CHAPTER 135
Ulnar Collateral Ligament Tear of the Thumb
(Ski Pole or Gamekeeper’s Thumb)
Presentation
The patient fell while holding onto a ski pole, banister, or other fixed object, forcing his thumb radially into abduction and causing pain at the base of thumb. The metacarpophalangeal (MCP) joint of the thumb is swollen and tender and may be ecchymotic. When tested for stability, it may show varying degrees of joint widening toward the radial (or palmar) aspect more than the metacarpophalangeal joint of the other thumb. The patient’s power pinch between the thumb and index finger, if possible at all, is less strong than with the other hand (Figure 135-1).
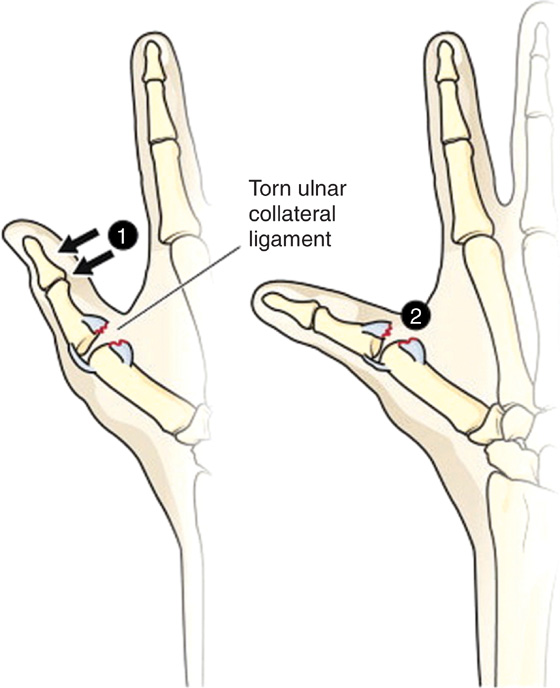
Figure 135-1 Rupture of the ulnar collateral ligament (gamekeeper’s thumb). 1, This injury is caused by forcible abduction. If unrecognized and untreated, progressive MCP subluxation may occur (2) with interference during grasp, causing significant permanent disability. Suspect this injury when there is a complaint of pain in this region. Look for tenderness on the medial side of the MCP joint. (From Roberts JR, Hedges JR: Clinical procedures in emergency medicine, ed 5. St Louis, Saunders, 2009. Adapted from McRae R: Practical fracture treatment. Edinburgh, 1981, Churchill Livingstone. Reproduced by permission.)
What To Do:
 Obtain a history of the mechanism of injury, and examine the thumb, hand, and wrist thoroughly. Tenderness to palpation should be greatest along the ulnar border of the proximal thumb.
Obtain a history of the mechanism of injury, and examine the thumb, hand, and wrist thoroughly. Tenderness to palpation should be greatest along the ulnar border of the proximal thumb.
 Stress testing of the first metacarpophalangeal joint should be performed while the joint is in 30 degrees of flexion and the thumb is held in full extension. The patient may not be able to tolerate this part of the examination because of pain, and it can consequently be deferred until specialist follow-up.
Stress testing of the first metacarpophalangeal joint should be performed while the joint is in 30 degrees of flexion and the thumb is held in full extension. The patient may not be able to tolerate this part of the examination because of pain, and it can consequently be deferred until specialist follow-up.
 A complete ulnar collateral ligament (UCL) tear induces the appearance of a palpable mass in the ulnar aspect of the joint and instability to radial stress, reaching an angle of 30 degrees or higher when compared with the contralateral thumb.
A complete ulnar collateral ligament (UCL) tear induces the appearance of a palpable mass in the ulnar aspect of the joint and instability to radial stress, reaching an angle of 30 degrees or higher when compared with the contralateral thumb.
 Obtain radiographs, which may be negative or show a small avulsion fracture of the proximal phalanx at the insertion of the ulnar collateral ligament.
Obtain radiographs, which may be negative or show a small avulsion fracture of the proximal phalanx at the insertion of the ulnar collateral ligament.
 Treat with ice, elevation, rest, acetaminophen, or anti-inflammatory medications, for comfort.
Treat with ice, elevation, rest, acetaminophen, or anti-inflammatory medications, for comfort.
 A soft dressing with an immobilizing elastic bandage that incorporates the thumb may be adequate for sprains or mild partial tears.
A soft dressing with an immobilizing elastic bandage that incorporates the thumb may be adequate for sprains or mild partial tears.
 A thumb spica provides support to the wrist and thumb for the more significant ligament injuries. The patient’s thumb should be positioned in a comfortable neutral position, and a 2-inch padded splint, which can be molded around the thumb, should be applied (Figures 135-2 and 135-3).
A thumb spica provides support to the wrist and thumb for the more significant ligament injuries. The patient’s thumb should be positioned in a comfortable neutral position, and a 2-inch padded splint, which can be molded around the thumb, should be applied (Figures 135-2 and 135-3).
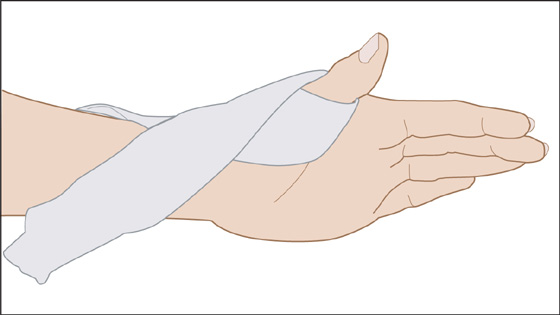
Figure 135-2 Apply the splint in a cross fashion around the dorsum of the thumb incorporating the MCP joint. (Adapted from Hart RG, Kleinert HE, Lyons K: A modified thumb spica splint for thumb injuries in the ED. Am J Emerg Med 23:777-781, 2005.)
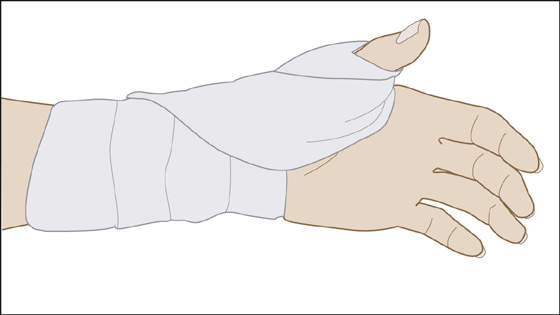
Figure 135-3 After the thumb and wrist have been positioned comfortably, an elastic bandage can be applied. (Adapted from Hart RG, Kleinert HE, Lyons K: A modified thumb spica splint for thumb injuries in the ED. Am J Emerg Med 23:777-781, 2005.)
 Explain to the patient with a significant partial or a complete ligament tear that this particular injury may not heal with closed immobilization and sometimes requires operative repair. Complete tears that require surgical repair should be done 1 to 3 weeks after the injury.
Explain to the patient with a significant partial or a complete ligament tear that this particular injury may not heal with closed immobilization and sometimes requires operative repair. Complete tears that require surgical repair should be done 1 to 3 weeks after the injury.
 Arrange for reexamination and hand specialist or orthopedic referral after a few days, when the swelling has decreased.
Arrange for reexamination and hand specialist or orthopedic referral after a few days, when the swelling has decreased.
This same lesion was once produced by the repeated breaking of the necks of rabbits by Scottish hunters or gamekeepers—hence the name.
Injury to the UCL is a frequent lesion that occurs from a radially directed force on the abducted thumb. Rupture of the UCL may be total or partial and usually takes place at its phalangeal point of insertion. The rupture of the thumb UCL can be an isolated lesion or can occur in combination with other joint structures, such as the volar plate or dorsal capsule. When the ligament ruptures distally, retraction may be associated with the interposition of the adductor pollicis aponeurosis, with the torn UCL lying superficially at the proximal end of the aponeurosis. This injury, called a Stener lesion, can inhibit proper healing of the ligament. MRI can detect the torn ligament and reveal displacement, if present.
Nondisplaced UCL tears are usually treated conservatively. Surgical intervention is usually reserved for Stener lesions and complete undisplaced tears with laterolateral instability, because conservative treatment leads to chronic instability and arthrosis.
Avulsion fractures involving more than 20% of the articular surface may require pinning.

Full access? Get Clinical Tree


