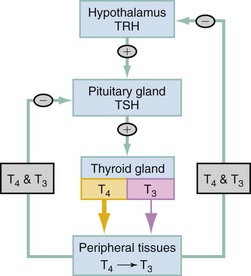
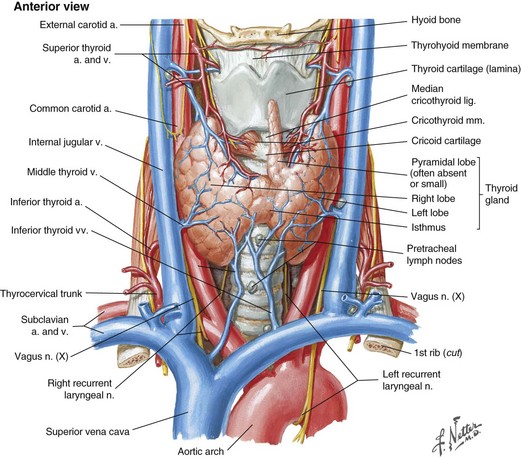
Chapter 128 Recent work has estimated the incidence of thyrotoxicosis at 80/100,000 per year in women and 8/100,000 per year in men.1 A population-based study in the United Kingdom demonstrated an incidence of 0.9/100,000 in children younger than 15 years. Most cases of thyrotoxicosis (>80%) are due to autoimmune disease.2 The prevalence of hyperthyroidism is five to ten times less than that of hypothyroidism. The myriad causes of thyrotoxicosis are listed in Box 128-1. Graves’ disease (diffuse toxic goiter) accounts for approximately 80% of all cases. Toxic multinodular goiter occurs most frequently in areas of iodine deficiency. It accounts for approximately 15% of thyrotoxicosis cases. In the United States, the incidence of toxic multinodular goiter is much lower than the global rate. Toxic adenoma is the third major cause of hyperthyroidism, accounting for approximately 3 to 5% of cases. Other less common causes of hyperthyroidism include thyroiditis (traumatic, infectious, or from radiation), ectopic thyroid tissue (lingual thyroid), tumors (pituitary, thyroid), drug induced (lithium, amiodarone), and exogenous thyroid hormone (from therapy or surreptitious consumption of thyroid hormone).3,4 The normal adult thyroid gland is a highly vascular organ overlying the anterior trachea. Its structure is bilobar with a median isthmus and total weight ranging from 10 to 30 g (Fig. 128-1). It receives its blood supply at a rate of 80 to 120 mL/min from the inferior and superior thyroid arteries, which are direct branches of the subclavian and external carotid arteries, respectively. The thyroid’s function is to secrete two iodinated hormones: triiodothyronine (T3) and thyroxine (T4). Only about 20% of circulating T3 is directly secreted by the thyroid; the remainder is produced by peripheral conversion of T4 to the more biologically active T3. This process occurs predominantly in the liver and in skeletal muscle. The thyroid is the only endocrine gland that stores large quantities of hormone, with enough for about 100 days’ supply. Figure 128-1 Anatomy of the thyroid gland and related structures. (Netter illustration from www.netterimages.com. Copyright Elsevier Inc. All rights reserved.) Regulation of hormone production is through a negative feedback loop involving the hypothalamic-pituitary-thyroid axis (Fig. 128-2). As the serum levels of T4 and T3 fall, the hypothalamus releases the tripeptide thyrotropin-releasing hormone (TRH), which in turn stimulates the anterior pituitary gland’s release of the polypeptide thyroid-stimulating hormone (TSH) from its thyrotroph cells. TSH then binds to epithelial cells on the thyroid gland, stimulating follicular cells to synthesize and secrete the thyroid hormones T4 and T3. TRH release may also result from exercise, stress, malnutrition, hypoglycemia, and sleep. The function of thyroid hormone is to influence the metabolism of cells by increasing their basal metabolic rate. It has a role in protein synthesis and function together with other hormones necessary for normal growth and development, such as human growth hormone and insulin. Graves’ Disease.: In the United States, Graves’ disease is the most common form of hyperthyroidism. In this autoimmune disorder, autoantibodies are formed to the TSH receptor, where they bind and stimulate the receptors. The overstimulated gland enlarges and increases thyroid hormone production and release. The triad of goiter, exophthalmos, and pretibial myxedema is diagnostic of Graves’ disease. The disease predominantly affects women and those with a family history of hyperthyroidism; it typically occurs between the ages of 20 and 40 years. Toxic Multinodular Goiter.: Toxic multinodular goiter is the second leading cause of hyperthyroidism in the United States. It is characterized by multiple autonomously functioning nodules developing in women older than 50 years. It is rare in youth, except in those with preexisting nontoxic multinodular goiters or living in iodine-deficient regions, such as Central America, South America, the Himalayas, eastern Europe, and central Africa. The hyperthyroidism in toxic multinodular goiter is milder than Graves’ disease and is gradual in onset, but acute presentations can occur when iodine replacement is given to an iodine-deficient individual. Graves’ disease typically is manifested in the sixth decade of life; cardiovascular manifestations like atrial fibrillation and heart failure predominate, whereas tremors and hypermetabolic features are less pronounced.5 Muscle wasting and weakness are common, and the patient is often described as apathetic. Obstruction of the airway is a concern as multinodular goiters often extend retrosternally. Toxic Adenoma.: A toxic adenoma is commonly referred to as a hot nodule. This single hyperfunctioning nodule typically affects the same population as toxic multinodular goiter does, but it occurs less commonly. Thyroiditis.: Any inflammatory process that results in thyroid gland inflammation can lead to thyroiditis. The inciting process may be autoimmune, drug induced, infectious, or traumatic. Inflammation leads to follicular cell breakdown, with resultant release of preformed thyroid hormone, causing acute thyrotoxicosis. The most common form of thyroiditis in the United States is Hashimoto’s thyroiditis, an autoimmune disorder characterized by the presence of thyroid antibodies and lymphocytic infiltration of the thyroid gland. Typically, patients present with a painless goiter and hypothyroidism, but some have transient thyrotoxicosis (hashitoxicosis) that may last for a few months. Postpartum and Sporadic Thyroiditis.: Other autoimmune disorders of the thyroid include postpartum thyroiditis and sporadic thyroiditis. Referred to as painless, or silent, thyroiditis, they are typified by a small nontender goiter and mild symptoms. It is estimated that 5 to 10% of women have postpartum thyroiditis. The diagnostic triad consists of the lack of previous history of thyroid disorder, an abnormal TSH concentration during the first postpartum year, and the absence of TSH receptor antibodies (Graves’) or a toxic nodule. Classically, these patients present with thyrotoxicosis 6 weeks to 6 months postpartum, followed by a hypothyroid state lasting up to 6 months; a euthyroid state returns by the end of the first postpartum year. However, the majority of patients present with either hyperthyroidism alone or lone hypothyroidism.6 The recurrence rate in subsequent pregnancy is estimated at 69%, and some women have permanent hypothyroidism. Sporadic thyroiditis is indistinguishable from postpartum thyroiditis except that it is unrelated to pregnancy. It may account for up to 1% of thyrotoxicosis, and most patients recover; 20% have hypothyroidism.7 Subacute Thyroiditis.: Subacute thyroiditis (de Quervain’s thyroiditis) is thought to be caused by a viral infection of the thyroid, often appearing after an upper respiratory infection. However, a study was unable to detect viral titers in 852 patients with subacute thyroiditis.8 It is manifested with a typical viral syndrome prodrome (fatigue, myalgias, and pharyngitis), followed by fever and severe anterior neck pain. Pain may radiate to the jaw, ears, or occipital area. The thyroid is exquisitely tender, and pain can occur with head movement or swallowing. During the acute painful phase, a minority of patients have symptoms of hyperthyroidism (diaphoresis, palpitations, and tremor) lasting several weeks. Subacute thyroiditis may account for 2% of thyrotoxic patients; it occurs in the fourth and fifth decades of life and is more common in women than in men. Suppurative Thyroiditis.: Suppurative thyroiditis is a rare but potentially life-threatening infection of the thyroid. Patients present with fever and anterior neck pain, neck swelling, induration, and erythema as well as dysphonia and dysphagia. Infectious causes are overwhelmingly bacterial (aerobic and anaerobic) and very rarely parasitic, mycobacterial, or fungal.9 Most patients have preexisting thyroid disease and are immunocompromised (AIDS). Drug-Induced Thyroiditis.: Amiodarone contains a high amount of iodine (37%, about 400 times the daily requirement) and as a result has a significant effect on thyroid function. It is estimated that between 5 and 20% of patients treated with amiodarone have thyrotoxicosis (higher in areas of iodine deficiency). Two proposed mechanisms have been described: an iodine-induced hyperthyroidism and a drug-induced destructive thyroiditis.10 It is thought that the iodine load may unmask hyperthyroidism in patients with multinodular goiter and subclinical Graves’ disease. More commonly, the cytotoxic effects of amiodarone destroy thyroid cells, resulting in a release of preformed hormone. An exacerbation of the tachyarrhythmia for which the patient is being treated or heart failure is the typical presentation of a patient with thyrotoxicosis related to amiodarone. Other drugs that may induce thyroiditis include interferon, interleukin-2, granulocyte-macrophage colony-stimulating factor, and lithium. Mechanisms vary, but lithium reportedly induces sporadic thyroiditis by direct toxic effects. Factitious Thyroiditis.: Thyrotoxicosis factitia results from ingestion of thyroid hormone. Although this can be iatrogenic or the result of patient medication error, the majority of cases stem from medical personnel with psychiatric illness who surreptitiously self-administer the medication. Cases of factitious thyrotoxicosis have been reported worldwide as a result of the consumption of bovine thyroid hormone in contaminated beef and from adulterated weight loss products.11 By contrast, inadvertent acute ingestions of thyroid hormone usually manifest only minor toxicity. Whereas the dose plays a role, the 7-day half-life of T4 allows physiologic compensation, such as the suppression of T4 to T3 conversion, inhibition of endogenous hormone production by negative feedback loops, and downregulation of thyroid hormone receptors. The variable presentation of thyrotoxicosis among patients creates a diagnostic challenge (Box 128-2). Hyperthyroidism induces a hypermetabolic state and increases beta-adrenergic activity. The resulting clinical manifestations range from vague constitutional symptoms to more organ-specific symptoms. Thyroid storm, the most severe manifestation of the disease, is a life-threatening state that requires prompt intervention. Variables that affect the severity of disease include age, disease duration, hormone levels and rate of rise, drug interactions, and stress of concurrent illness. Hyperthyroidism in elders often is manifested in subtle ways, mimicking symptoms of aging or masquerading as diseases of the cardiovascular, gastrointestinal, or nervous system.12 Gradual or long-standing thyrotoxicosis can go unnoticed by the patient, or symptoms may be attributed to other causes like emotional stress, dieting, or physical deconditioning. The clinical manifestations do not necessarily correlate with the degree of biochemical abnormality. Palpitations, dyspnea on exertion, and reduced exercise tolerance are common cardiopulmonary complaints. Elders are more prone to cardiac manifestations and often present with new-onset angina, atrial fibrillation, or congestive heart failure as the only manifestations of thyroid disease.13 Superior vena cava syndrome and dyspnea can occur as a result of compression of vascular and tracheal structures by an enlarged thyroid gland. Graves’ ophthalmopathy commonly causes eyelid retraction, lid lag, proptosis, and staring eyes. Although these symptoms were previously thought to occur only with Graves’ disease, one author suggests that they are present in thyrotoxicosis in the absence of an autoimmune phenomenon, in children and adolescents.14 Graves’ ophthalmopathy is also associated with restrictive extraocular myopathy, exophthalmos, and, less commonly, optic nerve dysfunction.15 Patients often complain of irritation and excessive tearing as early symptoms; diplopia, retrobulbar discomfort, blurring of vision, and foreign body sensation occur late in the disease. Physical examination of the thyrotoxic patient will reveal distinct symptoms that depend on the age of the patient (Box 128-3).16 Younger patients often appear anxious and fidgety, with a fine tremor of the hands and tongue. Dermatologic changes vary by area of the body. The skin feels warm, smooth, and velvety, especially over the elbows; the face is rosy and blushes readily, and the patient’s hands may reveal palmar erythema. Onycholysis (Plummer’s nails) may be present and shows separation of the distal portion of the nail from the nail bed. Scalp hair is fine and brittle, and diffuse alopecia may occur. In Graves’ disease, about 5% of patients have pretibial myxedema, in which mucopolysaccharide infiltration of the dermis yields marked thickening of the pretibial skin. These lesions are painless, raised nodules and plaques that become confluent over the pretibial area and dorsum of the feet. Hyperpigmentation and induration are present, but pitting is absent, and pretibial myxedema is almost always associated with Graves’ ophthalmopathy.17 Of the cardiac manifestations, tachycardia is by far the most common finding and is often accompanied by a systolic flow murmur. Other findings include a widened pulse pressure, bounding peripheral pulses, and rarely a friction rub heard along the left sternal border (Means-Lerman scratch). Whereas atrial fibrillation is more common in elders, with a prevalence of 15% in patients older than 70 years, it can be seen at any age, with an overall prevalence of 2%.13 Patients with subclinical hyperthyroidism have an increase in the prevalence of atrial fibrillation compared with the total population. Dilated cardiomyopathy may develop as a complication of tachycardia and high cardiac output state. Primary pulmonary hypertension, sometimes associated with tricuspid regurgitation and right-sided heart failure, may also be seen. Increased activity at the sympathetic innervation of the eyelids leads to widening of the palpebral fissures, resulting in the characteristic stare of thyrotoxicosis. Similarly, this also leads to lid lag, noted when the patient looks slowly downward and the lid lags behind the globe. Proptosis of the globe results from mucopolysaccharide infiltration and inflammation of the ocular muscles and soft tissue, leading to exophthalmos. This finding is thought to be unique to Graves’ disease and affects about 50% of patients. Early in Graves’ ophthalmopathy, conjunctival injection, periorbital edema, and chemosis may be seen. As the disease progresses, patients may experience restriction of upward gaze from infiltration of the inferior rectus muscle and visual loss from optic nerve involvement (compression by inflamed, enlarged orbital contents). Treatment of hyperthyroidism, especially with radioactive iodine, may paradoxically aggravate Graves’ eye disease.18 The majority of hyperthyroid patients have an enlarged thyroid gland. The size of the goiter depends on its etiology. Enlargement is common in patients with toxic multinodular goiter or Graves’ disease. However, many elders with Graves’ disease have a nonpalpable thyroid. In Graves’ disease, the thyroid gland is typically symmetrically enlarged (two to three times in size), soft, and smooth (without nodules). Variable enlargement occurs in toxic multinodular goiter, and multiple nodules may be present, resulting in an irregular surface. Retrosternal enlargement can occur, making detection difficult while causing the obstructive symptoms discussed earlier. Facial and neck vein engorgement can be elicited when arms are elevated above the head (Pemberton’s sign) (see Box 128-3). Thyroid storm is a rare, life-threatening form of severe thyrotoxicosis. Although it can occur as the result of unrecognized or undertreated thyrotoxicosis, more often it is an acute reaction to thyroid or nonthyroid surgery, trauma, infection, iodine load (contrast media or amiodarone), or parturition in patients with preexisting hyperthyroidism. Other precipitants include acute myocardial infarction, pulmonary embolism, and diabetic ketoacidosis (Box 128-4). It affects 1 to 2% of patients with hyperthyroidism and up to 10% of hospitalized thyrotoxic patients. Untreated, mortality approaches 100%, but prompt recognition and aggressive therapy have lowered mortality to 20 to 30%.19 Nearly all cases are related to Graves’ disease or occasionally toxic multinodular goiter and toxic adenoma; it rarely occurs in other causes of thyrotoxicosis. The typical clinical manifestations of hyperthyroidism are exaggerated in thyroid storm. Marked pyrexia to 104 to 106° F, tachycardia (often in excess of 140 beats/min), and altered mental status (agitation, delirium, or coma) are common features. These findings coupled with the clinical picture of a patient with hyperthyroidism, lid lag, stare, goiter, ophthalmopathy, and tremor should alert the clinician to the diagnosis. Cardiovascular collapse can result in congestive heart failure, hypotension, and cardiac arrhythmias. Hypotension can also result from volume depletion secondary to nausea, vomiting, and diarrhea. Abdominal pain is common; less commonly hepatic failure with cholestatic jaundice occurs, which is an indicator of a poor prognosis.20 Hyperthyroidism increases catecholamine receptor expression. As such, an exaggerated response is seen in the face of the adrenergic surge associated with physiologic stressors such as sepsis or trauma, yielding thyroid storm. The clinical picture that ensues should prompt the clinician to the diagnosis; however, no validated diagnostic system exists. Currently, the only tool available is a scoring system developed by Burch and Wartofsky, which can help distinguish between thyrotoxicosis, impending thyroid storm, and frank thyroid storm (Table 128-1).19 Table 128-1 Diagnostic Criteria for Thyroid Storm Modified from Burch HB, Wartofsky L: Life-threatening thyrotoxicosis: Thyroid storm. Endocrinol Metab Clin North Am 22:263-277, 1993. Reliable assays for serum TSH and free T4 have made the laboratory diagnosis of hyperthyroidism straightforward. Measurement of serum TSH is the single best test to assess thyroid function. A normal TSH level excludes hyperthyroidism and an elevated TSH level is generally diagnostic for hypothyroidism. In thyrotoxicosis, serum TSH concentration is depressed or undetectable (values <0.05 µU/mL in third-generation assays). Values above this threshold associated with hyperthyroidism are consistent with subclinical disease.21 Assessment of thyroid function during acute nonthyroidal illness is difficult, especially in critically ill patients. Severe systemic illness depresses TSH production, leading to low levels of TSH, free T3, and free T4. Once referred to as the euthyroid sick syndrome, it appears to be a transient form of central hypothyroidism.22 It is considered an adaptive response during systemic stress to prevent excessive catabolism. Patients taking dopamine, glucocorticoids, somatostatin, and octreotide may also have depressed TSH levels but not to the degree of patients with hyperthyroidism.23 Elevation of free T4 and free T3 in conjunction with TSH suppression is diagnostic of thyrotoxicosis. Subclinical hyperthyroidism is likely if TSH is suppressed and free T4 is normal. T3 toxicosis occurs in about 5% of patients with thyrotoxicosis, more commonly in toxic multinodular goiter. These patients have an elevated free T3 level and a normal free T4 level. When the reverse pattern is present (normal free T3 level and elevated free T4 level), the differential includes thyroiditis, exogenous levothyroxine ingestion, and hyperthyroidism in the elderly, often with suppressed T4 to T3 conversion due to comorbid illness (Table 128-2). Table 128-2 Thyroid Function Test Interpretation T3, triiodothyronine; T4, thyroxine; TSH, thyroid-stimulating hormone. The results of liver function tests are frequently abnormal in thyrotoxic patients. Mild increases in serum aspartate transaminase, alanine transaminase, lactate dehydrogenase, bilirubin, and alkaline phosphatase may be seen. The elevations in serum bilirubin do not typically result in clinical jaundice. Other frequent laboratory abnormalities include leukocytosis with a leftward shift, mild normocytic normochromic anemia, and low serum cholesterol levels.21 In thyroiditis, the diagnostic evaluation is more difficult. An exquisitely tender gland and an erythrocyte sedimentation rate above 100 mm/hr make the diagnosis of subacute thyroiditis likely. The other forms of thyroiditis lack these findings. Doppler ultrasound examination of the thyroid may be helpful in differentiating among the various causes of thyrotoxicosis. A hypervascular enlarged gland is seen in Graves’ disease, nodules in toxic multinodular goiter, and decreased Doppler flow in thyroiditis or factitious thyrotoxicosis.24 If factitious thyrotoxicosis is suspected, low thyroglobulin levels may confirm the diagnosis as these levels are elevated in all other forms of thyrotoxicosis. Furthermore, radioactive iodine uptake is depressed in thyroiditis and factitious thyrotoxicosis but increased in hyperthyroidism. Management of thyrotoxicosis is based on symptom severity. For those with mild symptoms, outpatient referral and management are appropriate. Patients with moderate to severe symptoms are best managed in the emergency department (ED) setting. Treatment is divided into supportive, symptomatic, and thyroid directed (Box 128-5). In addition, it is important to identify and to treat the precipitating cause of thyroid storm. BOX 128-5 Management of Thyroid Storm Propranolol 60-80 mg PO every 4 hr Metoprolol 50 mg PO every 6-12 hr If IV route is required: propranolol 0.5-1.0 mg IV slow push test dose, then repeat every 15 min to desired effect, then 1-2 mg every 3 hr Esmolol 250-500 µg/kg bolus, then 50-100 µg/kg/min infusion Strict contraindication to beta-blocker: reserpine 2.5-5 mg IM every 4 hr Inhibition of Thyroid Hormone Synthesis Propylthiouracil 600-1000 mg loading dose, then 300 mg every 6 hr (maximum daily dose, 1200 mg) Methimazole 20-30 mg initially, then 20-30 mg every 6 hr (maximum daily dose, 120 mg) (Preferred route: PO or NG. Alternative route: PR. Enema prepared by pharmacy. Same dose for all routes. No IV preparation is available, but IV methimazole can be prepared with the use of a Millipore filter and given 30 mg every 6 hr.) Lorazepam or diazepam as anxiolytic and to decrease central sympathetic outflow L-Carnitine (block entry of thyroid hormone into cells), 1 g PO every 12 hr Cholestyramine (blocks enterohepatic recirculation of thyroid hormone), 4 g PO every 6 hr
Thyroid and Adrenal Disorders
Hyperthyroidism
Background and Epidemiology
Principles of Disease
Pathophysiology
Clinical Features
Physical Signs
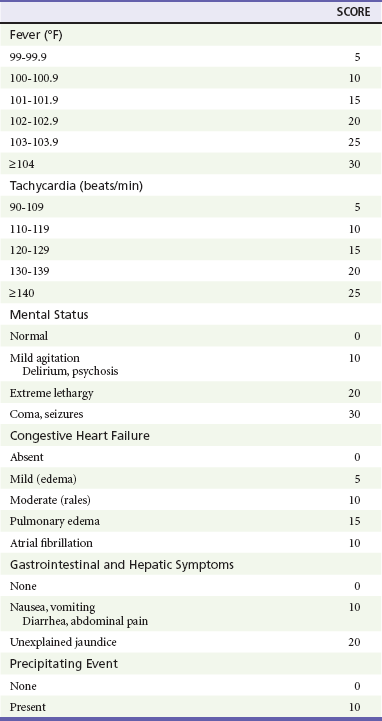
Thyroid Storm
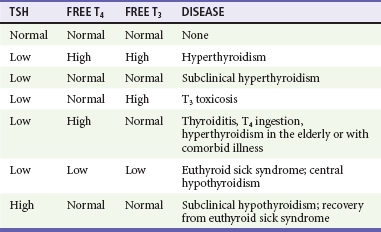
Diagnostic Strategies
Management

Full access? Get Clinical Tree


Thyroid and Adrenal Disorders