INTRODUCTION
BLADDER DRAINAGE/TUBES
Anesthetic jellies (gels), such as lidocaine 2%, reduce the discomfort of male catheterization, although this is not true in women.1,2 Lidocaine jelly may not be available, so it helps to know about the alternatives.
Diphenhydramine (e.g., Benadryl) and promethazine (e.g., Phenergan) may be used effectively as urethral anesthetics. The dose is the same, or less, than would be used orally. Inject the drug into the urethra using a bulb syringe, and keep it in place for about 5 minutes using a penile clamp or equivalent. Some patients experience an initial burning sensation. The anesthesia lasts about 1 hour. To obtain more extensive anesthesia, coat a small urethral sound with an ointment of these medications and leave in it place about 5 minutes before passing larger sounds.3
Use mineral oil to lubricate urethral catheters if standard lubricating jellies are unavailable.4 In women, apply 10% cocaine jelly with a cotton-tipped applicator for an effective urethral anesthetic. Leave this in place for 5 minutes.5
Passing a urethral catheter is almost routine from the clinician’s perspective. Some catheters are difficult to pass, especially in older men. When calling the urologist is not an option, the following technique may make catheter insertions more successful.
In males >50 years old, use a syringe to inject 25 to 50 mL lidocaine jelly 2% into the urethra before attempting to pass any catheter. If lidocaine jelly is not available, use any sterile gel (e.g., K-Y). If you anticipate that passing a urethral catheter will be difficult, use at least an 18- to 20-Fr Foley rather than a smaller-sized catheter. Smaller catheters simply bend if they hit an obstruction, rather than passing into the bladder. Use slow, steady pressure to insert it all the way to the Foley’s hub. Do not inflate the balloon until the catheter is fully inserted and urine returns.
Use a coudé catheter if you suspect that the patient may have an enlarged prostate. A coudé catheter has a gentle upward curve at its distal 3 cm that allows easier passage through an enlarged prostate. When inserting a coudé catheter, point the tip anteriorly. This means that the balloon inflation side port should be facing up (on the same side as the curve). If the patient has a red catheter in place, it generally means that it is either a coudé or a Councill (used by urologists to pass over a guidewire). In either case, beware of removing it for replacement.
If multiple attempts at catheter placement have failed, a suprapubic aspiration using a needle and large syringe can easily buy time until a suprapubic tube can be placed or an experienced clinician can use alternative methods (e.g., filiforms and followers) to drain the bladder.
Bladder clots are reasonably common and often cause painful obstructive symptoms. Assuming that you know why these are occurring (chronic infection, tumor, anticoagulant), treat the acute problem and ensure bladder drainage. To do this, put in a ≥4-Fr catheter. Do not place a three-way catheter, which is normally used for continuous bladder irrigation, until the clot is removed—the opening is too small, because two smaller catheters and an inflation port must fit into the one catheter. Advance the catheter all the way. It may pass beyond the clot and allow the urine to drain. Then use an irrigation syringe to instill 60 to 120 mL aliquots of sterile water, which is more lytic than saline (up to 300 mL total). Then withdraw the fluid and repeat the process. If the clot cannot be removed in this fashion, a surgical approach may be necessary. If surgery is not an option, some clinicians have instilled thrombolytics.6,7
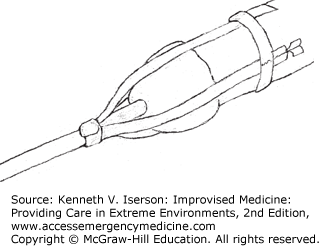
If only a straight (non-balloon) catheter or a makeshift catheter (e.g., a nasogastric tube) must be placed, the trick is securing it to the penis. After inserting the tube, secure it to the penis using three long strips of adhesive tape. First, attach about 1 inch of a tape strip to the catheter just as it exits the urethra. Lay the rest of the tape along the penis. Do the same for the two other pieces of tape. Use benzoin, if necessary, to keep the pieces in place. Then wrap one or two non-constricting circular pieces of tape around the penis to secure the long strips further (Fig. 33-1).
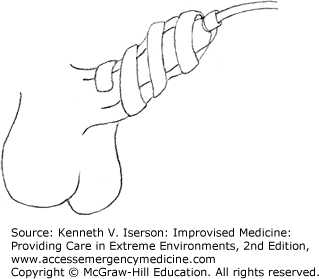
Another method of securing a non-balloon catheter is to tie a suture around the catheter just beyond the external meatus and carry the ends along the body of the penis (Fig. 33-2). Secure the ends with a piece of tape, wrapping it in a spiral beginning at the catheter and then around the penis.8
In infants, using a pediatric feeding tube as a catheter is common. Matt Steinway, MD, a urologist in Phoenix, Ariz., suggests securing these with a clear adhesive dressing (e.g., OpSite) or with a suture placed through the glans and tied to the tube at the meatus. (Personal written communication, February 2008.)
In women, securing a straight catheter may be less successful. It can be taped to the labia, after shaving.9 Alternatively, as Keyes wrote in 1917, “In the female, the (non-balloon) catheter is held in place by tying a number of silk strings to it as it issues from the vulva and fixing these to the pubic hairs in front, and by means of adhesive strapping to the lateral gluteal creases behind.”10
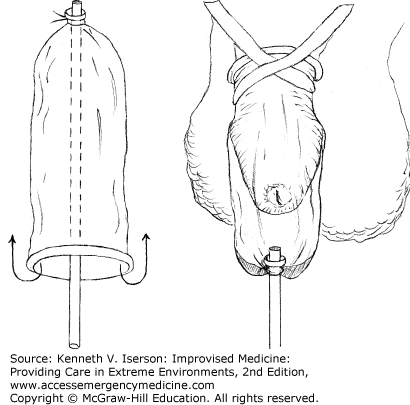
A condom (external) catheter can easily be improvised using a normal condom and any tube that connects to the collection bottle or bag. Slip the end of the tube completely into the condom. Make a small hole at the end of condom, but don’t pass the tube through it or it will rub against the penis. Tie the end of the condom tightly around the end of the tube, and invert the condom so it dangles free of the tube (Fig. 33-3). Put the condom over the penis and secure it with tape around the penis, extending the tape onto the anterior abdomen. In many cases, a Penrose drain, a glove, or other material can be used in place of a condom.
Between intermittent catheterization of the same patient, clean catheters as follows:
Related posts:







Full access? Get Clinical Tree


