Fig. 46.1
The Ebers Papyrus (c. 1550 BC) from Ancient Egypt (Source: http://commons.wikimedia.org/wiki/File:PEbers_c41.jpg). By Einsamer Schütze [GFDL (http://www.gnu.org/copyleft/fdl.html) or CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Claudius Galenus (better known as Galen of Pergamon) was a prominent Greek physician and a surgeon who furthered the understanding of wounds [2]. Significantly, he identified the importance of maintaining wound-site moisture to ensure successful closure of the wound.
In the twelfth century Moses Maimonides in his “Surgical Aphorisms” further identified the danger of skin “boils” and possible spread from these lesions, a precursor to the issue of infectious contamination and lateral spread. Further he identified the role of cauterization, heat, and corrosive agents as means of sterilizing a wound and preventing infectious spread [3].
All of these early observations and insight were amplified in the nineteenth century with the growth of the fields of microbiology and cellular pathology. See Fig. 46.2a–d. Finally, infection was recognized as being due to microorganism spread rather than a confluence of bad humors. Further, the role of inflammation, tissue ischemia, necrosis, and response to injury were revealed. These established the basis for a mechanistic understanding and approach to therapy. Unfortunately, however, the same insights into the germ theory of medicine also led to physicians and surgeons literally and figuratively “washing their hands” off the problem. This perception coupled with the rise of professional societies of nurses led to much of the day-to-day management of wounds being borne on the shoulders of nurses.
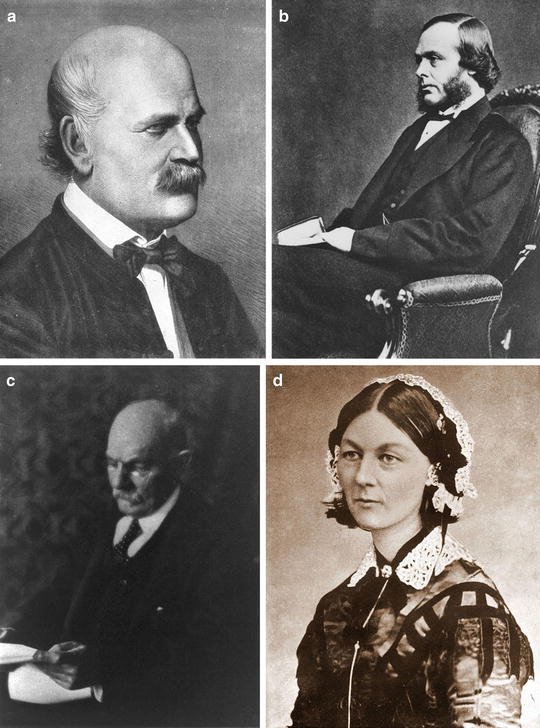
Fig. 46.2
(a–d) A brief timeline of wound healing. (a) Ignaz Philipp Semmelweis (July 1, 1818, to August 13, 1865) was a Hungarian physician now known as an early pioneer of antiseptic procedures (Ignaz Semmelweis 1860. Copper plate engraving by Jenő Doby. Source: http://upload.wikimedia.org/wikipedia/commons/f/f8/Ignaz_Semmelweis_1860.jpg. By Jenő Doby [Public domain], via Wikimedia Commons.); (b) Joseph Lister, 1st Baron Lister (April 5, 1827, to February 10, 1912). Known as Sir Joseph Lister. Between 1883 and 1897 was a British surgeon and a pioneer of antiseptic surgery (Joseph Lister, 1st Baron Lister, circa 1876: Source: http://commons.wikimedia.org/wiki/File%3AJoseph_Lister_c1867.jpg. Author unknown [Public domain], via Wikimedia Commons); (c) William Stewart Halsted (September 23, 1852 to September 7, 1922) was an American surgeon who emphasized strict aseptic technique during surgical procedures (William Stewart Halsted, 1852–1922, half-length portrait. Source: http://commons.wikimedia.org/wiki/File%3AWilliamHalsted.jpg. Author unknown [Public domain], via Wikimedia Commons); (d) Florence Nightingale (12 May 1820 to 13 August 1910) was a celebrated English social reformer and statistician, and the founder of modern nursing (Florence Nightingale from Care de Visite, circa 1850s. Source: http://commons.wikimedia.org/wiki/File%3AFlorence_Nightingale_CDV_by_H_Lenthall.jpg. By H. Lenthall, London [Public domain], via Wikimedia Commons)
1850s–1995: Poultices, Plasters, and Polymers
Much of the efforts over this period of time were focused on serving the dressing needs of nurses. Dressings were designed at best to manage drainage and to reduce pain during dressing changes. During World War I, in response to the needs of soldiers on the Western Front, Nobel Laureate Alex Carrel and chemist Henry Dakin screened more than 200 compounds and ultimately developed a wound-irrigating solution composed of sodium hypochlorite (0.45–0.5 %) in a buffered solution. This formulation, subsequently referred to as “Dakin’s solution,” provided excellent antimicrobial activity, combined with good irrigating properties without significant caustic, corrosive, or painful effects [4].
With the advent of synthetics and polymers in the 1950s, materials such as polyethylene, polypropylene, and polyvinyls provided constructs, in the form of gauzes and dressings, that further provided means to modulate the material properties of dressings. Some of these led to the first widely available foam/hydrocolloid-based dressings in the 1980s. More dressings such as these continued through the 1980s and into the 1990s until the next major advance: active healing technologies.
From Analog to Digital: Dressings and Supportive Care Meet Pharmaceuticals and Devices (Fig. 46.3)
Fig. 46.3
Wound care technologies
In 1995, the first pharmaceutical requiring a prescription, Becaplermin (Regranex®, Smith+Nephew, Largo, FL), became available in North America. This single event led to rapid reeducation of the broader community of physicians and surgeons into chronic tissue repair and wound healing. Followed rapidly by negative pressure wound therapy (NPWT), and cell-based allografts (Dermagraft (Advanced Biohealing Ltd, La Jolla, CA), Apligraf® (Organogenesis, Inc., Canton, MA)), there emerged choices for physicians, surgeons, and nurses in therapies beyond previously available gauzes and intraoperative management/wound packing. In essence, technology further facilitated team building. This led to a dichotomy of sorts. The first of these two historical categories includes dressings and supportive care, which can now serve to manage drainage, reduce pain and frequency of dressing changes, and possibly also reduce/modulate bacterial load. The second, pharmaceuticals and devices, serves to promote angiogenesis and regeneration.
Significance of Wound Healing
Wound healing is a process via which injured tissue attempts to repair itself after injury. It is an intricate process in which the body tries to wall off and eliminate infection, clear damaged and necrotic tissue, and rebuild damaged or lost tissue elements. The classic model of wound healing is divided into four sequential yet overlapping phases. These include (a) hemostasis, (b) inflammation, (c) proliferation, and (d) remodeling [5]. Under ideal conditions these phases progress synchronously. Certain pathophysiologic and metabolic conditions can alter this course of events so that healing is impaired or delayed, resulting in chronicity, i.e., chronic wounding [5, 6].
Perhaps the most common chronic wound in the developed and the developing world comes as a result of or concomitant with diabetes mellitus. According to the World health Organization, the epidemic of diabetes is affecting 285 million people (6.4 %) around the globe, and is expected to affect over 400 million adults by 2030 [7, 8]. A major cause of hospitalization and amputation among persons with diabetes is foot ulceration. It is estimated that one in four persons with diabetes in the USA will get foot ulcers at some point in their lifetimes [9]. As such, diabetic foot ulcer treatment is consuming nearly 25 % of overall cost of diabetes care, totaling around $43.5 billion [10]. Additionally, diabetes associated with ulceration increases the crude mortality rate from 6.7 to 27 % and shortens life expectancy by 3 years, relative to the average life expectancy for diabetic patients [11].
Additionally, as the world population is aging and becoming more sedentary, with an increased dependence on computers and automated manufacturing, low overall mobility results in venous obstruction or venous valvular dysfunction. This often precipitates chronic venous insufficiency which serves as yet an additional risk for foot ulceration. The annual prevalence of venous leg ulcers is estimated to be between 1.65 and 1.74 % in adults ≥65 years old, with anticipation of a substantial increase within the next several decades [12].
Wound Classification
In modern clinical practice, patients with foot ulcers present with a broad spectrum of underlying factors which contribute in the prognosis of the wound. Hence developing methods for stratification of wounds will help guide treatment decisions including the decision for amputation.
A recent advance was provided by the Society of Vascular Surgeons’ Wound Ischemia Foot Infection (WIFI) classification, which was introduced in late 2013 to fill in the gaps remaining with other clinical diagnostic schemes. This classification systematically addressed individual grading of wound severity, ischemia, and presence of foot infection. Each category is graded based on specific criteria, which offers an improved and objective assessment of diabetic foot complications, and its recoverability [13].
The Strategies for Treatment: “Vertical” and “Horizontal”
There are two main strategies for treatment of ulcers, the “vertical strategy” or the “horizontal horizontal.” In the vertical, the focus is aimed at trying to resolve the issue of the depth of the wound—either by filling the gap with living cells or approximating the edges using negative pressure. In the horizontal plan, the emphasis is aimed at trying to re-epithelialize the area using different techniques such as growth factors, negative pressure, stem cells, or amniotic membrane derivatives.
Modern Cell-Based Matrices: Three Examples
Grafix® (Osiris Therapeutics, Columbia, MD)
This is an example of a three-dimensional cellular matrix, designed to be directly applied to acute and chronic wounds—resulting from either burns or complications of the diabetic foot. It is a processed form of human placental membrane. With flexibility, this conforming membrane provides an excellent source of living mesenchymal stem cells (MSCs) and growth factors to the wound bed. The manufacturing process maintains the integrity of the extracellular matrix, the viability of the neonatal MSCs, and the active growth factors.
A clinical trial [14] to evaluate the safety and efficacy of Grafix for treatment of chronic foot ulcers was conducted. The trial included diabetic (both types) participants with foot ulcers which presented between 4 and 52 weeks, located around the malleoli aspects, varying in size from 1 to 15 cm2, and age range from 18 to 80. The study protocol excluded patients with HbA1c above 12 %, active infection, osteomyelitis, cellulitis, or muscle, tendon, or joint capsule infections. Additional criteria were used to omit participants with circulatory insufficiency, which was determined using the ankle brachial index (ABI), toe brachial index (TBI), or Doppler. Participants with wound healing rates of 30 % or more during the screening period were also disqualified.
One hundred and thirty-nine patients were recruited, of which 42 were disqualified for matching the exclusion criteria. The remaining 97 were divided into two arms, 50 who received Grafix, with 47 receiving the standard wound therapy. No significant differences were observed in the baseline characteristics between the two arms. The Grafix arm revealed significant efficacy for primary and secondary endpoints when compared with the standard arm.
Thirty-one participants (62 %) of the Grafix group achieved complete wound closure, with significantly (p = 0.019) faster median time (42 days) and probability (67.1 %) of closure, compared to ten in the standard wound therapy (21.3 %), with median time of 69.5 days and probability of 27.1 %. Grafix patients also required fewer study visits (i.e., applications) to achieve closure compared with patients in the control arm. The wound recurrence in the Grafix group, after complete closure, was 12.1 % less than the control arm.
Related posts:
 End Points of Resuscitation
End Points of Resuscitation
 Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
 The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
 Artificial Limbs for Upper Extremity Amputation
Artificial Limbs for Upper Extremity Amputation
 Use of Biologic Grafts in Surgery
Use of Biologic Grafts in Surgery
 Brain Cancer: The New Frontiers
Brain Cancer: The New Frontiers

Full access? Get Clinical Tree



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}