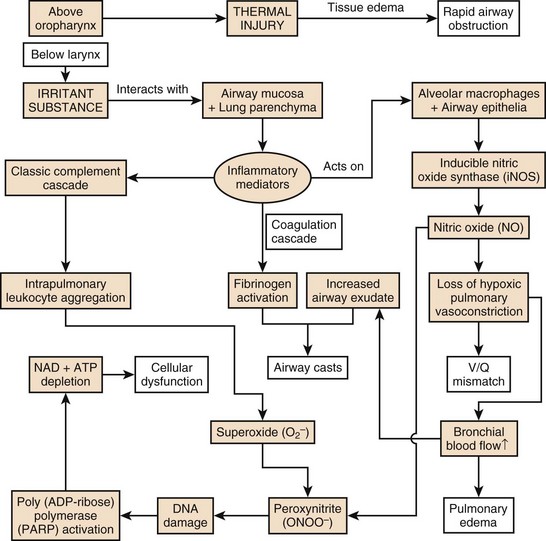
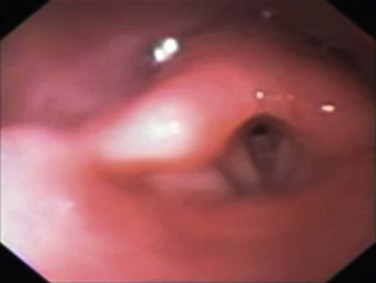
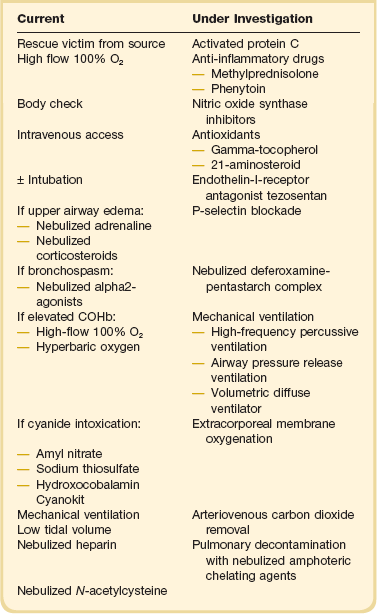
48 Chronic exposure to inhalation of atmospheric pollution may damage the lung over decades, predisposing to infection, pulmonary fibrosis, or cancer.1 The World Health Organization estimates that more than a billion people, mainly in developing countries, develop airway and pulmonary inflammation resulting from inhaled smoke from indoor cooking fires, forest fires, and burning of crops.2 In the industrial world, chronic inhalation injury may be due to cigarette smoking or occupational exposure (e.g., asbestos). This aspect of inhalation injury will not be further discussed in this textbook, and readers are referred to other resources.3 Acute smoke inhalation results in approximately 23,000 injuries and 5000 to 10,000 deaths per year in the United States alone. Among industrial countries, the United States has one of the highest incidences of smoke inhalation injuries.4 The ensuing pulmonary derangements, which follow burn and smoke inhalation injuries, are major contributors to morbidity and mortality in fire victims. The pathophysiology of the injury is multifaceted and induces distant organ dysfunction (Fig. 48.1). The consequences of the profound airway inflammation are heightened by pulmonary shunting and augmented microvascular pressure gradient, resulting in hypoxemic respiratory failure.5 Although survival from burn injury continues to improve, this is not mirrored in inhalation management. The acute lung injury caused by smoke inhalation and pneumonia has a major negative impact on mortality figures in patients with burn injuries. Inhalation injury alone increases mortality in burn victims by approximately 20% and pneumonia increases the rate by approximately 40%, with a maximal increase of approximately 60% when both are present.6 The mainstay of treatment of the smoke inhalation sufferer remains optimal respiratory support with airway toilet, adequate fluid resuscitation, early and aggressive surgical interventions, and precise antimicrobial interventions. Continued research into this systemic process is needed to stop smoke inhalation injury being the major cause of death in fire victims.7 Inhalation injuries, both of toxins and smoke, have been recorded in the history books for several thousand years and have been used with enmity from the outset. Thucydides records the Spartans burning pitch, naphtha, and sulfur to produce sulfur dioxide while attacking Athenian cities in 423 BC.8 The fifteenth century brought incendiary devices filled with sulfa and belladonna.9 The history of toxic gases other than smoke tends to run hand in hand with military conflict, and it wasn’t until the First World War that the increased usage sparked off once more, where at least 14 different toxic respiratory agents were used. The years 1914-1915 marked the modern nascence of inhalation warfare when France released chloroacetone and Germany released thousands of liters of chlorine gas in Belgium, at Ypres. More than 1 million casualties were attributed to the use of chemical agents during that war, with sulfur gas being anointed as the “king of battle gases.”10 The 1925 Geneva Protocol signed by many countries pledged never to use gas warfare again.9 Sadly, this has not been adhered to, with Italy being accused of using mustard gas against Abyssinia in Ethiopia. The Chinese suffered gas inhalation at the hands of the Japanese during the Second World War, and the Kurds were victim to similar agents during the attacks by Iraq through the 1980s.11 Sarin gas poisoning was used in Japan in the mid-1990s. In 1994 and 1995, inhaled biochemical weapons have been used for terrorism acts like the sarin gas attacks in Japan.12 Cyanide (CN) may be considered one of the most likely agents of chemical terrorism, as it is capable of causing mass incapacitation and casualties and can cause mass confusion, panic, and social disruption. In addition, cyanide possesses all attributes of an ideal terrorist weapon: it is plentiful, readily available, and easily obtainable because of its widespread use in industry and laboratories.13 Although military interest in biochemical warfare diminished following World War II, there was an understanding of the devastation possible with nuclear weapons; terrorist organizations understand the fear, panic, and collapse of infrastructure that could be realized through the release of such a substance in a busy city. It seems likely that there are many areas of the world where such agents are, or can be, manufactured in great quantities.9 Equally, smoke inhalation has a long record in history, with the first recording by Pliny in the first century AD. He described the execution of prisoners over greenwood smoke, and it seems he may have died through toxic smoke inhalation himself during the eruption of Vesuvius in 79 AD. More recently, two much more industrial occurrences highlighted the problems of smoke inhalation. The Cocoanut Grove fire of 1942 resulted in the deaths of 491 people who were trapped in a burning building. The number of patients who sustained burns was minimal, and it was then that the realization hit that smoke alone could kill as easily, if not more so, than cutaneous burns.14 More than 2000 burn/smoke casualties resulted after the chain of fires and explosions that rippled through refineries and factories in Texas City, Texas, in the 1940s.15 The understanding of smoke and carbon monoxide (CO) inhalation in enclosed spaces was further highlighted in the fire at the MGM Grand Hotel in Las Vegas in 1980 and the Stardust Nightclub fire in Dublin in 1981. Again, the small number of burn injuries was swamped by the deaths resulting from smoke and CO.16 Cyanide’s independent role became clear in the 1980s, particularly after the aircraft fire at Manchester International Airport, Manchester, UK, in 1985 where the majority (87%) of the 54 individuals who died had potentially lethal levels of cyanide in their blood, as opposed to only 21% of these victims having carboxyhemoglobin (COHb) levels exceeding 50%. This event highlighted that different combustants produce different inhalants, and depending on the environment, these may be more lethal than carbon monoxide, which had been regarded as the primary toxic threat.4 Hence, the determinants of inhalants are both environment and material being combusted. It is therefore a mixed toxicology following smoke inhalation. The terrorism attacks on September 11, 2001, on the World Trade Center in New York were associated with a high incidence of inhalation injuries. Among the 790 injured survivors, 49% suffered from inhalation injury caused by toxic compounds in the smoke and dust.17,18 Industrial catastrophes, biochemical warfare, and terrorism will continue to occur. This chapter’s aim is to help physicians diagnose and then manage patients with inhalation injuries. Smoke is a heterogeneous compound. Each fire produces different toxic features relating to the material combusted and the environment in which the fire occurs, specifically oxygen content. Hence, each patient suffering smoke inhalation may represent a new condition with a possibility of many different inhalants.19 The components of smoke that cause damage are as follows: • Particulates, deposited in the airways according to their size, with substances smaller than 1 µm in diameter able to reach the alveolar zone suspended in air. At that site, these chemically laden particles increase airway resistance and cause cell lysis and irritation while diminishing pulmonary surfactant production and efficacy.19 • Systemic toxins, such as carbon monoxide and cyanide, which adversely affect oxygen transport by erythrocytes and utilization by mitochondria.20 • Respiratory irritants are implicated in the high mortality rates. Water-soluble gases such as ammonia and hydrogen chloride react with water contained in mucous membranes and produce strong alkalis and acids, which elicit profound inflammatory reactions, which rapidly induce systemic changes via the dense alveolar-capillary interphase. Lipid-soluble irritants (e.g., oxides of nitrogen, phosgene, and aldehydes) exert their effects more slowly as they dissolve into the cellular membrane.21 Burns to the nasal and oropharyngeal mucosa are common in fire-exposed victims, but it is rare to encounter thermal injury below the vocal cords. This is because the oropharynx acts as an effective “heat sink,” with the thermal energy of the heated air dissipating into the cells they pass by, causing rapid cell injury, necrosis, and swelling of the upper airway (Fig. 48.2). This can result in upper airway obstruction, which can be fatal before the sequelae of pulmonary burn become apparent. Super-heated steam is an exception, where the oropharynx cannot absorb all the thermal energy, and hence airway burn occurs in this situation.22 Systemic toxins are products of incomplete combustion and include carbon monoxide and hydrogen cyanide. Carbon monoxide intoxication, together with heat incapacitation and a hypoxic environment, is the most common immediate cause of death from fire.20 Carbon monoxide is an odorless, colorless gas that binds to erythrocyte hemoglobin with about 250 times the affinity of oxygen. The resulting COHb molecule is unable to transport oxygen, thus impairing oxygen delivery to the tissue and shifting the oxygen-dissociation curve to the left.23 Furthermore, at the tissue level, carbon monoxide competes with, and inhibits, oxygen binding to the cytochrome oxidase system of enzymes, inhibiting the aerobic metabolism chain and thus incapacitating cellular respiration.21 Hence, CO paralyzes oxygen carriage in the blood and subsequent utilization in the tissue (see Table 48.2, presented later in the chapter). Thermal decomposition of nitrogen-containing polymers in oxygen-poor environments produces smoke containing hydrogen cyanide, inhibiting electron transport and cellular respiration.19 Table 48.2 Carboxyhemoglobin Concentration and Related Symptoms Although the inhaled gases as described earlier can cause significant and fatal alterations in physiology, the chief mediator of the pathophysiology of smoke inhalation is particulate matter. Carbonaceous particles (soot) impregnated with a multitude of toxins reach the alveolar level suspended in air.24 The chemicals associated with these particles vary depending on the products combusted but commonly include aldehydes from cellulose-based materials such as wood and paper; nitrogen oxides from fabric combustion; halogen acids and sulfur dioxide from rubber; ammonia from wool, silk, and polyurethane; and phosgene from polyvinyl chloride.22 Water-soluble compounds are readily soluble in airway mucus and interact freely with tissue at more proximal levels of the respiratory system. Less water-soluble compounds (such as phosgene) penetrate the airway mucosa deeply and may cause severe delayed damage through late interaction with distal airway tissues, up to 48 hours after exposure. This is an important consideration when treating patients who initially present with apparently mild clinical effects after smoke inhalation.22 Although thermal injury is mostly adsorbed in the upper airway, the other components of smoke—particulate materials, systemic toxins, and respiratory irritants—descend to the lung and trigger a cascade of events, resulting in pulmonary edema, bronchiolar obstruction, cell death, and ventilation/perfusion (V/Q) mismatch.19 Of paramount importance is the cascade of inflammatory mediators activated by the interaction of irritant substances with the airway mucosa and lung parenchyma. Intrapulmonary leukocyte aggregation following activation of the classic complement cascade releases even more chemokines and cytokines, leading to the production of free radicals of oxygen and nitrogen25 from nitric oxide synthase (NOS)–triggered nitric oxide (NO) and peroxynitrite (ONOO−) production. The vasodilation induced by NO rapidly increases bronchial blood flow and decreases the degree of the protective hypoxic pulmonary vasoconstriction in poorly ventilated areas of the lung, resulting in V/Q mismatch.26 This also intensifies the spread of irritants from the pulmonary to systemic circulation. NO also combines with superoxide (O2−) produced in large quantities by activated neutrophils to form ONOO−. This reactive nitrogen species leads to DNA damage and subsequent activation of poly (Adenosine diphosphate ribose [ADP-ribose]) polymerase, an important enzyme in DNA repair. This activation and subsequent action requires a large amount of chemical energy in the form of adenosine triphosphate (ATP) and Nicotinamide adenine dinucleotide (NAD), the depletion of which causes necrotic cell death of deprived energy-dependent tissues.25 The combination of these effects contributes to tissue injury and increased pulmonary vascular permeability, leading to decreased diffusion, edema, and V/Q mismatch. Furthermore, neutrophils are sequestered from the systemic circulation to the intrapulmonary compartment and are activated, and fibrinogen release by inflammatory mediators causes airway cast formation and widespread plugging. These casts obstruct a number of the smaller airways, and subsequent efforts to mechanically ventilate this inhomogeneous lung can induce ventilator-induced barotrauma as normal lung is overdistended, whereas other regions collapse, and atelectasise. The further tissue injury is heightened with biotrauma of ventilation, and the production of chemokines leads to a potent accumulation of damage.21 Much of the study of smoke inhalation injuries in animal models has focused on aspects of this pathophysiologic sequence. Attempts to manipulate and alter the chain of effects experimentally have reinforced these theories and suggested exciting treatment targets. Nevertheless, experimental treatments have yet to deliver specific therapeutic modalities that improve the course of smoke inhalation injury.5 The first priority at the injury scene is rescue of the victim from the source of fire to minimize the exposure time. This is usually the responsibility of firefighters.4 The patient must be assessed as a trauma patient and not merely as the victim of an isolated burn or smoke inhalation injury. Standard early management of severe trauma (EMST) protocols must be observed, including stabilization of the neck. Following the immediate administration of a high flow of O2 to reduce COHb levels, a primary survey must then follow to assess accompanying injuries such as burns or trauma with simultaneous estimation of the extent of smoke inhalation. In addition, it is important to determine whether the victim has been exposed to an explosion and to assess the possibility of blast injury to the lung. If possible, information about comorbidities should be obtained. Standard cardiopulmonary monitoring (electrocardiogram, pulse-oximetry, and noninvasive blood pressure) and intravenous access should be established.27 Carbon monoxide poisoning can result in an erroneously high SaO2 reading due to the light absorption of the classic “cherry red” hemoglobin in smoke inhalation. After these basic measures, the safety of the airway must be assessed. The risk of rapidly developing airway edema has to be taken into account even if no dyspnea is present, but it must be balanced by the real risks faced by endotracheal intubation itself in an unstable, potentially hypoxic patient with possible neck injuries. In the authors’ opinion, endotracheal intubation that is entirely prophylactic is ill advised. Nevertheless, the airway with early edema is likely to worsen, particularly if significant fluid resuscitation is required for burn injury, and hence repeated and thorough assessment of the airway is mandatory. Patients with evidence of stridor or heat and smoke inhalation injury combined with extensive face or neck burns may mandate early intubation. In the case of oral burn without inhalation injury, an airway secured early represents the safest approach. However, victims with smoke inhalation injury but no facial or neck burns can be carefully observed and can be intubated later, if necessary.28 The patient’s head should be elevated to 45 degrees to minimize facial and airway edema. In the field, fluid resuscitation can be minimized to reduce the risk of airway compromise if the necessary skills or equipment are not readily available for intubation. Nebulized adrenaline or corticosteroids may be used in the hope of minimizing upper airway edema, although there is no conclusive evidence for the efficacy of these treatment strategies.29 Bronchospasm is frequently observed, and the nebulized administration of bronchodilators, such as β2-agonists, will reduce this effect, while improving respiratory mechanics by decreasing airflow resistance and peak airway pressures in ventilated patients. This results in improved dynamic compliance. In addition, β2-agonists provide anti-inflammatory properties, represented by a decrease in inflammatory mediators such as histamine, leukotrienes, and TNF-α. Finally, β2-agonists are associated with improved airspace fluid clearance and stimulation of mucosal repair.30–32 After initial stabilization of the patient, information about the type of fire and combustible materials involved, whether the fire occurred in an enclosed space, and the estimated duration of exposure should be sought. In cases of presumed specific intoxication, appropriate therapies should begin.21 Diagnosis of such intoxications is impossible in the field, but a high degree of suspicion must be maintained if the combustion materials and enclosed space lead the treating practitioner to assume risk of CO or CN. All patients should be immediately administered 100% O2 from a high-flow facemask to reduce the CO binding to Hb. Specific therapies exist to treat the toxicity of carbon monoxide and cyanide, which aim to reduce the serum levels of these substances. Depending on the Glasgow Coma Scale, the severity of injury, and the symptoms, the patient’s condition may mandate intubation and mechanical ventilation with an FiO2 of 1. Patients with the possibility of cyanide intoxication require standard supportive care, which may be augmented with specific antidote therapy—the choice of which is the more efficacious remains controversial. Amyl nitrate and sodium thiosulfate are used to oxidize hemoglobin to methemoglobin, which preferentially binds cyanide. In contrast to these antidotes, hydroxycobalamin (vitamin B12a) actively binds CN by forming cyanocobalamin, which is directly excreted via the kidney. Because it does not produce methemoglobin, hydroxocobalamin is safe to use in the preclinical setting. Accordingly, it represents the active compound of the “Cyanokit,” which is used in the prehospital management of smoke inhalation injury in Europe with a reported reduction of mortality33 (Table 48.1). Clinical suspicion of inhalation injury of the upper airway is aroused by the presence of certain risk factors such as history of exposure to fire and smoke in an enclosed space or a period of unconsciousness at the accident scene, burns including the face and neck, singed facial or nasal hair, altered voice, dysphagia, oral or nasal soot deposits, or carbonaceous sputum. The most immediate threat from inhalation injury is upper airway obstruction due to edema (see Fig. 48.2). Early intubation is recommended when this complication threatens and the patient was not intubated on scene.34 However, exposure to smoke does not always lead to severe injury, and in the absence of overt evidence of respiratory distress or failure it may be difficult to identify patients who will experience progressive inflammation and ultimately require intubation of the trachea. When intubating in the field, optimal technique to secure a difficult airway is a contentious issue. Experienced operators may attempt to preserve spontaneous breathing, which allows patients to maintain their own reflexes even when intubation is not possible. Others may elect to perform a rapid sequence induction, which provides better intubating conditions but oblates all of the patient’s own airway reflexes. Attention should be given to gastric residuals during enteric feeding after admission to the burn intensive care unit. In addition, the development of sepsis can slow gastric emptying, which can result in retained fluids in the stomach and risk of aspiration.27 A patient with a compromised airway has evolved to maintain the airway at all costs. This primitive survival instinct is neutered if paralyzing agents or heavy sedation is administered and the safe airway can rapidly become unsalvageable. Intubation of a spontaneously breathing patient, while being more technically challenging, is safer, as the patient will keep breathing at all costs. In terms of anesthetic airway management, the most profound and clinically significant effect of burn injuries on drug response relates to muscle relaxants. Burn injuries influence responses to both succinylcholine and the nondepolarizing muscle relaxants. In burned patients, sensitization to the muscle relaxant effects of succinylcholine can produce exaggerated hyperkalemic responses severe enough to induce cardiac arrest, though this tends to occur 24 to 48 hours post injury, rather than immediately.35 However, recommendations regarding the safe use of succinylcholine after burn injury cannot be given. Various authors recommend avoidance of succinylcholine at intervals ranging from 24 hours to 21 days post burn injury,36 but it seems clear that the hyperkalemic response associated with burn does not occur in the first day and hence the drug can be used with standard precautions at this stage. An increase in the numbers of acetylcholine receptors and the proliferation of these receptors away from the neuromuscular junction have been suggested as common mechanisms explaining both reduced sensitivity to nondepolarizing relaxants and the exaggerated hyperkalemia that may follow succinylcholine administration in burned patients. Resistance is apparent by 7 days post injury and peaks by approximately 40 days. Sensitivity returns to normal after approximately 70 days. In contrast to other nondepolarizing neuromuscular blockers, mivacurium dosage requirements in pediatric patients appear to be unchanged by burn injury.37
Toxic Gas, Fume, and Smoke Inhalation
Introduction
Epidemiology
History
Pathogenesis of Inhalation Injury
Toxic Smoke Compounds
Heat
Systemic Toxins
COHb [in %]
Symptoms
<20
Slight headache and dilation of peripheral blood vessels
21-40
Severe headache and pulsating in temporal blood vessels, vertigo, dizziness, nausea and vomiting, circulatory collapse
41-60
Symptoms as above, syncope, tachycardia, hyperventilation, intermittent seizures, cyanosis, coma, shock, Cheyne-Stokes respiration
61-80
Coma, intermittent seizures, impaired heart and lung function, weak pulses, slow breathing, death within hours
>81
Death occurs within minutes
Airway Injury
Pulmonary Parenchymal Injury
Diagnostics and Treatment
Initial Prehospital Rescue
Airway Management

Full access? Get Clinical Tree


Toxic Gas, Fume, and Smoke Inhalation