, Corinna Eleni Psomadakis2 and Bobby Buka3
(1)
Department of Family Medicine, Mount Sinai School of Medicine Attending Mount Sinai Doctors/Beth Israel Medical Group-Williamsburg, Brooklyn, NY, USA
(2)
School of Medicine Imperial College London, London, UK
(3)
Department of Dermatology, Mount Sinai School of Medicine, New York, NY, USA
Keywords
UrticarialExanthemaExanthemHivesWhealWeltHistamineInflammatoryInflammationDermatographismAllergiesAntihistamineCetirizine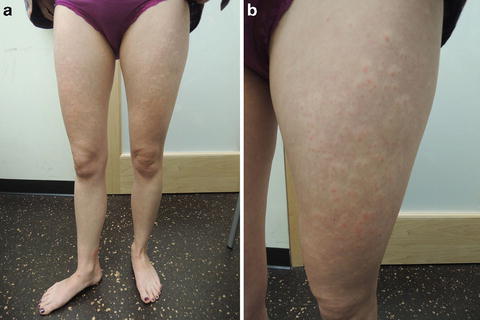
Fig. 44.1
(a and b) Edematous wheals with perilesional pallor on the bilateral lower extremities
Primary Care Visit Report
A 29-year-old female with no past medical history presented with a diffuse, itchy, erythematous papular rash . The rash was most severe on her anterior and posterior lower extremities bilaterally, and less prominent on her lower abdomen and lower forearms. The rash started 2 days prior to her visit and got progressively worse over that time. She felt well otherwise. She reported no new lotions, detergents, or clothes. She got a flu shot 2 days prior (which she had received in the past without incident and she denied an egg allergy), otherwise there were no new medications. The rash started later in the afternoon after she got her flu shot. The rash on her hands worsened with contact with hot water. She had taken 50 mg of benadryl the day before and the day of the visit, and the rash continued to progress and to become more itchy.
Vitals were normal. On exam, there was a diffuse, papular, erythematous blanchable rash on her anterior and posterior thighs, lower legs, and ankles bilaterally. Hypopigmentation surrounded the erythematous papules. The rash was less severe but similar in appearance on her lower abdomen and bilateral forearms and hands. There was one 3 cm × 3 cm erythematous wheal on the patient’s right medial ankle area.
The patient was treated for hives or a possible allergic reaction (to an unknown allergen). She was put on a 15-day prednisone taper (80 mg for 3 days, 60 mg for 3 days, 40 mg for 3 days, 20 mg for 3 days, 10 mg for 3 days).
Discussion from Dermatology Clinic
Differential Dx
Urticaria
Viral exanthem
Contact dermatitis
Erythema multiforme
Urticarial vasculitis
Favored Dx
Urticaria is favored.
Overview
Urticaria, commonly known as hives , is a raised, pruritic edematous rash. It occurs when a stimulus activates mast cells, causing a massive release of histamine and inflammatory mediators that results in leaky capillaries and, consequently, the appearance of wheals .
Urticaria is common, affecting one in five people at some point in their lifetime [1–3]. It can affect people of any age and gender, but commonly occurs in children and middle-aged women [2]. Urticaria is classified as acute (resolving within 6 weeks) or chronic (recurrent, lasting longer than 6 weeks). Chronic urticaria is much less common, with a 0.5 % incidence [3], and twice as likely to occur in women than men [2]. Chronic urticaria is subtyped as autoimmune and idiopathic. Chronic urticaria is associated with underlying health conditions, including thyroid problems and lupus. A common type of chronic urticaria is dermatographism , which is characterized by the appearance of raised welts after the skin is scratched, rubbed, or slapped.
Urticaria can be triggered by a number of allergic or nonallergic factors, and can be further categorized according to the causative agent. These triggers include foods, medications, insect bites, plants, pollen, animal dander, pressure, emotional stress, sweat (cholinergic urticaria), some viral, bacterial, and fungal infections, and exposure to heat, cold, water, or sunlight. Fewer than half the cases of acute urticaria have an obvious cause.
Related posts:







Full access? Get Clinical Tree


