Thrombocytopenia in the Intensive Care Unit
Thrombocytopenia in the Intensive Care Unit
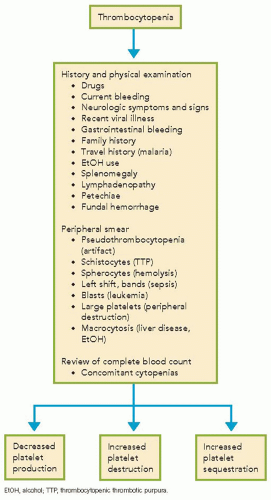
Thrombocytopenia is a very common occurrence in the intensive care unit (ICU), occurring in as many as 60% of patients. The normal platelet count ranges between 150,000 and 450,000/µL. In the ICU, it is important to recognize that the absolute platelet count is important, but trends in the platelet count, specifically a decline by more than one-half, may be evidence of a serious clinical problem such as heparin-induced thrombocytopenia (HIT), which requires urgent attention. A systematic approach to the diagnosis allows for the common causes to be detected early and enables rational use of platelet transfusions (
Algorithm 62.1). Platelet survival in the circulation is approximately 7 to 10 days, and one-third of the platelets are sequestered in the spleen under normal circumstances.
Recognition of thrombocytopenia normally occurs after a complete blood count is drawn, but it is important to remember that mucocutaneous bleeding is a classic sign of thrombocytopenia. Bleeding from thrombocytopenia normally occurs only once the platelet count is <50,000/µL in postsurgical patients; spontaneous bleeding can occur with counts <5000/µL. The diagnostic approach starts with a thorough history and physical examination, followed by examination of the peripheral smear. A pathophysiologic approach to thrombocytopenia enables all common causes to be rapidly screened for and facilitates recognition of potential causes (
Table 62.1). Careful attention should be paid to prescription and over-the-counter drugs (
Table 62.2).
The common causes of thrombocytopenia in an ICU setting are as follows:
Drug-induced (heparin, H2-receptor blockers, GP2b3a inhibitors, antibiotics, alcohol)
Sepsis
Massive bleeding
Thrombocytopenia with microangiopathic hemolytic anemia (thrombocytopenic thrombotic purpura [TTP], hemolytic uremic syndrome [HUS], disseminated intravascular coagulation [DIC]).
Clinical recognition of the cause is vital, as the therapies differ considerably depending on the etiology. For example, a patient with thrombocytopenia secondary to bleeding should be treated with platelets compared with a patient with TTP/HUS, in whom platelet transfusion is generally contraindicated. A few common conditions will be discussed, and readers are encouraged to refer to Suggested Reading for further details.
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree