CHAPTER 52
Trigger Point Injections
INDICATIONS
• Trigger point injections (TIs) are commonly used as a treatment option in patients with acute and chronic muscle pains associated with an irritable, tight or taut muscle band, or palpable knot within a muscle that can radiate pain into specific distant or referred pattern called the “reference pain zone.”
• Pain can be present at rest, with poor posture or with overuse activity increasing the stress of a particular muscle or muscles involved. It can be the primary pathology in a muscle injury due to trauma or accident (ie, Whiplash) or secondary to underlying problem such as disk herniations, facet joint pain or bone, nerve injury.
• Trigger points are commonly present in patients with myofascial pain syndrome. This is a chronic regional localized pain syndrome with several trigger points limited to a particular area of the body. The neck and upper and lower back are commonly involved areas.
• In the cervical and thoracic area common muscles involved include the paraspinal muscles: splenius capitis, sternocleidomastoid, trapezius, levator scapulae, rhomboids, latissimus dorsi, serratus posterior inferior.
• In the lumbar spine, it commonly involves the quadratus lumborum (both deep and superficial), psoas, internal oblique, iliocostalis, longissimus or deep semispinalis, and multifidus.
• Trigger points in the shoulder rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, and teres minor) and shoulder blade area such as serratus posterior superior, latissimus dorsi, teres major, coracobrachialis, serratus anterior can present with referred pain patterns that can mimic or be confused with nerve root or radicular distribution.
• Similarly, trigger points in the gluteus medius, minimus, and piriformis muscles can refer down the posterior lateral thigh and be confused with sciatica.
• Trigger points are not to be confused with tender points commonly present in patients with fibromyalgia in which pressure in the tender points cause pain but no distant reference zone.
PHYSICAL EXAMINATION
• Physical examination findings include a knot, tight or taut muscle band.
• Associated with muscle spasm, irritable muscle with positive “jump sign,” histamine reaction.
• Painful on resistance to movement as during manual muscle strength testing.
• Referred pain in a “reference pain zone.”
• And at times, muscle twitch presents with pressure or when needle is inserted in the muscle.
• A pressure algometer can be use to quantify abnormal pressure pain sensitivity over trigger points and to identify the most painful trigger points for injection.
• Increase of pressure pain threshold by 2 to 3 kg immediately after TPI indicates that the injection was effective.
• A trigger point is called active when the referred pain is present spontaneously and latent when the referred pain is elicit with pressure or muscle activity.
TYPICAL REFERRED PATTERNS
Goal of Trigger Point Injections
The primary goal of the trigger point injections is to inactivate the trigger points by destroying and anesthetizing the primary area of pain through needling and infiltration with injectable solution.
Equipment and Supplies (Figure 52-1)

Figure 52-1. Picture of the tray.
• Sterile gloves
• Betadine and/or alcohol solution or other antiseptic solution
• 1% lidocaine (usual anesthetic of choice) and/or 0.25% or 0.5% marcaine, +/– steroid
• 10-cc syringe
• 25-gauge 1.5-in needle for superficial muscles and 25-gauge 3.5-in needle for deeper muscles
Procedure
• Patient is positioned to optimize access to the affected muscle, ie, prone for posterior muscles and supine for anterior muscles (ie, sternocleidomastoid, pectoralis, abdominals, biceps, quadriceps); see Figure 52-2.

Figure 52-2. Patient positioning.
• Ensure comfortable breathing and body positioning by using a head rest, pillows under the chest or abdomen and pillow under the legs.
• In the neck and upper back, the sitting position can be used but prone position preferably due to potential vasovagal reaction.
• Identify and mark with sterile marker trigger point locations (Figure 52-3) and more painful area within the trigger point.
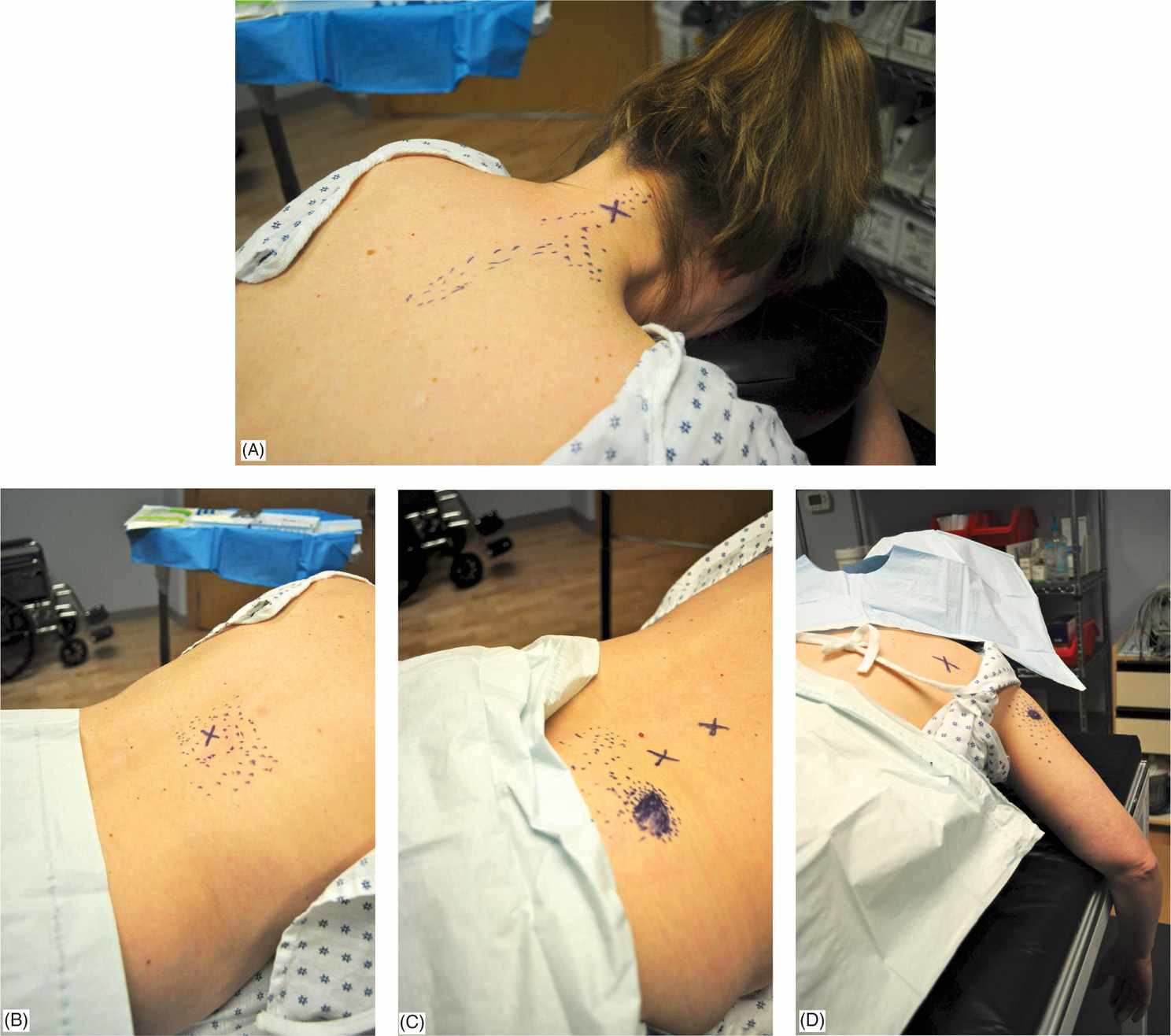
Figure 52-3. (A–D) Examples of common trigger points with reference zone marked.
• Clean area to be injected with antiseptic solution of choice. Spray the area to be injected (the taut band) with ethyl chloride to slight frost point.
• Utilizing a 25-gauge 1.5 in needle for deeper muscles insert the needle into the muscle slowly (Figure 52-4).

Figure 52-4. Example of injection.
• Give yourself time to feel the needle advancing through skin, subcutaneous tissue, normal muscle, and contacting the trigger point or fibrotic tissue and find trigger point (ideally muscle twitch present) through needling technique moving the needle back and forth through the trigger point.
• After negative aspiration of blood, fluid, or air inject a total of 3 mL of solution per trigger point location.
• Following the injection ethyl chloride stretch and spray can be of help.
• Also acupuncture needle placement and left to disperse for 10 to 15 minutes or gentle massage in the area injected.
POSTINJECTION INSTRUCTIONS
• No heavy activity or exercise except for gentle stretching on the day of the procedure and apply heat to the injection site for 15 minutes with a barrier between skin and heat 2 to 3 times a day.
• Postinjection stretching and stabilization program and instructions/education on proper posture, spine mechanics and extremities ergonomics.
POTENTIAL COMPLICATIONS
• Infection, bleeding, reaction to the medications used (keep total lidocaine used to no >20 mL), vasovagal reaction, injection site pain (temporary flare up) or more serious complications such as pneumothorax.
• If using steroid be aware of potential skin depigmentation changes and possible skin atrophy particularly on thin patients and with superficial muscles.
CLINICAL PEARLS
• While among the safest procedures, they are not without risk.
• Risk of pneumothorax when performing procedure either posterior or anterior over the lung margins (ie, cervical upper thoracic and anterior injections).
• When using a 25-gauge needle it can deflect without the operator being aware of what is happening at the tip of the needle.
• Patients may cough at the time of the procedure or have a strange taste in the mouth. Certainly shortness of breath can occur.
• Other concerns include injection of local anesthetic into superficial arteries in the neck.
• Vertebral and carotid injections with even low volume of local anesthetics can cause seizures and death.
• As with all interventional procedures, it is important to use caution and carefully weigh the risks and benefits of the proposed procedures.





Full access? Get Clinical Tree


