CHAPTER 51
Viscosupplements and Steroid Injections
INTRODUCTION
Steroids and viscosupplements (VS) are two commonly injected substances used to provide mobility of and relief to osteoarthritic joints. Steroids presumably provide relief by controlling inflammation of peripheral joints, while VS seek to reestablish the elasticity and viscosity of the joint’s normal synovial fluid. VS are also reported to have anti-inflammatory effects through the reduction of leukocyte function and inflammatory mediators.1,2 The efficacy of both injections for temporarily alleviating joint pain has been demonstrated in various clinical trials.3–5
The FDA approved the use of VS in 1997 for the treatment of knee osteoarthritis (OA) and VS have since gained widespread use.6 Although off-label use of VS occur in everyday clinical practice, such as its use for hip and shoulder,7,8 this chapter will focus on the use of these agents for their current FDA indication, the treatment of knee OA.9
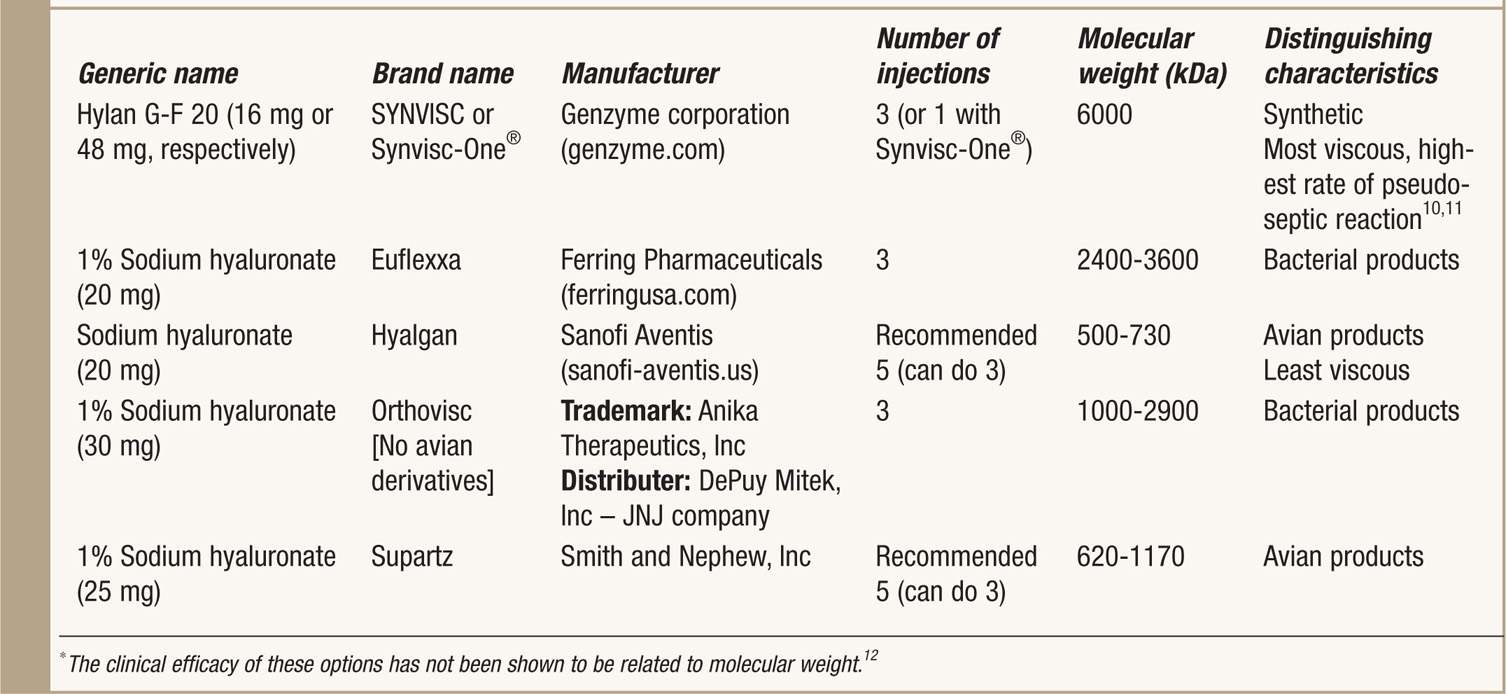
See Table 51-1 for a list of current FDA-approved VS.
TABLE 51-1. Manufacturer and Brand Information for Viscosupplements
INDICATIONS
According to the American College of Rheumatology (ACR), the indications for treating a swollen inflamed knee are:
• Failed conservative measures (oral medications such as nonsteroidal anti-inflammatory drugs (NSAIDs), physical therapy, activity modifications, and other lifestyle changes).
• Patients who have or are at higher risk for developing NSAID-induced renal dysfunction or gastroduodenal ulcers are excellent candidates for intra-articular steroid injections because they avoid the potential systemic effects that occur with oral NSAIDs.
If there is persistent pain and impaired quality of life following a knee steroid injection, or only short-term benefit from the steroid injection, then VS is the next treatment option to consider. Although steroid injections are reported to have quicker acting pain relief than VS, VS-derived pain relief may last considerably longer, from 4 to 26 weeks.13,54 Therefore, in some cases the patient will experience short duration but significant relief following a knee steroid injection and this duration of relief may be extended with the use of knee VS injection(s).
The clinical criteria for the diagnosis of knee osteoarthritis based on anatomical location of pain include14,15:
• Persistent knee pain that typically worsens with weight bearing and activity
• Morning stiffness
• Tenderness of the bony margins of the joint
• Bony enlargement
• Crepitus with motion
• Lack of palpable synovial warmth
Radiographic evidence of knee osteoarthritis, including the presence of osteophytes, subchondral cysts, and joint space narrowing, helps to confirm or support clinical suspicion.
Recent findings suggest that the most useful diagnostic criteria are:
• Three symptoms: persistent knee pain, limited morning stiffness, and reduced function
• Three signs: crepitus, restricted movement, and bony enlargement
Assuming a 12.5% background prevalence of knee OA in adults aged ≥45 years, the estimated probability of having radiographic knee OA increased with increasing number of positive features to 99% when all 6 symptoms and signs are present.16
RELEVANT ANATOMY
A thorough understanding of intra-articular and extra-articular knee structures and three-dimensional surface anatomy is absolutely necessary in the management of various knee conditions and intra-articular knee injections. This will provide the clinician with the ability to locate the site of needle entry and then allow for proper navigation of the needle into the joint space.17
The key landmarks to identify before considering an intra-articular knee injection are (Figure 51-1):
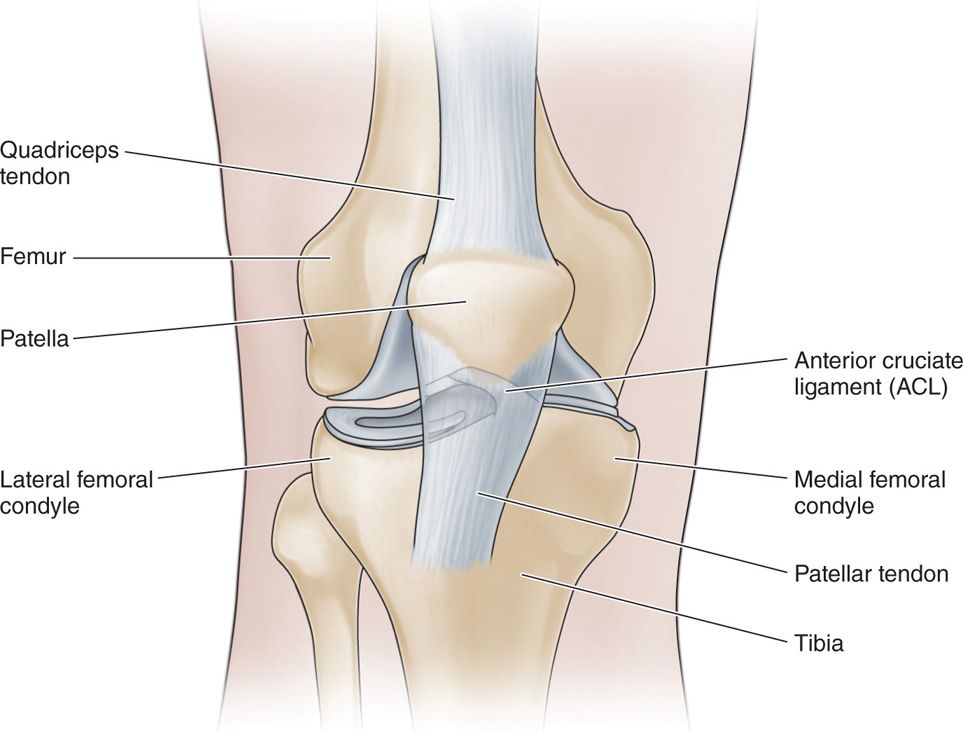
Figure 51-1. AP view of knee.
• Patella, including the inferior, superior, medial, and lateral poles
• Femoral condyles (medial and lateral)
• Tibial plateau (medial and lateral)
• Quadricep tendon
• Patellar tendon
Other relevant anatomy that should be considered prior to and during the injection is:
• A thorough understanding of the location of the synovial lining/joint capsule (Figure 51-2).
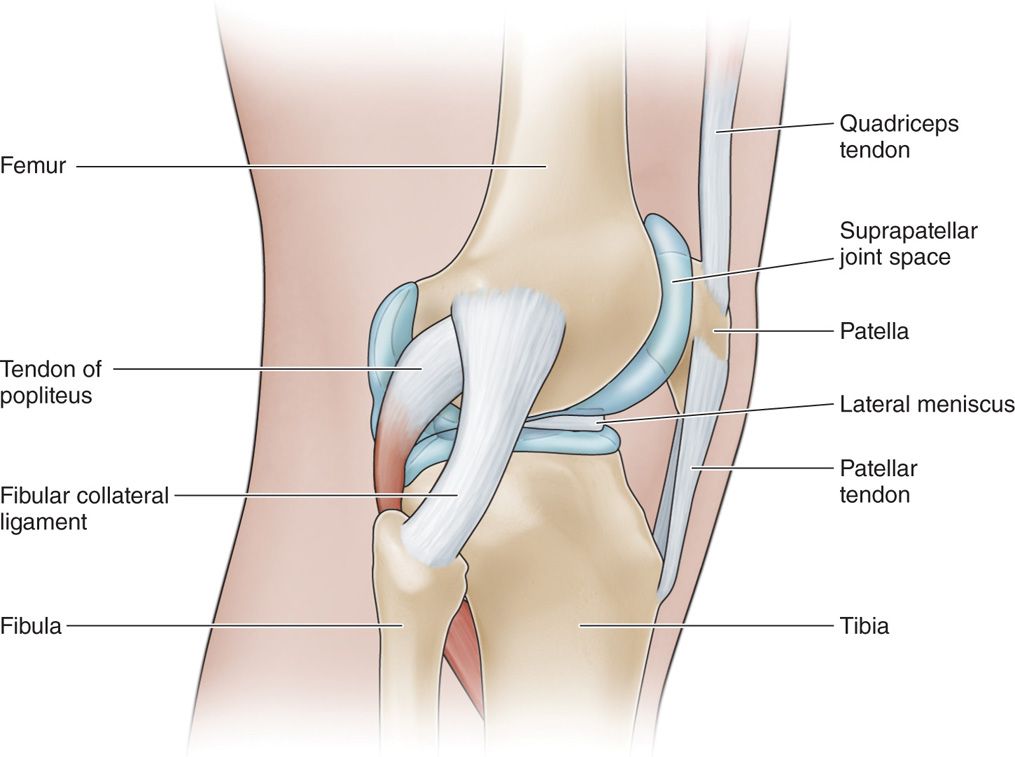
Figure 51-2. Lateral view of knee.
• The infra-patellar fat pad is important to understand and consider, depending on the injection approach utilized.
• Medial and lateral meniscus
• Medial and lateral collateral ligaments
• Quadriceps, including vastus lateralis and medialis
BASIC CONCERNS AND CONTRAINDICATIONS
Steroid injections and viscosupplements are routinely recommended after other conservative measures have failed to provide adequate relief of symptoms for patients with knee osteoarthritis. In the majority of cases, the potential benefit greatly outweighs the potential risks and these injections are well tolerated and have an excellent safety profile.4 The patients with significant medical comorbidities and multiple medications may be more susceptible, and certain adverse events and the risks/benefits of the procedure must be reassessed. Therefore, the medical history of each patient must be considered before administration to avoid further complication.
Basic concerns for the injections include:
• Injection of steroid or VS in intravascular or extra-articular areas from inaccurate needle placement can result in local and systemic complications.
• Patients may experience postprocedure pain at the site of the injection.
Some contraindications include:
• Infection, systemic or localized
• Coagulopathy
• Distorted or complicated anatomy (may be an indication for image guidance, even contrast enhancement)
• Patient refusal
• Known hypersensitivity to hyaluronan
• Product specific (Hyalgan, Supartz): Known allergy to avian products
• Product specific (Orthovisc): Known allergy to gram-positive bacterial proteins
INTRA-ARTICULAR KNEE INJECTION FOR ASPIRATION/STEROID INJECTION
Preoperative Considerations
• Informed consent and proper explanation of all potential complications.
• Anticoagulation. This is less of a concern than for spinal injections but since there is trauma to the tissues from the introduction of a needle both subcutaneously and intra-articularly, there is an inherent risk for hematoma or hemarthrosis.
• Physical examination of the area for signs of infection or skin breakdown, and the ability to properly palpate bony landmarks of the knee.
• Patient must be able to lie supine for brief procedure. The head of the bed/examination table may be slightly elevated for patient tolerance during the procedure.
• Intravenous access is not necessary but may be considered if the patient has a history of vasovagal reaction and hypotension responses post injection.
Efficacy of the injections is dependent upon accurate needle placement in the joint space, and not by patient’s age or gender. The knee joint can be accessed through a multitude of approaches and the majority of studies show that there is no significant difference in the accuracy of needle placement between the various approaches.18,19
Fluoroscopic or Ultrasound Guidance
Fluoroscopic or ultrasound-guided injections generally are not necessary since accurate knee intra-articular needle placement can be obtained without guidance. If anatomical guidance (eg, palpation of anatomic landmarks) appears to be too difficult due to body habitus, distorted or complicated anatomy, or other factors, then fluoroscopic or ultrasound guidance may be considered.19
However, recent studies suggest that the use of imaging during injection significantly increases the needle placement accuracy rates. In the absence of imaging, up to 20% of injections are inaccurate.18
Equipment
• 25-gauge 1.5-in needle
• 22-gauge 2-in needle (an 18-gauge needle may be required for large-volume aspiration)
• 3-cc syringe for local anesthetic (optional)
• 10-cc syringe for aspiration
• 10-cc syringe for intra-articular steroid/anesthetic
Medications
• 1% lidocaine
• 0.25% or 0.5% bupivacaine (optional)
• Triamcinolone or methylprednisolone
Technique
Varying techniques have been described for intra-articular knee injections and aspiration:
• Medial or lateral parapatellar approach. Patient seated or supine position with knee flexed 45 to 90 degrees. This approach is also described as an anteromedial or anterolateral approach.20
• Medial or lateral suprapatellar approach. Patient in supine position, with knee in full extension.
• Medial or lateral retropatellar approach. Patient in supine position, with knee in full extension. This approach is also described as an medial or lateral midpatellar approach.20
The medial or lateral parapatellar approaches, with the patient seated and the knee flexed 90 degrees are commonly utilized by clinicians.
The advantage includes:
• Relatively easy access to the joint due to gravitational distraction forces on the knee that increases the tibio-femoral joint space.
The disadvantages include:
• The potential for infrapatellar fat pad injection that is very painful for the patient
• Inability to aspirate mild effusions in the flexed knee position
• Difficulty handling vasovagal responses for a seated patient
The medial or lateral suprapatellar approach, with the patient in supine position and the knee in full extension, are another approach commonly utilized by clinicians (Figure 51-3).

Figure 51-3. Positioning.
• Safer positioning for management of potential vasovagal responses during or after the injection
• The ability to aspirate joint effusions and confirm intra-articular needle placement
• The ability to avoid infra-patellar fat pad injections
• Accuracy remains high with this approach.
The disadvantage includes:
• A potentially narrower joint space to navigate
The medial or lateral retropatellar approaches have similar advantages and disadvantages as those described for the suprapatellar approaches.
Medial Suprapatellar Approach
We advocate the medial suprapatellar approach. In our opinion, this technique minimizes the potential risk of a painful injection that may occur due to inadvertent infrapatellar fat pad injection, allows confirmation of intra-articular placement if an effusion is present, and allows for easier management of vasovagal responses. In our experience, this approach is tolerated very well by the patient and is a very accurate approach in regards to intra-articular needle placement.21,22
Our Preferred Technique
• The patient is placed in a supine position with the knee in full extension (see Figure 51-3).
• The skin overlying the knee is marked, using key anatomical landmarks (eg, medial and superior poles of the patella and medial femoral condyle) (Figure 51-4).

Figure 51-4. Photo of anatomical landmarks on the right knee. The circle outlines the patella, infrapatellar tendon is outlined as well and a small horizontal line represents the superior pole of the patella.
• The injection site is prepared in a typical sterile fashion (Figure 51-5).

Figure 51-5. Site of needle entry marked with an X, and sterile preparation of the injection site.
• Up to 3-cc of 1% lidocaine is then infiltrated into the skin overlying the site of the injection to provide adequate skin analgesia using the 25-gauge 1.5-in needle.
• The injectate is drawn up into the 10-cc syringe which consists of 40 mg of either triamcinolone or methylprednisolone and 2 to 4 cc of 1% lidocaine +/–, an additional 2 cc of 0.25% bupivacaine.
• The 22-gauge 2-in needle with an empty 10-cc syringe attached (an 18-gauge needle may be required for large-volume aspiration) is then advanced at approximately a 45 degree from the Sagittal plane. The needle will be directed in a slightly lateral, inferior, and posterior direction to enter the capsule of the knee joint (Figure 51-6). The patella may be tilted slightly to open up the joint space (Figure 51-7).

Figure 51-6. Needle placement photo and line drawing of needle placement.

Figure 51-7. Image of Patella Tilt, preformed to slightly elevate the medial facet of the patella.
• Once the needle is suspected to have entered the joint capsule, the needle is then aspirated to confirm intra-articular placement (and for therapeutic reasons) and to ensure that the needle is not intravascular.
• Once proper placement has been achieved, the 10-cc syringe used for aspiration is removed and 10-cc syringe containing the injectate is attached.
• Then the injectate is instilled into the knee joint.
• At the conclusion of the procedure, the needle is clearly withdrawn and sterile dressings are used to apply pressure.
• The area is cleaned with an alcohol solution, dried, and a dressing is applied over the site of the injection.
INTRA-ARTICULAR KNEE INJECTION OF VISCOSUPPLEMENT
Preoperative Considerations
• Please refer to the section Intra-articular Knee Injection for Aspiration/Steroid Injection.
Fluoroscopic or Ultrasound Views
• Please refer to the section Intra-articular Knee Injection for Aspiration/Steroid Injection.
Equipment
• 25-gauge 1.5-in needle (optional)
• 22-gauge 2-in needle
• 3-cc syringe for local anesthetic (optional)
• 10-cc syringe for aspiration
• Syringe of viscosupplement
Medications
• 1% lidocaine
• Viscosupplement (one preloaded syringe of preferred viscosupplement)
Our Preferred Technique
• The patient is placed in a supine position with the knee in full extension.
• The skin overlying the knee is marked, using key anatomical landmarks (eg, medial and superior poles of the patella and medial femoral condyle) (see Figure 51-4).
• The injection site is prepared in a typical sterile fashion (see Figure 51-5).
• Up to 3 cc of 1% lidocaine is then infiltrated into the skin overlying the site of the injection to provide adequate skin analgesia using the 25-gauge 1.5-in needle.
• The 22-gauge 2-in needle with an empty 10-cc syringe attached (an 18-gauge needle may be required for large-volume aspiration) is then advanced at approximately a 45 degree from the sagittal plane. The needle will be directed in a slightly lateral, inferior, and posterior direction to enter the capsule of the knee joint (see Figure 51-6). The patella may be tilted slightly to open up the joint space (see Figure 51-7).
• Once the needle is suspected to have entered the joint capsule, the needle is then aspirated to confirm intra-articular placement (and for therapeutic reasons) and to ensure that the needle is not intravascular.
• Once proper placement has been achieved, the 10-cc syringe used for aspiration is removed and a preloaded syringe of preferred viscosupplement is attached.
• Then the viscosupplement is instilled into the knee joint.
• At the conclusion of the procedure, the needle is clearly withdrawn and sterile dressings are used to apply pressure.
• The area is cleansed with alcohol solution, dried, and a dressing is applied over the site of the injection.
Postprocedure Follow-Up
The patient should be instructed to contact the office if there are any concerns for potential complications. It is important to advise the patient that the antiinflammatory effect of steroid will not be apparent for 48 to 72 hours and maximal benefit may take up until 1 or 2 weeks postinjection. The primary concern postinjection is for infection (cellulitis or joint infection), therefore, the patient should monitor the injection site for erythema, warmth, increased swelling, or systemic features of an infection:
• Fever or chills
In addition, depending on the viscosupplement chosen, the patient will need to return to the office to repeat this injection an additional 2 to 4 times. Treatment with viscosupplement, with the exception of Synvisc-One, follows a protocol recommended by the manufacturer for a treatment series of 3 to 5 total injections.
Potential Complications
Because of the percutaneous approach, there are limited potential systemic complications from this treatment. The most commonly reported adverse events with VSN and steroid injections are transient and occur at the injection site. The potential complications include:
• Mild pain
• Swelling or effusion
• Warmth
• Redness
• Allergic reactions to the medications.
• Iatrogenic knee joint infections or local skin infections.
• Hemarthrosis of the knee joint
Product-specific instances of pseudosepsis were found in patients who received Synvisc injections.10,11,23 In rare cases, patients reported various systemic effects.10,24 The long-term effects of repeated steroid injections and VSN on the joint are conflicting. A number of studies have concluded that repeated injections of VSN are safe and have no known long-term complications.4,25 A more recent study found increased levels of a cartilage breakdown marker postprocedure, suggesting that long-term VSN use increases the rate of joint degradation.26,27
Similarly with steroids, there is some fear that repeated injections will lead to more rapid joint deterioration; however, there is little current evidence supporting or denying this claim.3,28 The potential, but rare, complications from steroid injections also include skin depigmentation and subcutaneous fat atrophy.29–33
CLINICAL PEARLS
• These injections are effective therapeutic tools for the management of knee OA.
• The duration of benefit is variable
• Steroid injections tend to produce substantial short-term relief of symptoms (eg, pain, swelling), whereas VS tend to produce longer duration relief (3-6 months) but with a slower onset of relief.
• These injections are well tolerated and have an excellent safety profile. If patient compliance for a series of injections may be a problem, then consider Synvisc-One.
• No specific VS has been proven to be superior to another, so clinicians can help their patients to make individualized choices. The variables include but are not limited to patient allergies (eg, egg allergies require avoiding those VS made from avian products) or the patient’s ability to return to the office weekly for repeated injections.
• Many needle approaches can be utilized, all with relatively good accuracy, but our preferred approach is the medial supra-patellar approach. The patient remains relaxed in the supine position, with the knee extended and a 22-gauge 2-in needle is guided percutaneously under the supero-medial aspect of the patella into the joint capsule.
• These procedures can be repeated to manage recurrent symptoms (eg, knee pain, joint effusion) and maintain quality of life.
• Typically, the use of steroids is best in patients with concurrent acute synovitis and arthritis versus viscosupplementation which is best utilized in patients with knee osteoarthritis without synovitis.





Full access? Get Clinical Tree


