Cathleen Crowley-Koschnitzki
Valvular Heart Disease and Cardiac Murmurs
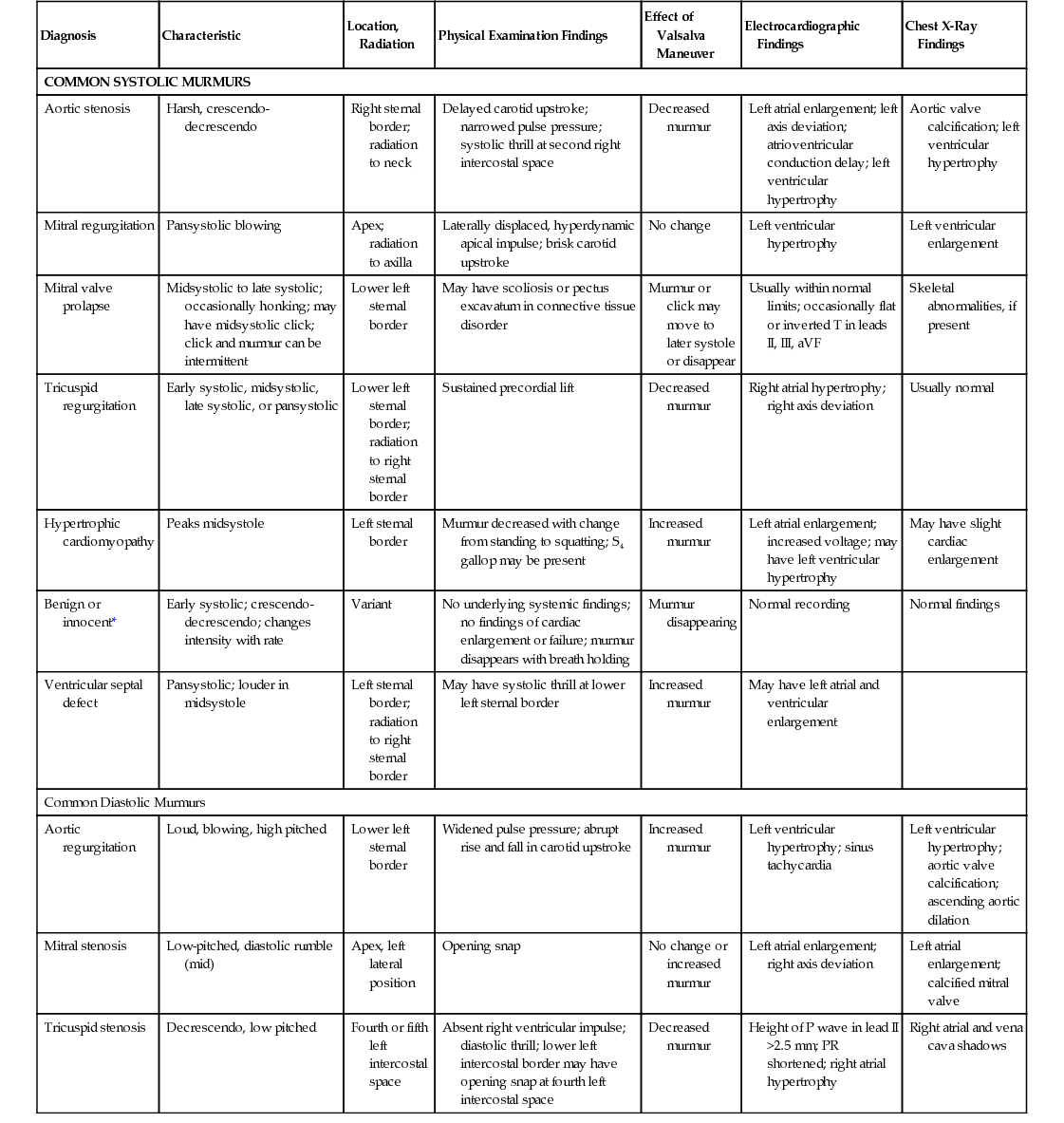
When a murmur is heard for the first time, it is important to determine whether it is from a pathologic condition and what type of condition it may represent. The cause of a murmur, whether benign or malignant, is difficult to determine by auscultation alone. What distinguishes benign from pathologic murmurs is often the characteristics of the murmur, associated physical findings, or symptoms (Table 126-1). Some patients require referral for diagnostic testing, whereas the clinical assessment of others suggests that diagnostic testing is unnecessary.
TABLE 126-1
Murmurs
| Diagnosis | Characteristic | Location, Radiation | Physical Examination Findings | Effect of Valsalva Maneuver | Electrocardiographic Findings | Chest X-Ray Findings |
| COMMON SYSTOLIC MURMURS | ||||||
| Aortic stenosis | Harsh, crescendo-decrescendo | Right sternal border; radiation to neck | Delayed carotid upstroke; narrowed pulse pressure; systolic thrill at second right intercostal space | Decreased murmur | Left atrial enlargement; left axis deviation; atrioventricular conduction delay; left ventricular hypertrophy | Aortic valve calcification; left ventricular hypertrophy |
| Mitral regurgitation | Pansystolic blowing | Apex; radiation to axilla | Laterally displaced, hyperdynamic apical impulse; brisk carotid upstroke | No change | Left ventricular hypertrophy | Left ventricular enlargement |
| Mitral valve prolapse | Midsystolic to late systolic; occasionally honking; may have midsystolic click; click and murmur can be intermittent | Lower left sternal border | May have scoliosis or pectus excavatum in connective tissue disorder | Murmur or click may move to later systole or disappear | Usually within normal limits; occasionally flat or inverted T in leads II, III, aVF | Skeletal abnormalities, if present |
| Tricuspid regurgitation | Early systolic, midsystolic, late systolic, or pansystolic | Lower left sternal border; radiation to right sternal border | Sustained precordial lift | Decreased murmur | Right atrial hypertrophy; right axis deviation | Usually normal |
| Hypertrophic cardiomyopathy | Peaks midsystole | Left sternal border | Murmur decreased with change from standing to squatting; S4 gallop may be present | Increased murmur | Left atrial enlargement; increased voltage; may have left ventricular hypertrophy | May have slight cardiac enlargement |
| Benign or innocent* | Early systolic; crescendo-decrescendo; changes intensity with rate | Variant | No underlying systemic findings; no findings of cardiac enlargement or failure; murmur disappears with breath holding | Murmur disappearing | Normal recording | Normal findings |
| Ventricular septal defect | Pansystolic; louder in midsystole | Left sternal border; radiation to right sternal border | May have systolic thrill at lower left sternal border | Increased murmur | May have left atrial and ventricular enlargement | |
| Common Diastolic Murmurs | ||||||
| Aortic regurgitation | Loud, blowing, high pitched | Lower left sternal border | Widened pulse pressure; abrupt rise and fall in carotid upstroke | Increased murmur | Left ventricular hypertrophy; sinus tachycardia | Left ventricular hypertrophy; aortic valve calcification; ascending aortic dilation |
| Mitral stenosis | Low-pitched, diastolic rumble (mid) | Apex, left lateral position | Opening snap | No change or increased murmur | Left atrial enlargement; right axis deviation | Left atrial enlargement; calcified mitral valve |
| Tricuspid stenosis | Decrescendo, low pitched | Fourth or fifth left intercostal space | Absent right ventricular impulse; diastolic thrill; lower left intercostal border may have opening snap at fourth left intercostal space | Decreased murmur | Height of P wave in lead II >2.5 mm; PR shortened; right atrial hypertrophy | Right atrial and vena cava shadows |
Definition
A murmur is the relatively lengthy series of sounds produced by the turbulent flow of blood. Under normal conditions, blood flow is uniform or laminar within the vessel or chamber and is therefore free of audible vibration. When flow velocity is excessively high or when normal flow occurs across an obstruction, turbulence and its resultant audible vibration occur. In a classic article on auscultation of the heart, Leatham1 noted that all murmurs are related to one of three factors: (1) high rates of flow through a normal or abnormal valve; (2) forward flow through a constricted or irregular valve or into a dilated vessel; or (3) backward flow through a regurgitant valve, septal defect, or patent ductus arteriosus.
Evaluation of Murmurs
Murmurs may be characterized by a number of factors: location, intensity, pitch, radiation, and timing. Of these, timing is the most important factor. Timing delineates the critical division between systolic and diastolic murmurs as well as the relationship to the heart sounds (S1 and S2; e.g., ending well before, right at, or continuing through S2). As the heart rate increases, diastole shortens, and systole and diastole approach similar intervals. When this occurs, differentiation between S1 (beginning of systole) and S2 (beginning of diastole) on the basis of cadence alone becomes difficult. Palpation of the carotid pulse while simultaneously auscultating the heart at the base will easily permit the listener to focus and time S1 (the onset of systole), which will occur slightly before the onset of the carotid pulse rise. The two components of S2 (aortic, or A2, and pulmonic, or P2) are almost superimposed at end-expiration, with inspiration P2 splits later, creating an easily audible gap. This will be best appreciated over the upper left sternal border. A systolic murmur that ends at or before A2 will be a left-sided murmur (e.g., aortic stenosis [AS] or mitral regurgitation [MR]), whereas one that extends beyond A2 will be emanating from the right side of the heart (i.e., pulmonic stenosis or tricuspid regurgitation).
Intensity, or loudness, which is related to the velocity of blood flow, describes how audible the murmur is. However, loudness does not equate with the severity of the underlying problem. Some of the loudest murmurs are caused by a small muscular ventricular septal defect (VSD) in an adolescent that is destined to close spontaneously. Murmurs are graded 1 (barely audible), 2 (faint but clearly heard), 3 (easily heard but without being able to palpate the vibrations on the chest wall), 4 (heard with a palpable thrill), 5 (heard with the stethoscope only partially in contact with the chest wall with a palpable thrill), or 6 (heard without a stethoscope with a palpable thrill). The location where a murmur is best heard is also generally noted (e.g., at the upper right sternal border [second intercostal space], upper left sternal border, lower left sternal border, or apical areas of the chest wall). These terms have largely superseded the earlier descriptors of aortic, pulmonic, tricuspid, and mitral locations because of the variable radiation or transmission of the sounds.
Systolic Murmurs
Systolic murmurs are classified into two general types: ejection type (midsystolic) and regurgitant type (pansystolic). In the ejection type, the murmur is grade 1 or 2, and there is a period between S1 (closure of the mitral and tricuspid valves) and the onset of the murmur. During this time, the ventricle is generating pressure (isovolumetric contraction) to overcome the pressure in the great vessels (aorta and pulmonary artery) and to open the aortic and pulmonic valves. The murmur builds in intensity as velocity increases, followed by a decrease in intensity, which occurs well before S2 (closure of the aortic and pulmonic valves). Thus, the murmur is diamond shaped, or crescendo-decrescendo. This murmur occurs with left ventricular outflow obstruction whether the obstruction is from rheumatic or calcific AS, idiopathic hypertrophic subaortic stenosis (IHSS, also known as hypertrophic obstructive cardiomyopathy), or pneumonic stenosis. Most murmurs are of this type.
In contrast are the murmurs resulting from flow from a high-pressure chamber to a low-pressure chamber, which occurs in incompetent valves (mitral or tricuspid regurgitation) or with a VSD. As soon as pressure starts to develop, flow occurs throughout systole (pansystolic flow). The pressure gradient and therefore the intensity of the murmur are largely unchanged throughout systole. Such murmurs are described as plateau shaped. The murmur of chronic tricuspid regurgitation or MR is the epitome of the pansystolic murmur. However, when a significant gradient or differential of pressure does not exist between chambers, the murmurs will be truncated. Thus, the murmur of severe acute MR may occur only during early systole because of rapid equalization of left atrial pressure with left ventricular pressure. Similarly, the classic murmur of a VSD, which may ordinarily be indistinguishable from that of chronic MR, may be truncated or even totally absent in the face of pulmonary hypertension (Eisenmenger complex). The murmur of mitral valve prolapse (MVP) is classically late systolic, often after a midsystolic click. Variation in intensity of the murmur with respiration is strongly associated with right-sided (pulmonic or tricuspid valve) abnormalities.2
Diastolic Murmurs
Diastolic murmurs are related to regurgitation across either the aortic or the pulmonic valve or to filling rumbles caused by flow across a normal (in exaggerated flow states) or obstructed mitral or tricuspid valve. Listening for the high-pitched diastolic murmur of aortic or pulmonic insufficiency (regurgitation) is difficult and may require proper positioning of the patient. These murmurs are loudest early in diastole, when there is a large pressure gradient between the aorta and the left ventricle; they then fall in intensity as the pressure gradient falls, producing a decrescendo pattern of sound. They are best heard with the patient sitting, leaning forward, and exhaling, all of which minimize the distance from the stethoscope to the heart. The diaphragm of the stethoscope should be used because of the high-frequency response of the murmur.
The cause of the murmur cannot be discerned by the character of the murmur; however, it is generally acknowledged that aortic insufficiency murmurs heard best at the upper right sternal border are more likely to be related to dilation of the aortic root, in contrast to murmurs caused by damage to the aortic valve. If the aortic insufficiency is acute and severe, the duration of the murmur may be truncated as a result of the rapid and premature equalization of pressures between the left ventricle and the aorta. Pulmonic insufficiency is usually found in the setting of pulmonary hypertension with dilation of the pulmonic artery and produces a Graham Steell murmur, which by clinical examination is almost indistinguishable from the murmur of aortic insufficiency. Low-pitched rumbles in diastole are caused by forward flow across a stenotic mitral or tricuspid valve. Such low-pitched murmurs are best appreciated by use of the bell of the stethoscope at the apical area with the patient lying slightly on the left side. Because the filling of the ventricles occurs primarily in early diastole (the rapid filling phase) and at the end of diastole (from atrial contraction), the murmur is loudest during these times. Therefore patients with atrial fibrillation will lack the presystolic accentuation of their diastolic rumbles because they have no atrial contraction.
The duration, not the intensity, of the murmur correlates with the severity of the obstruction. Less-severe stenosis will result in a shorter gradient across the stenotic valve and a shorter murmur; more severe stenosis will result in a longer gradient across the stenotic valve and a longer murmur (to the end of diastole). Hyperdynamic states, such as anemia and fever, or the presence of atrial septal defects or VSDs producing shunting of blood from one chamber to the other during diastole may produce murmurs in mid-diastole. Left atrial myxomas may obstruct flow across the mitral valve during diastole, producing a similar rumble but one that is associated with a “tumor plop” instead of an opening snap.
Continuous Murmurs
Continuous murmurs begin in systole and extend at least partway into diastole. Continuous murmur causes include rapid blood flow, high to low pressure shunts, or localized stenosis.3 The classic continuous murmur is exemplified by the murmur associated with a patent ductus arteriosus. Intracardiac shunting between a high-pressure system (aorta) and a low-pressure system (pulmonary artery) exists throughout the cardiac cycle and may be heard in the region just beneath the left clavicle. Fistulas or localized arterial obstructions may also produce continuous murmurs. In addition, continuous murmurs are often associated with benign high-flow states. A continuous murmur known as a venous hum and heard in the neck is commonly noted in children and adolescents. It may be abolished by compression of the jugular vein. Similarly, women in the late stages of pregnancy or lactating women shortly postpartum may develop a continuous “mammary shuffle” over the breast that may be obliterated with firm pressure.
Flow Murmurs (Benign and Pathologic)
Murmurs that are not caused by any pathologic obstruction to flow are termed innocent, benign, or functional. As noted previously, the acoustic-mechanical phenomena that create benign or innocent murmurs are the same as those that create pathologic conditions. The differentiation is based on the lack of other findings (e.g., abnormal carotid or peripheral pulses, associated symptoms). Several clues may help distinguish innocent murmurs from pathologic ones.3 Murmurs that are caused by an increased cardiac output (e.g., as a result of fever, thyrotoxicosis, anemia) may be termed functional because they are caused by excess flow across the outflow tract. Many older adults have decreased mobility of the aortic valves as a result of fibrosis and calcification (aortic sclerosis), which distorts the flow without producing a significant gradient across the valve. Other older patients may have outflow murmurs that are caused by ejection of blood into a kinked, tortuous aorta.
2014 American College of Cardiology/American Heart Association Guidelines
The 2014 American College of Cardiology (ACC) and American Heart Association (AHA) guidelines for the management of patients with valvular heart disease (VHD) updated the recommendations for evaluation and management of adult patients. General recommendations include a through history and complete physical examination on all patients with suspected or known heart disease. The presence or absence of symptoms guides progression staging and treatment (Table 126-2). Recommendations for initial diagnostics of VHD include transthoracic echocardiogram (TTE) with two-dimensional (2D) imaging and Doppler studies, which provides necessary anatomic and hemodynamic measurements. Transthoracic echocardiography is the standard diagnostic test for the initial evaluation of patients with suspected or known VHD. Classification of the severity of valve disease is determined from physical examination findings and TTE results.4 Monitoring of asymptomatic VHD patient status by periodic TTE varies based on lesion, severity level, and valvular function. For patients with known VHD, a change in symptoms or the physical examination findings warrants a repeat TTE. Cardiac catheterization is recommended for symptomatic patients with inconclusive TTE results or when there is a discrepancy between physical examination findings and noninvasive testing results (see Table 126-2).4

Aortic Stenosis
Definition and Epidemiology
AS is a disorder associated with advancing age. Purely based on clinical findings, it is more difficult to assess the degree of severity of AS than it is to assess any other valvular abnormality. Valvular AS may be caused by rheumatic damage, congenital abnormality (bicuspid aortic valve), or degeneration by the aging process (calcific AS of older adults).5 During the past three decades, with the successful treatment of streptococcal pharyngitis, the etiology has shifted away from rheumatic to calcific. A history of 20 to 30 years of repetitive mechanical trauma of the blood against the valve results in inflammation, fibrosis, calcification, and eventually stenosis. This progression of calcification within the valve cusps is usually seen during the latter decades of life. An inflammatory process similar to that causing the development of atherosclerotic plaques in coronaries may be a possible cause of the progression of AS.5 AS is staged based on symptomatology, valve anatomy, and hemodynamics.
Pathophysiology
Any reduction of the normal aortic valve orifice of approximately 3 cm2 ( square inches) will cause obstruction to the flow of blood from the left ventricle into the aorta during ventricular systole. A systolic pressure gradient develops between the left ventricle and the aorta. Left ventricular pressure rises, increasing systolic wall stress. The left ventricle hypertrophies as a compensatory mechanism to maintain adequate cardiac output. Valvular stenosis is generally considered to be significant when the valve area is reduced to 25% of normal. Therefore, hemodynamically significant AS would be an aortic valve area of less than 0.75 cm2 (
square inches) will cause obstruction to the flow of blood from the left ventricle into the aorta during ventricular systole. A systolic pressure gradient develops between the left ventricle and the aorta. Left ventricular pressure rises, increasing systolic wall stress. The left ventricle hypertrophies as a compensatory mechanism to maintain adequate cardiac output. Valvular stenosis is generally considered to be significant when the valve area is reduced to 25% of normal. Therefore, hemodynamically significant AS would be an aortic valve area of less than 0.75 cm2 ( square inch) in an adult, which is associated with a gradient of more than 50 mm Hg. A large pressure gradient across the aortic valve may be sustained for many years without a reduction in contractile function, with left ventricular dilation generally a very late manifestation. Persistent pressure overload to the left ventricle may eventually lead to left ventricular dilation, left atrial enlargement, and pulmonary hypertension.
square inch) in an adult, which is associated with a gradient of more than 50 mm Hg. A large pressure gradient across the aortic valve may be sustained for many years without a reduction in contractile function, with left ventricular dilation generally a very late manifestation. Persistent pressure overload to the left ventricle may eventually lead to left ventricular dilation, left atrial enlargement, and pulmonary hypertension.
Clinical Presentation
Chest pain, syncope, exercise intolerance, and dyspnea are the classic symptoms associated with severe AS. With chronic AS, there generally is a long latent period before the development of symptoms. By the time clinical symptoms are present, AS can be advanced.5 Angina and syncope manifest whereas the left ventricular function remains preserved; dyspnea indicates congestive heart failure (CHF) and left ventricular dysfunction. Angina pectoris is a frequent symptom among patients with AS. Anginal symptoms in AS may be caused by an increased myocardial oxygen demand related to increased wall tension combined with a reduction in coronary blood supply.5 This may occur even in the presence of normal coronary arteries. 4 Heart failure is a late clinical sign and is associated with poor prognosis.5
Although it is uncommon, patients with severe AS are at a higher risk of sudden death when anginal symptoms are present. Dizziness or frank syncope occurs in patients and has been attributed to an abrupt fall in systemic vascular resistance in the presence of a fixed cardiac output, abrupt failure of the overloaded left ventricle during effort, or arrhythmia.5 Left ventricular failure eventually occurs with symptoms of fatigue, cough, progressive dyspnea on exertion, orthopnea, and paroxysmal nocturnal dyspnea.5
Physical Examination
No physical finding can reliably assess the severity of AS obstruction. Classically, the carotid pulse has a slow rise with delayed peak and small volume (pulsus parvus and pulsus tardus). A notch or shudder in the upstroke (anacrotic notch) may be appreciated. Auscultation reveals a harsh (grade 3/6 or greater) crescendo-decrescendo systolic ejection murmur that begins after the first heart sound. The murmur of AS is loudest at the second right sternal edge and radiates to the left lateral sternal border and carotids. A thrill is often present. The murmur may become softer or even inaudible in patients with end-stage AS. Paradoxical splitting of the second heart sound (S2) occurs as a result of delay in closure of the aortic valve. In severe stenosis, the A2 is often inaudible; therefore, no splitting of S2 is appreciated. An additional early systolic ejection sound or click may be heard, more commonly in younger patients with congenital or bicuspid AS. Left ventricular hypertrophy (LVH) produces a sustained thrust or heave of the apical impulse. Displacement of the apical impulse downward and to the left occurs after left ventricular failure develops and the ventricle dilates.
Diagnostics
Recommendations for initial diagnostics include electrocardiography (ECG), chest x-ray examination, and TTE with 2D imaging and Doppler studies. TTE is the standard diagnostic test for the initial evaluation of patients with suspected or known VHD.4 In patients with AS, normal findings (e.g., lack of LVH or normal chest x-ray findings) do not exclude severe disease. ECG demonstrates normal sinus rhythm with signs of LVH. Atrial fibrillation usually represents either end-stage disease with left ventricular decompensation or other associated disease. Conduction abnormalities, such as first-degree atrioventricular block, bundle branch block, and intraventricular conduction disturbances, are fairly common. The chest x-ray film may demonstrate rounding or prominence of the left ventricle as a result of concentric hypertrophy of the left ventricle, poststenotic dilation of the aorta, and calcification of the valve cusps, or the chest x-ray findings may be completely normal.
In contrast, a technically satisfactory, well-performed 2D echocardiogram has the ability to exclude significant obstruction of the aortic valve. The Doppler portion of the examination is able to provide an assessment of the outflow gradient that closely approximates that obtained by cardiac catheterization. By combining Doppler ultrasonography and echocardiography, the examiner may make a reasonable calculation of the aortic valve area. Thickened, calcified, and immobile leaflets are readily noted by transthoracic 2D echocardiography. The echocardiogram also demonstrates poststenotic dilation of the aorta and left ventricular wall thickening. Dilation of the left ventricle or reduced contractility (ejection fraction) occurs with myocardial failure. Equally important, additional valvular abnormalities (e.g., MR or mitral stenosis [MS]) are apparent, as are the findings of IHSS.
Cardiac catheterization can determine the severity of obstruction by recording the gradient across the valve and by calculating the valve area. Additional functional assessment of the left ventricle is possible. In the current era, these findings often confirm those obtained by Doppler echocardiography. In adults, the major indication for cardiac catheterization is to delineate the coronary anatomy. Even in patients without angina, approximately 50% will have significant coronary obstructions.6
Differential Diagnosis
The major condition in the differential diagnosis for a systolic ejection murmur without valvular disease is the functional or innocent murmur (i.e., flow murmur without disease). The absence of symptoms or other physical abnormalities will generally lead to this diagnosis. In adults, the major pathologic state that must be differentiated is IHSS, or hypertrophic obstructive cardiomyopathy. These patients may have similar symptoms; however, the carotid upstroke is very brisk, with at times two distinct humps (pulsus bisferiens). The primary distinguishing characteristic is the murmur’s response to maneuvers that increase or decrease the dynamic obstruction. Thus, standing or the strain phase of the Valsalva maneuver decreases venous return, resulting in a smaller left ventricular outflow tract and an increase in the murmur intensity.
Differential Diagnosis
Systolic Murmurs







