Increased afterload
Decreased heart rate (baroreflex)
Increased coronary and cerebral blood flow
Cardiac conduction system
Increased heart rate
Increased conduction
Increased automaticity
Vascular smooth muscle of skeletal blood vessels
Vasodilation
Vasopressor Medications
As blood pressure decreases, neural and hormonal autoregulatory mechanisms may become compromised, causing tissue bed perfusion to become solely reliant on the maintenance of adequate blood pressure for a sufficient supply of oxygenated blood. Consequently, medications with vasopressor properties are often used to restore blood pressure and perfusion in states of hypotension and shock. Data from a large multicenter, descriptive study in the United States revealed that almost one quarter of adults admitted to a critical care unit require at least one vasoactive infusion, and more than a third of patients in cardiovascular surgery units require vasopressor support.6
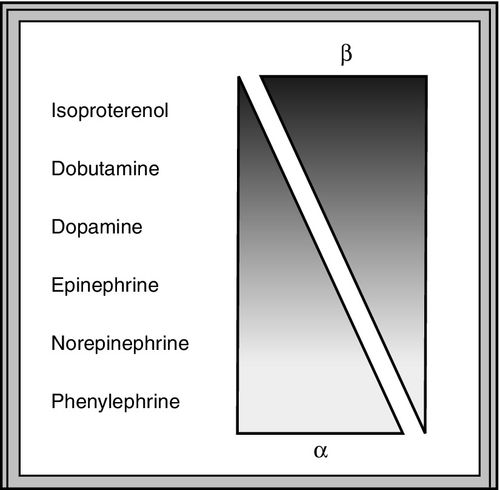
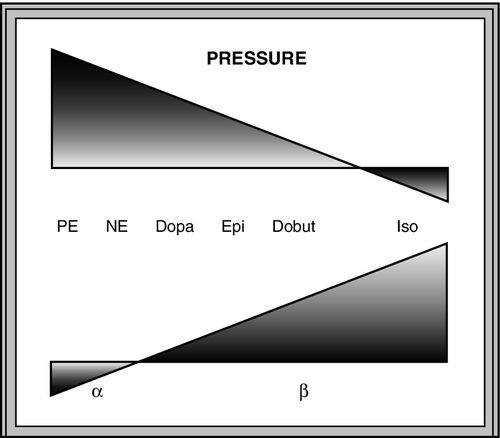
Most vasoactive agents are catecholamines, or adrenergic agonists. They mimic the effects of the sympathetic nervous system by stimulating alpha-, beta-, and other vascular receptors. They are administered intravenously, have a half-life of 1 to 2 minutes and reach their peak effect within 10 minutes.1,7 As a result, they can be quickly titrated to manage hemodynamic instability.
The majority of catecholamines increase blood pressure by stimulating alpha-1 adrenergic receptors in vascular smooth muscle. It is important to evaluate clinical signs of adequate tissue perfusion while administering these medications, particularly at higher doses, as the resultant vasoconstriction may adversely reduce perfusion to vulnerable cutaneous, mesenteric, and renal tissue beds. See the Clinical Indications section for a discussion on the clinical signs of perfusion. Medications with strong vasoconstrictive properties should be used cautiously in patients with compromised myocardial function, as the increase in afterload may impede cardiac output and increase myocardial oxygen demand. Use of vasoactive agents in the setting of hypovolemia does not markedly improve cardiac output and may worsen microcirculatory flow because of vasoconstriction.
The names, properties, and usual dose ranges of commonly used vasopressors are listed in Table 9-2. Also, see Box 9-1 for a discussion of the differences and similarities of three specific vasopressors.
Table 9-2
Vasopressor Medications
D, Dopaminergic receptor; mcg/kg/min, micrograms per kilogram per minute; mcg/min, micrograms per minute.
Dopamine
Dopamine (Intropin) is an endogenous central nervous system neurotransmitter that is a direct precursor of norepinephrine and epinephrine. Once metabolized, it stimulates the sympathetic nervous system. The effects of exogenously administered dopamine are dose dependent. Dopamine primarily has dopaminergic properties at low doses of 2 micrograms per kilogram per minute (mcg/kg/min), and beta-1 properties at doses between 2 and 10 micrograms per kilogram per minute.8 See the Positive Inotropes section for a discussion on the inotropic, vascular, and kidney effects of dopamine. At doses over 10 mcg/kg/min, it primarily stimulates alpha-1 receptors and causes vasoconstriction, which may negate the positive inotropic effects.8 It may also cause a marked increase in heart rate, which may increase myocardial oxygen demand and reduce cardiac output by shortening diastolic filling time. Dopamine may be used to manage hypotension of unknown origin and is titrated to achieve a desirable blood pressure. Appropriate circulating volume must be ensured prior to starting dopamine because it has a high propensity for causing tachycardia in hypovolemic patients. Dopamine may be considered for the management of hypoperfusion in the setting of septic shock when the patient is exhibiting relative or absolute bradycardia and is not likely to develop a tachydysrhythmia.9 Soft tissue ischemia and necrosis will result from extravasation of dopamine or other vasopressors. Consequently, it is preferable to infuse these medications in a central venous catheter.7 If infiltration does occur, phentolamine is the treatment of choice and is discussed further in the section on Alpha Blockers.
Phenylephrine
Phenylephrine (Neo-Synephrine) is a synthetic catecholamine that is a pure alpha-1 agonist that causes vasoconstriction. Phenylephrine has no beta-adrenergic agonist activity, has no direct effect on the myocardium, and does not increase heart rate. Phenylephrine may be used to restore blood pressure for neurogenic shock and hypotension caused by medications or vagal stimulation. In light of the lack of myocardial effect, it may be used for septic shock when norepinephrine is associated with tachydysrhythmia or if cardiac output is known to be high with a persistently low blood pressure.9 A bolus dose of 0.1 to 0.5 micrograms may be given every 10 to 15 minutes for precipitous decreases in blood pressure.4 Side effects of phenylephrine include increased afterload, reflex bradycardia, and peripheral ischemia.
Norepinephrine
Norepinephrine (Levophed), an endogenous neurotransmitter, is a potent alpha-1 agonist with mild beta-1 properties and no beta-2 activity. Therefore, it is a relatively weak positive inotrope and a potent vasoconstrictor, as its alpha-1 properties are unopposed. Norepinephrine is indicated for hypotension caused by vasodilatory shock states. In particular, it is recommended as a first-line agent in the setting of septic shock and should be titrated to increase the mean arterial blood pressure to 65 millimeters of mercury (mm Hg).9,10 Side effects of norepinephrine include tachycardia, dysrhythmias, myocardial ischemia, and, at higher doses, decreased organ and peripheral perfusion. Not all forms of shock are amenable to treatment with norepinephrine, which should not be started late in the course of cardiogenic shock because it increases afterload and decreases cardiac output.
Epinephrine
Epinephrine, also referred to as adrenaline in many countries, is an endogenous catecholamine that has strong beta-1 and beta-2 adrenergic properties that may cause a marked increase in cardiac output and heart rate, as well as bronchodilation. Although it increases blood flow to skeletal muscle beds, its potent alpha-1 agonist and vasoconstriction properties moderate the vasodilation from beta-2 receptor stimulation. Epinephrine also stimulates cardiac muscle cells to release a local vasodilator that increases coronary blood flow. A bolus dose of 1 milligram (mg) of epinephrine is indicated for cardiac arrest because of its ability to increase perfusion pressure to the coronary and cerebral blood vessels.11 It is sometimes used for vasodilatory hypotension and cardiogenic shock when other agents do not produce the desired outcomes. Epinephrine may also be used as a second line of therapy for bradycardia and heart block associated with hypotension. Its bronchodilatory effects make it useful for anaphylaxis and severe asthma that is unresponsive to other therapies. When patients with septic shock remain hypotensive, epinephrine may be added to or substituted for norepinephrine.9 Because of its potent effects, epinephrine should be started at low doses and carefully titrated to achieve a desirable response. Side effects of epinephrine include tachycardia and increased myocardial oxygen consumption. Therefore, it is generally regarded as a second-line therapy and reserved for treatment of profound shock because of its potential for inducing myocardial ischemia and tachydysrhythmia. Regional perfusion deficits may be caused by its strong alpha-1 effects. Because it is a stress hormone, epinephrine may stimulate gluconeogenesis and insulin resistance, which result in hyperglycemia.
Vasopressin
Vasopressin, a synthetic antidiuretic hormone, is a unique vasopressor that does not stimulate adrenergic receptors. Instead, it stimulates the V1 and V2 receptors, causing potent vasoconstriction and increased blood volume, respectively. Other mechanisms that promote vasoconstriction are thought to be related to vasopressin’s ability to reduce nitric oxide production and to attenuate adrenergic receptor downregulation, which results in an enhancement of the body’s response to catecholamines.4,5 An IV infusion of vasopressin is indicated for treating refractory vasodilatory shock. Vasopressin may be particularly helpful in hypoxic and acidotic states when adrenergic agonists are less effective. An infusion of 0.03 units per minute (units/min) is recommended as a second-line treatment for septic shock to either increase the mean arterial pressure or to decrease the dose and potential adverse effects of norepinephrine.5,9 The infusion dose is constant. It is not titrated, as it is administered as a replacement for a relative deficiency of endogenous vasopressin hormone. Vasopressin may also be beneficial for those who experience vasoplegic shock after cardiopulmonary bypass surgery.4,12 A single IV dose of 40 units may be given for asystole, pulseless electrical activity, shock, refractory ventricular fibrillation, and pulseless ventricular tachycardia.11
Vasodilator Medications
Direct-acting vasodilators stimulate the formation of nitric oxide by the vascular endothelium, which, in turn, activates cyclic guanosine monophosphate. This substance facilitates smooth muscle relaxation by preventing cross-bridging of myosin with actin. Vasodilators are typically used to manage severe increases in blood pressure and may also be used in conditions in which excessive afterload impedes cardiac output. The venous system, which is able to distend, can accommodate large volumes of blood under low pressure. Medications that dilate veins further increase venous capacitance, and reduce venous return to the heart, thus reducing cardiac preload. Patients with acute decompensated heart failure with pulmonary congestion and dyspnea at rest may benefit from a vasodilator as long as their blood pressure is adequate.13,14 See Table 9-3 for commonly used vasodilators with their mechanisms of action, dose ranges, and usual titration doses.
Table 9-3
Vasodilating Medications
mcg/kg/min, Micrograms per kilogram per minute; mcg/min, micrograms per minute; mg, milligrams; mg/hr, milligrams per hour.
Nitroprusside
Nitroprusside (Nipride), a potent and rapid-acting direct arterial and venous vasodilator, is used to manage severe hypertension. It may also be used to reduce afterload in patients with acute decompensated heart failure, particularly when they are hypertensive or have mitral valve regurgitation.14 The onset of its action is almost immediate, and the effects dissipate moments after it is discontinued. Nitroprusside is sensitive to light and must be protected with an opaque covering to prevent breakdown. It should be carefully titrated to achieve the desired blood pressure, which occurs with decreased SVR. Because of its short half-life and powerful effects, care should be taken to avoid any deleterious swings in blood pressure.
The side effects of nitroprusside include hypotension, decreased platelet aggregation, flushing, diaphoresis, and rash. Hypoxemia with ventilation–perfusion mismatch may also occur when pulmonary arterioles in nonventilated areas dilate. Nitroprusside has been associated with increases in intracranial pressure caused by alterations in cerebral autoregulation.15 Cyanide and thiocyanate, which are metabolites of nitroprusside metabolism, may cause toxic effects after exposure to high doses for prolonged periods. Cyanide causes metabolic acidosis by interfering with aerobic metabolism. The body has a limited supply of rhodanase, the enzyme needed to convert cyanide to thiocyanate. Originally, it was thought that if the amount of administered nitroprusside exceeded this limit, toxic levels of cyanide would accumulate and result in lactic acidosis. This premise led the U.S. Food and Drug Administration (FDA) to issue its strongest level of warning—a black box warning—to avoid nitroprusside doses greater than 2 mcg/kg/min. More recently, new data have suggested that additional enzymes and other chemical pathways for nitroprusside metabolism exist.16 Accordingly, higher doses of nitroprusside may be safe but warrant vigilant monitoring. Signs of cyanide toxicity include mental confusion, tinnitus, blurred vision, nausea, weakness, hyperreflexia, metabolic acidosis, and death. The maximum dose of 10 microgram per kilogram per minute should not be infused for more than 10 minutes.8 Nitroprusside infusions lasting more than 9 days should be avoided to prevent the accumulation of thiocyanate. Although thiocyanate is much less toxic than cyanide, prolonged exposure may cause neurologic derangements manifesting as confusion, hallucinations, seizures, and coma.16 Individuals with kidney insufficiency may suffer these toxic effects in as little as 3 days. Consequently, other antihypertensives should be considered when adequate blood pressure control is not achieved within this timeframe or as high doses are approached.
Nitroglycerin
Nitroglycerin (Tridil) causes vasodilation by generating nitric oxide in vascular smooth muscle. It is considered the drug of choice for angina and acute coronary syndrome because it dilates the coronary arteries and helps improve collateral blood flow to the ischemic areas of the myocardium. Nitroglycerin may be administered as a sublingual tablet or spray, transdermally, or intravenously. When administered intravenously at lower doses, it dilates the veins and reduces ventricular preload by reducing venous return to the heart. The reduction of intracardiac volume reduces ventricular wall stress and myocardial oxygen consumption. Therefore, nitroglycerin is also recommended for normotensive patients in acute heart failure when they are unresponsive to the usual therapies.14 At doses over 150 mcg/min, nitroglycerin decreases blood pressure and afterload by dilating the peripheral arteries.8 The side effects of nitroglycerin include hypotension, especially if the patient is volume depleted. Syncope and orthostatic hypotension may occur in patients sensitive to the medication. It is important to avoid using nitroglycerin in patients with right ventricular failure, as the right ventricle is reliant on sufficient venous return to maintain adequate cardiac output. Headache is another common side effect, and tolerance, which may necessitate escalation of doses to achieve the same clinical effect, may occur with prolonged use. Although the exact mechanism for this phenomenon is not completely understood, it is believed that nitric oxide production is reduced, whereas clearance is increased.17 Other proposed mechanisms include an increased sensitivity to vasoconstrictors and activation of the renin–angiotensin–aldosterone system, which oppose the effects of the remaining nitric oxide that is produced.17
Interactions with other medications are a concern. Patients who have taken a 5’phophosdiasterase inhibitor within the last 24 to 48 hours should not be given nitroglycerin because the combination may cause severe hypotension.8
The onset of action is 1 to 2 minutes, so the patient’s blood pressure should be closely monitored while initiating and titrating nitroglycerin. Nitroglycerin is titrated to achieve the desired clinical effects, which typically include elimination of anginal pain, reduction in pulmonary congestion, or decrease in blood pressure. Decrease of the systolic blood pressure below 90 mm Hg should be avoided to prevent a reduction in myocardial perfusion. Hypertensive individuals should not have a decrease of more than 25% in their blood pressure over several minutes to 1 hour.8
Hydralazine
Hydralazine (Apresoline) is an antihypertensive that causes arterial vasodilation by altering the movement of calcium within vascular smooth muscle. The peripheral vasodilation decreases peripheral vascular resistance with a resultant rise in stroke volume. Hydralazine has minimal effect on the veins and does not alter preload. Its propensity for inducing reflex tachycardia limits its usefulness, but this effect may be ameliorated by adding a beta-blocker. A slow IV injection of 10 to 20 mg may be administered for hypertensive crisis or for severe hypertension associated with preeclampsia or eclampsia.8,18 Subsequent doses should be administered cautiously after 15 minutes when the maximal blood pressure decrease can be determined. Side effects of hydralazine include headache, palpitations, flushing, and exacerbation of angina.
Nicardipine
Nicardipine (Cardene) is a dihydropyridine calcium channel blocker that causes arterial vasodilation and reduces systemic vascular resistance by blocking the influx of calcium in vascular smooth muscle. It is used for the short-term management of hypertension and is particularly useful in patients who have experienced an ischemic stroke.15,19 A systematic review comparing nicardipine and labetalol in the management of hypertensive crisis showed that while both agents had similar efficacy and safety profiles, nicardipine provided more consistent effects and required fewer dose changes.20 Nicardipine is contraindicated in those with advanced aortic stenosis. Its side effects include hypotension, tachydysrhythmia, headache, flushing, and dizziness.
Nesiritide
Nesiritide (Natrecor) is a recombinant form of human brain natriuretic peptide. When the heart becomes volume overloaded, the overstretched ventricular myocardium secretes the endogenous form of this hormone, which causes arterial and venous vasodilation. Accordingly, nesiritide is administered to patients with heart failure to alleviate pulmonary congestion and dyspnea by decreasing systemic afterload and venous return and by exerting a mild natriuretic effect. Natriuresis is a diuresis of urine with higher levels of sodium. An infusion of nesiritide for 24 to 48 hours is indicated in the management of dyspnea associated with acute decompensated heart failure, where it has been shown to decrease pulmonary artery occlusion pressure (PAOP), increase cardiac output, and improve diastolic function.21
If an endogenous brain natriuretic peptide level is needed for diagnostic purposes, it should be measured prior to starting a nesiritide infusion, as it cannot be reliably ascertained once the medication has been administered. Because the effects of nesiritide are not evident for several hours, dose changes are usually prescribed and performed no more frequently than every 3 hours. Nesiritide may cause hypotension, which usually occurs in the first hour and may last several hours. The initial bolus dose may be omitted to avoid hypotension in vulnerable individuals. If hypotension does occur, the infusion should be immediately stopped and a fluid bolus administered. Patients receiving nesiritide should be monitored for hypersensitivity reactions and anaphylaxis.8 Other adverse effects include bradycardia, atrial fibrillation, and other tachydysrhythmia.
The Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure (ASCEND-HF), a large, randomized, double-blind clinical trial, demonstrated that although nesiritide is relatively safe and confers a small, yet nonsignificant (p = 0.007), benefit on subjective reports of dyspnea, it did not significantly reduce the composite endpoint of heart failure re-admission or 30-day mortality (p = 0.31).22 Additionally, the use of nesiritide did not reduce the risk of kidney dysfunction. The study investigators recommended that nesiritide not be used in all patients with acute heart failure symptoms. Instead, it might be useful for selected individuals with volume overload, in whom a clinical benefit is observed.23 Patients who have had their native ventricles removed for implantation of a total artificial heart and are not able to produce endogenous brain natriuretic peptide, may benefit from nesiritide in situations where resistance to diuretics has developed.14
Positive Inotropes
Positive inotropic agents are administered to increase cardiac output in patients with seriously altered cardiac function. Improvement in cardiac contractility may help relieve cardiopulmonary congestions associated with cardiac failure by promoting more complete emptying of the ventricles. Catecholamine agents that have beta-1 adrenergic properties increase myocardial contractility by increasing the levels of cyclic adenosine monophosphate and intracellular calcium available to bind myosin and actin filaments within myocytes.3,4,24,25 Tachydysrhythmia and myocardial ischemia may be induced when positive inotropic agents are given to patients with inadequate preload. Therefore, it is important to administer appropriate fluid resuscitation prior to the administration of positive inotropic medications or simultaneously.9 These agents should be used cautiously in patients with severe aortic valve stenosis and idiopathic hypertrophic subaortic stenosis, as these agents may exacerbate myocardial ischemia and worsen outflow tract obstruction.7
Dopamine
Dopamine (Intropin), at moderate doses of 2 to 10 micrograms per kilogram per minute (mcg/kg/min), primarily stimulates beta-1 adrenergic receptors, which increases cardiac contractility and heart rate.8 At this dose range, dopamine may be used for treating cardiogenic shock and symptomatic bradycardia. At doses less than 2 mcg/kg/min, dopamine stimulates dopaminergic receptors causing renal and mesenteric vasodilation.8 It also exerts a natriuretic effect at low doses, which results in loss of sodium and water in urine. Although these effects may increase urine output, several systematic reviews and one large randomized clinical trial revealed that it does not decrease the incidence of acute kidney injury, the need for renal replacement therapy, or mortality.26–30 Furthermore, Dopamine may worsen kidney function in patients with marginal or inadequate volume status. Therefore, what was once known as ‘renal dose’dopamine is no longer routinely used to improve kidney function.
A common side effect of dopamine is tachycardia, particularly when patients are hypovolemic. Therefore, clinicians should ensure adequate circulating volume before starting this medication. Dopamine increases myocardial cellular metabolism and oxygen consumption, which may result in myocardial ischemia and dysrhythmias. At higher doses, dopamine may inhibit microcirculatory flow because of vasoconstriction, thus limiting its usefulness in the later stages of shock. The vasoconstrictive effects may also increase afterload and decrease cardiac output. Therefore, it is imperative to assess peripheral perfusion at these doses and consider other inotropic agents. Alternatively, a reduction of dopamine to 7.5 mcg/kg/min and simultaneous administration of a second beta-1 agonist agent such as dobutamine may improve cardiac output without excessively increasing afterload and microcirculatory flow.4
Isoproterenol
Isoproterenol (Isuprel), a synthetic catecholamine, is a potent beta-adrenergic agent with minimal alpha-agonist properties. Although it has positive inotropic properties, this effect is attenuated by a decrease in afterload, which results in no marked change in cardiac output. Its usefulness in treating cardiogenic shock is limited because of its ability to increase cardiac impulse conduction and heart rate. Consequently, it is sometimes referred to as the pharmacologic pacemaker and may be used as a temporizing measure for atropine refractory symptomatic bradycardia and heart block until pacemaker therapy can be initiated. It is particularly useful in heart transplant recipients, who have symptomatic bradydysrhythmias and lack parasympathetic innervation of the myocardium. Isoproterenol has beta-2 adrenergic properties that cause bronchodilation and vasodilation of the pulmonary vasculature. Therefore, it may be used to treat refractory bronchospasms. The dose range for isoproterenol is 2 to 10 mcg/min.8 Side effects include tachycardia, myocardial ischemia, ventricular dysrhythmias, anxiety, and flushing.
Inodilators
Inodilators (Table 9-4) are medications that decrease afterload by dilating arteries while also exerting a positive inotropic effect. The combination of increased contractility and vasodilation may be beneficial to patients experiencing cardiogenic shock with increased afterload caused by stimulation of the sympathetic nervous system. Inodilators are also indicated for short-term support to maintain end-organ perfusion in patients with acute heart failure with systolic dysfunction.31
Table 9-4
Inodilator Medications
mcg/kg/min, Micrograms per kilogram per minute; mcg/min, micrograms per minute.
Related posts:
 Hemodynamic Management of Heart Failure and Cardiogenic Shock
Hemodynamic Management of Heart Failure and Cardiogenic Shock
 Hemodynamics of Mechanical Ventilation and Acute Respiratory Distress Syndrome
Hemodynamics of Mechanical Ventilation and Acute Respiratory Distress Syndrome
 Hemodynamics of Acute Right Heart Failure and Pulmonary Hypertension
Hemodynamics of Acute Right Heart Failure and Pulmonary Hypertension
 Ultrasonography-Based Hemodynamic Monitoring
Ultrasonography-Based Hemodynamic Monitoring
 Hemodynamic and Intracranial Dynamic Monitoring in Neurocritical Care
Hemodynamic and Intracranial Dynamic Monitoring in Neurocritical Care
 Oxygenation and Acid–Base Balance Monitoring
Oxygenation and Acid–Base Balance Monitoring

Full access? Get Clinical Tree


