DEFINITION
Unintended neuraxial anesthesia is one of the most severe complications that can occur during performance of a peripheral or plexus block (Box 18-1). The interscalene approach to the brachial plexus is a classic example of how local anesthetic can be unintentionally injected into the epidural, subdural, or subarachnoid spaces, thereby resulting in high spinal or massive epidural anesthesia. As one moves caudad along the neuraxis, unintended subarachnoid or epidural injection may also occur during paravertebral or psoas compartment blocks.
BOX 18-1 Unintended Destinations of Local Anesthetic
 Soft tissue spread: cervicothoracic sympathetic chain, vagus or recurrent laryngeal nerve
Soft tissue spread: cervicothoracic sympathetic chain, vagus or recurrent laryngeal nerve
 Intravascular injection or vascular uptake from adjacent tissues
Intravascular injection or vascular uptake from adjacent tissues
 Hollow viscus perforation with local anesthetic deposition and/or needle trauma
Hollow viscus perforation with local anesthetic deposition and/or needle trauma
Systemic local anesthetic toxicity is fully discussed in Chapter 7. There is, however, an aspect of proximal brachial plexus block that deserves further emphasis with regard to intravascular injection. Because these blocks occur in close proximity to arteries that directly supply the brain, unintentional injection of even extremely small amounts of local anesthetic into the vertebral, carotid, or subclavian artery (followed by retrograde flow into the carotid or vertebrals) can result in the rapid development of seizures. Indeed, vertebral artery injection of 2.5 mg of bupivacaine has caused a convulsion during performance of an interscalene block.
Less serious than intra-arterial injection or direct injection near the neuraxis is the soft tissue spread of local anesthetics to anatomic structures near the intended neural target. These side effects occur most commonly during proximal approaches to the brachial plexus, such as with interscalene or supraclavicular blocks. Unintended spread to the cervicothoracic sympathetic chain results in Horner’s syndrome (characterized by ptosis, miosis, and anhydrosis), whereas local anesthetic may also affect the nearby vagus or recurrent laryngeal nerves, causing hoarseness.
 SCOPE
SCOPE
The incidence of unintended neuraxis involvement from interscalene block is not well defined. Epidural and spinal extension have been reported in isolated case reports,1–6 wherein the vast majority occur with Winnie’s technique and some with the posterior approach (i.e., the cervical paravertebral block). For the psoas compartment approaches, Macaire et al.7 reported a retrospective study including 4,319 blocks performed by 42 teams. Spinal extension occurred in 0.6% of blocks, whereas epidural diffusion varied from 1% to 10% according to each team.
Minor problems such as Horner’s syndrome occur in 12% to 75% of brachial plexus blocks using the interscalene or especially the supraclavicular approach.8 Recurrent laryngeal nerve block occurs more frequently on the right side, and its incidence varies from 6% to 12% with interscalene block, or 1.3% with supraclavicular block.8 Horner’s syndrome and hoarseness may occur concurrently.
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Neuraxial Placement
Various mechanisms may be implicated in the occurrence of total spinal or high epidural anesthesia following interscalene block (Box 18-2). Direct injection into the subdural (or epidural) space may be the consequence of incorrect needle placement through an intervertebral foramen. A perineural or intraneural injection may lead to a secondary migration of the drug into the subdural space.8 Selander and Sjostrand9 demonstrated that 20% of endoneural sciatic nerve injections reached the spinal cord. In their rabbit model, endoneural (intrafascicular) injections were associated with high pressure (300–750 mm Hg) and caused a rapid spread of radioisotope-labeled local anesthetic over long distances within the fascicle. This study showed that the fascicle is not just a grouping of nerve fibers but a conduit connecting the peripheral nervous system with the central nervous system(CNS). Finally, long dural root sleeves have been shown in autopsy studies to extend as far as 3 to 5 cm beyond the intervertebral foramen. Placement of a needle into an abnormally long dural root sleeve10 may therefore provide another explanation for the unintended transfer of local anesthetic into the intrathecal space11 (Fig. 18-1).
BOX 18-2 Plexus Blocks and Neuraxial Anesthesia: Pathways to the Spinal Cord
 Injection through the intervertebral foramen, leading to epidural, subdural, or subarachnoid placement
Injection through the intervertebral foramen, leading to epidural, subdural, or subarachnoid placement
 Retrograde local anesthetic migration via the intervertebral foramen into the epidural space
Retrograde local anesthetic migration via the intervertebral foramen into the epidural space
 Injection into the dural root sleeve
Injection into the dural root sleeve
 Distal intrafascicular injection with retrograde migration to the spinal cord
Distal intrafascicular injection with retrograde migration to the spinal cord
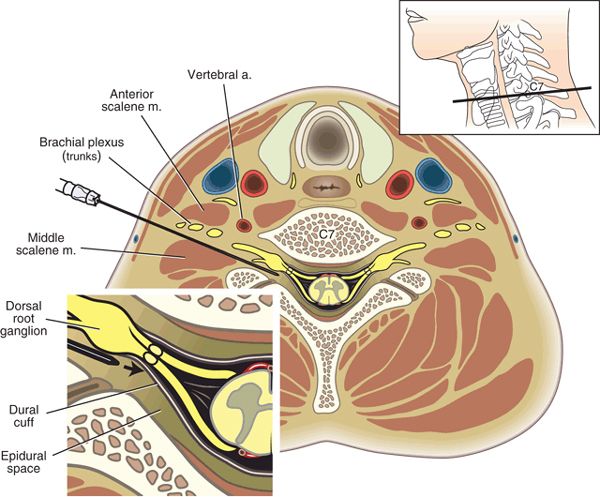
FIGURE 18-1. Axial section of the left neck. Note the proximity of the brachial plexus to the dorsal nerve root ganglia (needle). The spinal nerve root cuff is medial to the ganglia. Note also the proximity of the epidural space, the subarachnoid space, and the vertebral artery. (Drawing based on cryomicrotome section by Quinn H. Hogan, M.D. Modified from Neal JM, Hebl JR, Gerancher JC, et al. Brachial plexus anesthesia: essentials of our current understanding. Reg Anesth Pain Med 2002;27:402–428, with permission.)
Unintended neuraxial injection or spread of local anesthetic consequent to psoas compartment or paravertebral block may follow a similar pathway as described previously. Direct intrafascicular injection or injection via the intervertebral foramen or dural root sleeve is possible, as is retrograde local anesthetic spread into the epidural space.
Soft Tissue Spread
The stellate ganglion and recurrent laryngeal nerve lie in close proximity to the brachial plexus in the lower neck. The stellate ganglion is positioned anteriorly and between the transverse process of C7 and the first rib and lies behind the vertebral artery (Fig. 18-2). The right recurrent laryngeal nerve leaves the vagus as it crosses the subclavian artery, loops under it, and ascends in the tracheoesophageal groove. On the left side, it leaves the vagus as it crosses the aortic arch, loops under the arch, and ascends in the tracheoesophageal groove (Fig. 18-3). These structures may be easily affected during interscalene block, particularly if the Winnie or posterior approaches are performed.
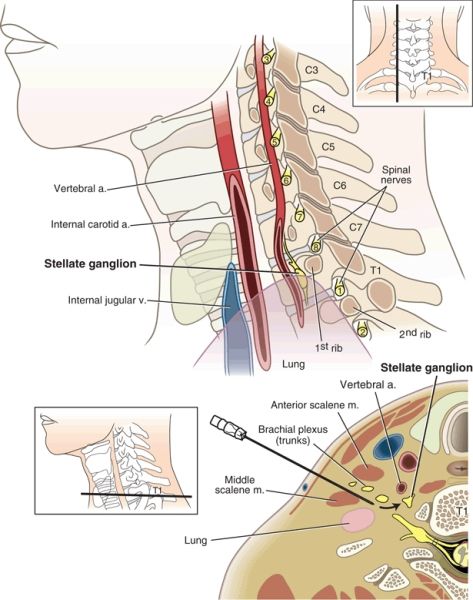
FIGURE 18-2. Parasagittal section of the neck demonstrating how local anesthetic may affect the stellate ganglia during the performance of an interscalene block. Note the proximity of the stellate ganglia to the C8 and T1 nerve roots. The jugular vein and internal carotid artery are seen in longitudinal section. (Drawing based on cryomicrotome section by Quinn H. Hogan, M.D. Modified from Neal JM, Hebl JR, Gerancher JC, et al. Brachial plexus anesthesia: essentials of our current understanding. Reg Anesth Pain Med 2002;27:402–428, with permission.)



