Understand and Take Advantage of the Unique Properties of Helium for the Management of the Compromised Airway
J. Mauricio Del Rio MD
Theresa A. Gelzinis MD
A 22-month-old girl began coughing while eating some sunflower seeds. Shortly thereafter, she appeared to be gasping for air. Her mother performed back blows and called for an ambulance. In the emergency department she was awake, alert, and sitting forward with obvious stridor, increased work of breathing, frequent coughing, and drooling. The patient was transported emergently to the operating room for airway management. When you arrive, her vital signs are blood pressure 119/76 mm Hg, respiratory rate 66 breaths/min, heart rate 160 beats/min, and pulse oximetry 90% with some blow-by oxygen. Examination of the chest reveals mild retractions and faint bilateral wheezing. While awaiting the arrival of the ENT surgeon, the patient has intermittent episodes of perioral cyanosis, repetitive coughing, and worsening stridor. How would you manage this patient?
Since 1934, when helium was first described as therapy for upper-airway obstruction and asthma exacerbation, it has been advocated for the treatment of a wide variety of respiratory conditions. However, the optimal application and effectiveness of the helium—oxygen mixture (heliox) for managing air flow obstructive disorders has not been clearly supported by the evidence. It is important to understand the mechanism of action and the scenarios in which this therapy is and is not warranted.
PHYSICAL PROPERTIES OF HELIUM
Helium is a colorless, odorless, tasteless, monatomic element. It is the first noble gas in the periodic table, with an atomic number of 2 and an atomic weight of 4 g/mol. Helium is the second most abundant element in the universe but relatively rare on earth, representing 0.000524% of the atmosphere. With the lowest boiling and melting points of the elements, helium exists as a gas except in extreme conditions. In natural conditions, most helium is created by the radioactive decay of heavier elements and is trapped within natural gas in concentrations up to 7%. Helium is extracted from natural gas by fractional distillation. At a temperature near absolute zero the liquid helium has virtually no viscosity, a property called superfluidity.
As a consequence of its low atomic weight, the density of helium is the lowest of any gas except hydrogen; unlike hydrogen, it is nonflammable. Helium’s low density allows CO2 to diffuse five times more rapidly through a helium—oxygen mixture than through air or oxygen. Being biologically inert, helium has no direct pharmacologic effects and has no intrinsic bronchodilatory or anti-inflammatory properties. For the same reasons, it has no known toxic effects, even when used for extended periods of time.
HELIOX
Heliox is a mixture of helium and oxygen gases. Standard heliox cylinders contain 80:20 heliox, though heliox also is also available in 70:30 and 60:40 mixtures. Commercial-grade heliox is available in H-size cylinders, which contain approximately 1,200 L of gas, at approximately 2,200 psi. If the patient requires supplemental oxygen, this limits the helium concentration that can be administered.
HISTORICAL USES OF HELIOX
Helium was discovered in 1868 by a French astronomer, Janssen, as a bright yellow line in the spectrum of the sun during a solar eclipse. The new element was first isolated on Earth in 1895 by a British chemist, Ramsay. At the time of its discovery, helium had no practical use. Heliox was first used physiologically to create breathing environments for diving. It reduced the formation of nitrogen bubbles responsible for decompression illness in divers and allowed them to work at depth for extended periods of time. In 1934, Barach noted the biologic inertness of heliox; he found no ill effects in mice exposed to a high helium concentration for 2 months. Those experiments were followed by clinical investigations of its potential benefits for various disorders, including asthma and infant airway obstruction. Barach noted evidence of relief within 6 to 10 breaths, with dyspnea returning in as little as 3 to 4 breaths after discontinuation of heliox. After the late 1930s, little was reported about clinical applications of heliox until 1979. Since then, there has been a resurgence in the investigation of its potential uses.
PHYSICS OF FLUID FLOW WITH HELIOX
The behavior of a fluid in flow is related to two intrinsic properties of the fluid: density and viscosity. The density of a substance is its mass per unit volume. Because 1 gram molecular weight of a gas occupies a volume of 22.4L under standard conditions, gas density is its gram molecular weight divided by 22.4 L. The density of helium is thus 0.179 g/L. Oxygen’s molecular weight is 32 g, so its density is 1.43 g/L. Viscosity is an internal property of a fluid. Viscosity causes resistance to flow. A fluid with a high viscosity strongly resists flow.
Gas flow can vary from laminar at one end of the spectrum to turbulent at the other. Under normal circumstances, gas flow in many parts of the respiratory tract is largely laminar and follows the Hagen—Poiseuille law. This law states that the fluid flow rate (Q) through a straight tube of uniform bore is proportional to the pressure gradient (ΔP) and the fourth power of the radius (r), and is related inversely to the viscosity of the gas (µ), and the length (l) of the tube:
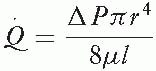
Flow varies directly with pressure, so quadrupling the pressure will quadruple the flow; it also varies as the fourth power of the radius, so doubling the radius will increase flow by a factor of 16. Note that laminar flow is viscosity-dependent and density-independent. Because the viscosity of helium, oxygen, and air is similar and laminar flow velocity is independent of density, heliox has no effect on areas of laminar flow.
Turbulent flow occurs in constricted passages and follows a different law:
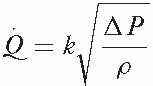
Compared with laminar flow, turbulent flow is less efficient. Flow increases with the square root of the pressure gradient, so quadrupling the pressure gradient merely doubles the flow. Decreasing the density will also increase the flow. As flow velocity decreases and/or airway resistance increases, there is a critical level at which the flow pattern changes from laminar to turbulent. This transitional zone is defined by Reynolds number (Re):
Related posts:
 Never Neglect the Basics of Airway Management
Always Troubleshoot An Increase in Peak Airway Pressure
Do Not Start the Airway Management of a Ludwig Angina Patient Until Personnel and Equipment for a Definitive (Surgical) Airway Are Assembled
Do Not Use the Subclavian Vein for Central Access of Any Type in a Patient Planned for Dialysis
Never Neglect the Basics of Airway Management
Always Troubleshoot An Increase in Peak Airway Pressure
Do Not Start the Airway Management of a Ludwig Angina Patient Until Personnel and Equipment for a Definitive (Surgical) Airway Are Assembled
Do Not Use the Subclavian Vein for Central Access of Any Type in a Patient Planned for Dialysis
 Consider the Use of Tris-Hydroxymethyl Aminomethane (THAM) to Treat Refractory or Life-Threatening Metabolic Acidosis
Be Aware of the Drugs that Require Slow Intravenous Administration
Consider the Use of Tris-Hydroxymethyl Aminomethane (THAM) to Treat Refractory or Life-Threatening Metabolic Acidosis
Be Aware of the Drugs that Require Slow Intravenous Administration

Full access? Get Clinical Tree


