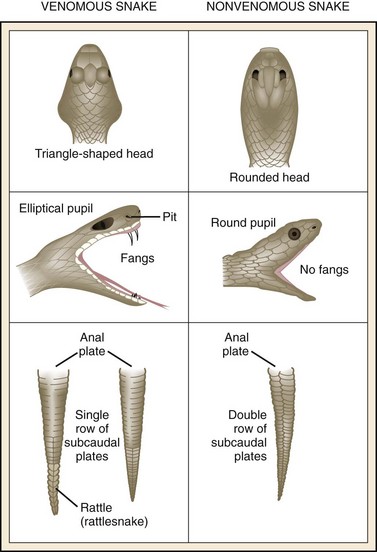
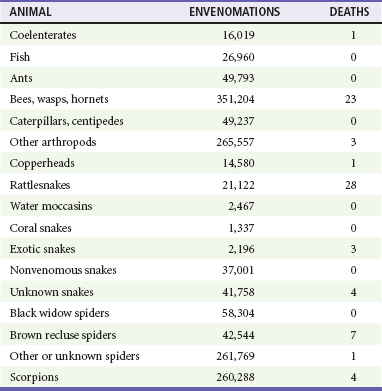
Chapter 62 Venomous animals account for considerable morbidity and mortality worldwide. Snakes alone are estimated to inflict 2.5 million venomous bites annually, with approximately 125,000 deaths. The actual numbers may be much larger. Southeast Asia, India, Brazil, and areas of Africa lead the world in snakebite mortality.1 It is impossible to estimate the worldwide morbidity and mortality resulting from other venomous animals such as bees, wasps, ants, and spiders. The American Association of Poison Control Centers began collecting data in 1983 on deaths caused by venomous animals. Their 25-year experience shows a significant number of exposures by bite or sting but relatively few deaths (Table 62-1).2 Although these data include most of the United States, there is no requirement that hospitals, emergency departments, coroners, or public health agencies report deaths or exposures to regional drug and poison information centers. This decline in deaths may be caused by an actual decrease in mortality or may be a result of inadequate reporting. Meaningful morbidity data, such as the number of amputations, hospitalizations, and disabilities, do not exist. The number of exposures and deaths from exotic snakes seems to be increasing, possibly because of interest in collecting so-called “hot” or venomous varieties such as cobras, mambas, and vipers. The morbidity from marine animal injuries is increasing in proportion to the number of people exposed to the ocean and the number of private collectors, but the mortality has not increased dramatically. An increase in outdoor recreational activities, such as camping, scuba diving, and wilderness trekking, puts more people in proximity to venomous animals and increases the risk of envenomation. Most exposures occur from April to October, when animals are most active and potential victims are outdoors and involved in activities that might increase their risk for envenomation. Of course, many spider bites and exotic animal envenomations that occur indoors can take place at any time. Most deaths seem to occur in very young, elderly, or inappropriately treated patients. Table 62-1 Venomous Animal Injuries and Deaths, 1983-2009 Data compiled from Watson WA, Litovitz TL, et al: American Association of Poison Control Centers data. Am J Emerg Med 2:1984–2005; Lai et al: Clin Toxicol 44, 2006; and Bronstein et al: Clin Toxicol 45, 2007, Clin Toxicol 46, 2008, Clin Toxicol 47, 2009, Clin Toxicol 48, 2010. Animals that have developed specific venom glands and venom delivery systems can be found in every class, including birds.3 The toxin and toxic apparatus vary from class to class. For example, the rattlesnake has modified salivary glands and maxillary teeth and uses this system primarily to obtain food. The bee has a modified ovipositor that is used mainly for defense. Poisonous and venomous animals are not the same and should be differentiated. Animals can be considered poisonous because of various toxins distributed in their tissues. For example, certain shellfish, toads, and barracuda have been known to cause death after ingestion. However, only animals with specific glands for producing venom connected to an apparatus for delivering that venom to another animal can be considered venomous. The incidence of reported venomous snakebites in the United States is greatest in the South. States having the highest death rates are North Carolina, Arkansas, Texas, and Georgia. Of all snakebites, 97% occur on the extremities, with two thirds on the upper extremities and one third on the lower extremities. This reversal of historical distribution may reflect bites being provoked rather than accidental. Bites that occur accidentally are considered “legitimate,” whereas bites that occur during attempts to handle or disturb a snake are considered “illegitimate.” Men are bitten nine times more frequently than women.4 Pit vipers, the most prevalent venomous snakes in the United States, are native to every state except Maine, Alaska, and Hawaii. They are classified into three main groups: true rattlesnakes (genus Crotalus), copperheads and water moccasins (genus Agkistrodon), and pygmy or Massasauga rattlesnakes (genus Sistrurus). Pit vipers account for 98% of all venomous snakebites in the United States.5 There are two key principles for identifying venomous snakes: Only experts should handle live snakes, and even dead snakes can envenomate careless handlers.6 It is not difficult to differentiate between pit vipers and harmless snakes found in the United States (Fig. 62-1). Pit vipers, as their name implies, have a characteristic pit midway between the eye and the nostril on both sides of the head. This pit is a heat-sensitive organ that enables the snake to locate warm-blooded prey. Pit vipers may be identified through other methods, but this characteristic is 100% consistent. The triangular shape of the head, the presence of an elliptical pupil, the tail structure, and the presence of fangs are useful characteristics but are inconsistent. The arrangement of subcaudal plates may be used for Crotalinae if the head has been damaged or is unavailable. An individual specimen may not fit the classic description, depending on the age of the snake, the time of the year, and the condition of the tail and mouthparts. Neither color nor skin pattern is a reliable method of identifying pit vipers (Fig. 62-2). Only two venomous lizards are found in the world, both in the southwestern United States and Mexico. They are the Gila monster (Heloderma suspectum) and the Mexican beaded lizard (Heloderma horridum). Fortunately, both these lizards are nonaggressive and rarely encountered. Bites usually result from handling the animals in captivity.7 The Gila monster and the Mexican beaded lizard are easily identifiable. Both have thick bodies, beaded scales, and either white and black or pink and black coloration. Elapidae and Hydrophiidae venoms have predominantly systemic effects, whereas Colubridae, Viperidae, and Crotalinae venoms have mainly local effects. There are many exceptions to this general division. For example, the venom of the Mojave rattlesnake (Crotalus scutulatus) may show minimal local effects and significant systemic effects, whereas the venom of the cobra (Naja naja) may cause extensive local tissue destruction.8 The mechanism for delivering venom is fairly standard among snakes. It consists of two venom glands, hollow or grooved fangs, and ducts connecting the glands to the fangs. The glands, which evolved from salivary glands, are located on each side of the head above the maxillae and behind the eyes. Each gland has an individual muscle and a separate nerve supply that allow the snake to vary the amount of venom injected. The venom duct leads from the anterior portion of the gland along the maxilla to the fangs. Pit vipers have fangs that are large anterior maxillary teeth. These teeth are hollow and rotate outward from a resting position to a striking position. The coral snake has fixed, hollow maxillary teeth that are much smaller than those of pit vipers. The fangs in most snakes are shed and replaced regularly, and it is not unusual to see a snake with double fangs on one or both sides of its mouth.9 The most consistent symptom associated with pit viper bites is immediate burning pain in the area of the bite, whereas pain may be minimal with bites of Elapidae and other exotic snakes. With pit vipers, the severity of pain is probably related to the amount of venom injected or the degree of swelling. Edema surrounding the bite that gradually spreads proximally is a common finding. This edema is usually subcutaneous, begins early, and may involve the entire extremity. Compartment syndrome has been described; however, it is unusual even with severe edema. It has been reported more frequently in models involving intracompartmental venom injection.10–12 Most fangs do not penetrate into the fascial compartments, although muscle destruction may result from direct toxicity. Mortality is less frequent with distal bites to the toe and finger and is greatly increased with intravenous bites. An intravenous bite from any venomous snake is likely to be fatal. Petechiae, ecchymosis, and serous or hemorrhagic bullae are other local signs. Necrosis of skin and subcutaneous tissue is noted later and may result from inadequate doses of antivenin. Many systemic symptoms, such as weakness, nausea, fever, vomiting, sweating, numbness and tingling around the mouth, metallic taste in the mouth, muscle fasciculations, and hypotension, often occur after pit viper envenomation. Death from pit viper bites is associated with disruption of the coagulation mechanism and increased capillary membrane permeability. Ultimately, these two processes lead to massive pulmonary edema, shock, and death. Heart and kidney damage occur secondary to these mechanisms. Specific toxins in certain species may act directly on specific organs, such as the heart or skeletal muscle. An allergic type of reaction may add to this process through release of histamine and bradykinin.13 Signs and symptoms can vary considerably with bites of coral snakes, Mojave rattlesnakes, and many exotic snakes, especially cobras and Australian elapids. Little pain and swelling may occur. Many of these species’ venoms contain compounds that block neuromuscular transmission at acetylcholine receptor sites and have direct inhibitory effects on cardiac and skeletal muscle. Ptosis is common and often the first outward sign of envenomation. Other signs and symptoms include vertigo, paresthesias, fasciculations, slurred speech, drowsiness, dysphagia, restlessness, increased salivation, nausea, and proximal muscle weakness. The usual cause of death is respiratory failure.14 All snakebites are considered an emergency, and any victim should be medically evaluated. The initial 6- to 8-hour period after a snakebite is critical. During this time, medical therapy can help prevent the morbidity associated with severe envenomation. Effective out-of-hospital care can be important.16 Second, spread of the venom should be slowed if possible; several methods are known. The patient’s excitement and physical activity, movement of the bitten area, alcohol consumption, and greater depth of the bite may increase the spread of venom. Except for the last factor, these issues can be addressed by calming the victim, immobilizing the bitten area with a sling or splint, and not giving anything by mouth. A method of first aid for venomous snakebites that was developed in Australia—the immobilization and compression technique (also called the Commonwealth Serum Laboratory technique)—slows uptake of Elapidae venom and mock venom in humans. The bitten extremity is either wrapped in an elastic bandage or placed in an air splint. In another technique from Australia called the Monash method, a thick pad and bandage are placed over the bite wound and extremity. Both these techniques have similar postulated mechanisms of action: The lymphatic vessels and superficial veins are collapsed, and the proximal spread of venom is slowed.17 Although this method is successful as first-aid therapy for Elapidae bites, its use for pit vipers has not been demonstrated. If less than 30 minutes has elapsed since the bite, a constricting band applied tightly enough to impede superficial venous and lymph flow, but not arterial blood flow, may be used. The band is applied loosely enough to admit a finger between the band and the skin after application. It is used with caution to prevent the development of a tourniquet effect under swollen tissue, which may cause more destruction than the snakebite.18 Incision of bite wounds has no proven efficacy and poses potential danger to underlying structures and therefore is not recommended. The use of ice is not helpful in slowing the spread of venom, but an ice bag wrapped in a towel and applied to the bite area helps relieve pain. Ice water immersion and packing of the extremity in ice are dangerous and only contribute to tissue destruction. The use of suction devices has not been shown to be beneficial.19 Patient History.: Specific historical information includes time elapsed since the bite, the number of bites, whether first aid was administered and what type, location of the bite, and symptoms (e.g., pain, numbness, nausea, tingling around the mouth, metallic taste in the mouth, muscle cramps, dyspnea, and dizziness). A brief medical history includes the last tetanus immunization, medications, and cardiovascular, hematologic, renal, and respiratory problems. An allergy history with emphasis on symptoms after exposure to horse or sheep products, previous injection of horse or sheep serum, and a history of asthma, hay fever, urticaria, or allergy to wool, papain, chymopapain, papaya. or pineapple should be obtained if antivenin treatment is being considered. Patient Examination.: The bite area is examined for signs of fang marks or scratches and local envenomation (e.g., edema, petechiae, ecchymosis, and bullae). The area distal to the bite is checked for pulses. A general physical examination is performed, with emphasis on the cardiorespiratory system and the neurologic examination, especially if a Mojave rattlesnake, coral snake, or exotic snake is suspected. If the bite involves an extremity, the circumference of the extremity at the site of the bite and approximately 5 inches proximal to the bite should be measured and recorded. These data aid in objectively estimating both spread of the venom and the effect of antivenin (Fig. 62-3). Initial Medical Care.: If the bite occurred less than 30 minutes before arrival in the emergency department, first-aid measures can be instituted, including a constricting band until antivenin, can be obtained. Snakebite victims with clinical evidence of envenomation should have an intravenous line with normal saline placed in an unaffected extremity. An electrocardiogram, complete blood count, urinalysis, protime, and levels of fibrinogen, fibrin split products, electrolytes, blood urea nitrogen, and creatinine are recommended; blood should be typed and crossmatched for 4 units of packed red blood cells. The patient’s vital signs are monitored closely. Snakebite victims may be hypotensive because of third-space losses and hemorrhage. In an edematous extremity, the distal pulse may have to be examined with a Doppler instrument. If a compartment syndrome is suspected, insert a pressure monitor and obtain surgical consultation. If signs and symptoms of compartment syndrome are present, pressure greater than 30 mm Hg may necessitate fasciotomy, although there is evidence that administration of antivenin may lower compartment pressures.12,13 Once stabilization is initiated, the severity of the bite must be determined and a decision made regarding whether to administer antivenin. The more distal the bite on the extremity, the less toxicity associated with the bite.20 Intravenous bites may be rapidly fatal. Bites occurring on the trunk, neck, and face have increased risk because of rapid transit of the venom. Antivenin.: The emergency physician must determine the type of antivenin to administer, how much, and over what period. If the bite is from a pit viper, the problem is not too difficult. Bites from copperheads usually cause a moderate amount of edema but generally do not require antivenin, although it may be indicated in selected cases.21 Envenomation may be classified according to severity into five grades, from grade 0 (no sign of envenomation) to grade IV (very severe envenomation). The amount of antivenin to be given is correlated with the grade of envenomation: • Grade 0 (minimal). There is no evidence of envenomation, but snakebite is suspected. A fang wound may be present. Pain is minimal, with less than 1 inch of surrounding edema and erythema. No systemic manifestations are present during the first 12 hours after the bite. No laboratory changes occur. • Grade I (minimal). There is minimal envenomation, and snakebite is suspected. A fang wound is usually present. Pain is moderate or throbbing and localized to the fang wound, surrounded by 1 to 5 inches of edema and erythema. No evidence of systemic involvement is present after 12 hours of observation. No laboratory changes occur. • Grade II (moderate). There is moderate envenomation, more severe and widely distributed pain, edema spreading toward the trunk, and petechiae and ecchymoses limited to the area of edema. Nausea, vomiting, and a mild elevation in temperature are usually present. • Grade III (severe). The envenomation is severe. The case may initially resemble a grade I or II envenomation, but the course is rapidly progressive. Within 12 hours, edema spreads up the extremity and may involve part of the trunk. Petechiae and ecchymoses may be generalized. Systemic manifestations may include tachycardia and hypotension. Laboratory abnormalities may include an elevated white blood cell count, creatine phosphokinase, prothrombin time, and partial thromboplastin time, as well as elevated fibrin degradation products and D-dimer. Decreased platelets and fibrinogen are common. Hematuria, myoglobinuria, increased bleeding time, and renal or hepatic abnormalities may also occur. • Grade IV (very severe). The envenomation is very severe and is seen most frequently after the bite of a large rattlesnake. It is characterized by sudden pain, rapidly progressive swelling that may reach and involve the trunk within a few hours, ecchymoses, bleb formation, and necrosis. Systemic manifestations, often commencing within 15 minutes of the bite, usually include weakness, nausea, vomiting, vertigo, and numbness or tingling of the lips or face. Muscle fasciculations, painful muscular cramping, pallor, sweating, cold and clammy skin, rapid and weak pulse, incontinence, convulsions, and coma may also be observed. An intravenous bite may result in cardiopulmonary arrest soon after the bite. Dart and colleagues have advocated slightly different grading systems and higher doses of antivenin: Grades 0 and I correspond to minimal envenomation, grade II represents moderate envenomation, and grades III and IV correspond to severe envenomation.22,23 Either system can be used interchangeably. Administration of Antivenin.: Any victim of a venomous snakebite with moderate or severe envenomation is a candidate for antivenin. The choice of antivenin depends on the species of snake, and the antivenin may be horse serum- or sheep-derived Fab fragments. Wyeth Laboratories, producer of the polyvalent horse serum–derived antivenin for Western Hemisphere pit vipers, no longer manufactures that antivenin. Many zoos and hospitals still maintain vials of this antivenin until it can be replaced with the ovine-derived Fab antivenin (FabAV). This antivenin is derived from four species of U.S. pit vipers and has not been clinically studied with regard to bites from Mexican, Central American, or South American pit vipers.23,24 There is a reported case of a patient bitten by a South American rattlesnake who was successfully treated with FabAV.25 Most antivenin for exotic snakes and the eastern coral snake is derived from horse serum. A recent polyvalent Fab(2) antivenin derived form horse serum and produced in Mexico has been shown to be effective against both North and South American crotalid species.26 Skin testing was commonly performed before administration of horse serum–derived antivenin, but it is not medically indicated because of the inaccuracy of the test. Moreover, testing with normal horse serum may precipitate an allergic reaction, and even a positive test result may not preclude treatment if a patient has sustained severe envenomation. The incidence of allergic reactions with Fab antivenins has been much less than previously seen with whole IgG. The incidence of allergic reactions was 17% for early reactions and 12% for late reactions in postmarketing analysis. This was thought to be a result of incomplete purification of one lot contaminated by Fc fragments. Most of these reactions were minor and did not require stopping the infusion of the antivenin. The true incidence is unknown.27–30 Dosage and Precautions.: Current treatment of pit viper envenomation in the United States is to use a FabAV polyvalent antivenin rather than the horse serum product.31 This is designed to limit the allergic reactions associated with horse serum antivenin by use of antigen-binding fragments (Fabs) of sheep (ovine) immunized against four species of venomous snake found in the United States. CroFab has been shown to be as effective as the Wyeth antivenin, with fewer allergic reactions. Because of more rapid clearance of smaller Fab fragments by the kidney, however, a repeat-dose regimen must be used to prevent the recurrence of coagulopathy. The duration of action of the venom may be longer than the therapeutic effect of the antivenin. Initial studies have shown promise for a new affinity-purified, mixed monospecific ovine Fab antivenin that has been tested with favorable results in humans after minimal to moderate crotalid envenomation.23 Its efficacy in pit vipers from South America or Asia has not been proved. Purification of antivenin by separation of active fractions may lead to safer administration of horse serum–derived antivenin. An algorithm has been developed that can aid in decision-making after a crotalid bite (Table 62-2 and Fig. 62-4).31 In the next decade, snakebite management will probably change radically throughout the world. Phytotherapy (botanical therapy) and other nonantivenin drug therapies for snakebite have shown promise in experimental animal studies, and some centers have successfully treated snakebite with medical support only. Hyperbaric oxygen therapy has also been used as an adjunct to antivenin in the treatment of venomous snakebite; however, there is insufficient evidence to recommend its use.32 Table 62-2 Antivenin Dosage for Pit Viper Envenomation* *Dosage based on initial findings and clinical response to antivenin. (See also Fig. 62-4.) †If this dose elicits a clinical response, it is recommended that an additional two vials be given at 6, 12, and 18 hours. The patient’s coagulation studies should be followed to determine additional amounts.
Venomous Animal Injuries
Perspective
Venom Delivery
Venomous Reptiles
Epidemiology
Classification and Characteristics
Identification
Other Reptiles
Principles of Disease
Venom Delivery
Clinical Features
Pit Vipers
Coral Snakes
Management
Emergency Department Care
FabAV†
FabAV
ENVENOMATION
INITIAL DOSE TOTAL
MAINTENANCE DOSE
Moderate
4-6 vials
2 vials
Severe
8-12 vials
2-4 vials
Very severe
12-18 vials
4-10 vials

Full access? Get Clinical Tree