters provide more detail on peripheral nerve (Chapter 107) and neuromuscular disorders (Chapter 108). The epidemiology of weakness is closely linked to the epidemiology of other diseases and medical conditions. Although weakness can be a presenting problem at all ages, patients who are elderly or chronically ill are more likely to develop weakness. Advanced diabetes, cardiovascular and pulmonary diseases, chronic infectious diseases, and cancer may produce neuromuscular weakness through secondary effects on the brain and neuromuscular system. Brain, spinal cord, peripheral nerve, and neuromuscular causes of weakness are much less common than weakness that is secondary to other medical conditions.1 There are a number of physiologic considerations for the patient with diffuse weakness (Box 13-1). Conditions that have only peripheral effects at the NMJ and muscle have preserved reflexes. If by history, physical examination, and bedside ancillary testing the patient does not appear to have derangements in intravascular volume or cardiopulmonary function, metabolic abnormalities, or a source of infection, the investigation turns to a neural or primary muscular cause for weakness. Often these patients will have some asymmetrical finding on their neurologic examination. The critical and emergent diagnoses for neuromuscular weakness are listed in Table 13-1. Table 13-1 Critical and Emergent Causes of Neuromuscular Weakness Deciphering loss of muscle power means following the pattern of a patient’s weakness from the myofiber back to a particular site within the central or peripheral nervous system (Fig. 13-1). Common clinical patterns of weakness can be classified and assessed as discussed in the following sections. This presentation is generally caused by a lesion in the contralateral cerebral cortex or the CSTs coursing down the corona radiata and forming the internal capsule. Mild forms can be limited to a loss of dexterity and coordination with hand movements. Moderate loss of power is termed paresis, and complete loss of motion is termed plegia. UMN signs are useful corroborative findings but may not always be present. Sensory disturbances commonly occur over the areas of weakness. Look for associated neglect, a visual field cut, or an expressive or receptive aphasia to localize the problem to the cortex.2 Patients with equal loss of strength to the face, hand, and leg are more likely to have a subcortical lesion disrupting all of these fibers as they funnel close together in the internal capsule. Concomitant headache is suggestive of a brain hemorrhage or mass lesion.3 Sudden onset of this weakness pattern implies hemorrhage or ischemia, whereas a gradual onset may be seen in demyelination or neoplasm. This pattern indicates a brainstem lesion. A careful cranial nerve (CN) examination can provide more clues. If the patient has contralateral facial findings, there will likely be ptosis (CN III or sympathetic fibers) or a facial droop with forehead involvement (CN VII nucleus). Signs of CN V, VI, VIII, IX, or XII dysfunction will help to localize to a particular level within the brainstem.4 Cerebellar findings or nystagmus may also be present on examination. Sensory disturbances can parallel the weakness, and some patients will report double vision, trouble swallowing, slurred speech, vertigo, or nausea and vomiting. The CST courses ventrally through the brainstem, and extremity weakness with UMN signs in the involved limbs may accompany brainstem lesions. Depressed consciousness can also occur if the brainstem reticular activating system is involved. The two main underlying processes that cause unilateral extremity weakness with contralateral facial involvement are vertebrobasilar insufficiency and demyelinating diseases.
Weakness
Perspective
Epidemiology
Pathophysiology
Differential Considerations
Critical Diagnoses
Cerebral cortex or subcortical
Ischemic or hemorrhagic cerebrovascular accident (CVA)
Brainstem
Ischemic or hemorrhagic CVA
Spinal cord
Ischemia, compression (disk, abscess, or hematoma)
Peripheral nerve
Acute demyelination (Guillain-Barré syndrome)
Neuromuscular junction
Myasthenic or cholinergic crisis
Botulism
Tick paralysis
Organophosphate poisoning
Muscle
Rhabdomyolysis
Emergent Diagnoses
Cerebral cortex or subcortical
Tumor, abscess, demyelination
Brainstem
Demyelination
Spinal cord
Demyelination (transverse myelitis)
Compression (disk, spondylosis)
Peripheral nerve
Compressive plexopathy (hematoma, aneurysm)
Paraneoplastic vasculitis uremia
Muscle
Inflammatory myositis
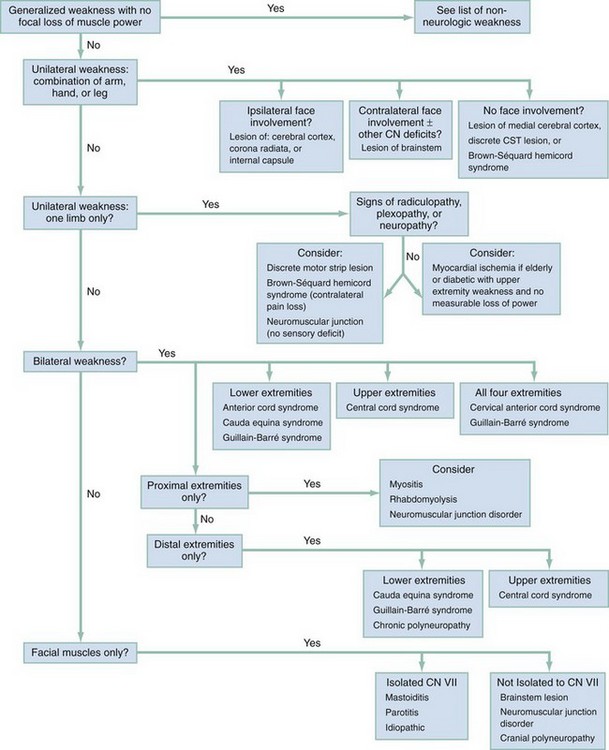
Diagnostic Algorithm
Unilateral Weakness with a Combination of Arm, Hand, or Leg with Ipsilateral Facial Involvement
Unilateral Weakness: A Combination of Arm, Hand, or Leg but with Contralateral Facial Involvement

Full access? Get Clinical Tree


Weakness
Only gold members can continue reading. Log In or Register to continue




