INTRODUCTION
As stroke care has changed rapidly over the last several decades, we continue to progress and are on the precipice of major change both in stroke care as well as health care. Several looming developments will impact the care of stroke patients in the short term, including clinical research, technological advances both in health care and other industries, and health care reform in the United States. Beyond the more immediate impact of developments in progress, the rapid pace of technological development and its adaptation to health care will undoubtedly impact the future of stroke patient management. This chapter will review the rapid evolution of stroke care over the past decades, the projected stroke patient population of the future, and the current and anticipated developments in the understanding and management of stroke at the individual and population levels.
Rapid Evolution of Stroke Care
The scientific and empirical bases for understanding stroke pathophysiology, treatment, and recovery have evolved at an astounding pace over the past three decades. As thrombolysis changed the entire paradigm of ischemic stroke treatment in the late 1990s, and intra-arterial treatment options for ischemic stroke and subarachnoid hemorrhage (SAH) evolved in the 2000s, stroke researchers and practitioners are expected to continue to rapidly produce research to guide individual and population-level interventions to improve outcomes for patients after stroke. Stroke caregivers and program leaders must work to remain current in their understanding of the science of stroke care and integrate new knowledge and best practices into the evidence-based care that supports optimal patient and population outcomes.
Clinical practice guidelines (CPGs) published and used throughout the world play a critical role in synthesizing current evidence and best practice and serve to guide stroke program organization and individual clinical care. A discerning caregiver should review CPGs with a critical eye. A review and recommendations on CPG trustworthiness conducted by the Institute of Medicine (IOM) in 2011 observed that the adoption of evidence-based medicine has resulted in over 3,700 guidelines from more than 39 countries (IOM, 2011). However, not all guidelines are created using the same degree of rigor. The trustworthiness of CPGs may be hindered by lack of transparency in the goal and methodology of guideline preparation and undisclosed real or potential biases or conflicts of interest from authors. Several tools are available to help evaluate the quality of a CPG, including the IOM guideline review tool, the Appraisal of Guidelines for Research and Evaluation (AGREE), the Cluzeau Appraisal Instrument, and Shaneyfelt Methodological Standards Tool (IOM, 2011).
Guidelines should be evaluated for their trustworthiness and applicability to clinical practice. Recommendations from the 2011 IOM Committee on Standards for Developing Clinical Practice Guidelines advise that guidelines should (IOM, 2011):
● Be based on a systematic review of the existing evidence
● Be developed by a knowledgeable, multidisciplinary panel of experts and representatives from key affected groups
● Consider important patient subgroups and patient preferences, as appropriate;
● Be based on an explicit and transparent process that minimizes distortions, bias, and conflicts of interest
● Provide a clear explanation of the logical relationships between alternative care options and health outcomes
● Provide ratings of both the quality of evidence and the strength of the recommendation
● Be reconsidered and revised, as appropriate, when important new evidence warrants modifications of recommendations.
In addition to disease-specific CPGs, other forms of recommendations provided by credible sources influence practice by addressing preventive services. For example, the U.S. Preventive Services Task Force (USPSTF) recently published a recommendation on screening for asymptomatic carotid artery stenosis. The USPSTF recommends against screening for asymptomatic carotid artery stenosis in the general adult population (LeFevre, 2014). It based its recommendation on the evidence of both the benefits and harm of the service and an assessment of the balance; it does not consider the cost of the service. The USPSTF uses a five-level grading scale from A to D, with A representing recommendation of the service and that there is high certainty that the net benefit is substantial. The grade of D represents a recommendation against the service and the statement that there is moderate or high certainty that the service has no net benefit or that the harms outweigh the benefits (LeFevre, 2014). The scale also includes an “I statement” which says that the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harm. The recommendation against screening for asymptomatic carotid artery stenosis was a grade D recommendation. Practitioners should monitor guidelines in their area of practice to say abreast of changes in recommendations.
 FORECASTING THE FUTURE OF STROKE
FORECASTING THE FUTURE OF STROKE
Global Burden of Stroke
A recent review of over 20 years of publications addressing the global burden of stroke revealed the startling impact of stroke beyond the United States. Whereas stroke is the fourth leading cause of death in the United States, stroke is the second leading cause of death and the leading cause of disability worldwide (Mukherjee & Patil, 2011). Although compiling epidemiological statistics for stroke spanning the globe is difficult, statistics from the World Health Organization (WHO) estimate that stroke accounts for more than 5.5 million deaths each year (Mukherjee & Patil, 2011). This number is expected to rise significantly by 2030, with an estimated 7.8 million deaths attributed to stroke.
Global stroke-related mortality reveals fluctuating outcomes according to a country’s income and prosperity. Projected stroke death rates in well-developed countries such as the United States and western European countries are similar and expected to remain relatively flat or even decline slightly over the next several decades (Mukherjee & Patil, 2011). However, stroke-related mortality rates in low- and middle-income countries are expected to increase significantly. For stroke in all age groups worldwide, approximately 85% of current global deaths from stroke occur in low- and middle-income countries. The number climbs to over 90% for stroke victims older than the age of 70 years.
The factors contributing to the tremendous global impact of stroke and disproportionate mortality burden seen in low- and middle-income countries are multifactorial and complex (Mukherjee & Patil, 2011; Ovbiagele et al., 2013). The lack of primary and secondary prevention strategies to address risk factors as well as the lack of organized stroke care is thought to be major factors impacting global stroke mortality. The global aging population also contributes to the overall stroke prevalence. Low- and middle-income countries often lack the primary care infrastructure to detect and treat hypertension, smoking, and diabetes mellitus, significant risk factors that contribute to the development of stroke.
Additionally, when stroke occurs, these countries lack the emergency medical service (EMS) response infrastructure to identify and facilitate timely treatment (Mukherjee & Patil, 2011). Even once stroke is identified, current best practice for stroke dictate the administration of thrombolytics for ischemic stroke and neurosurgical intervention for conditions in all stroke types. Thrombolysis for ischemic stroke is costly and requires specialist care. Most low- and middle-income countries lack a structure for administering thrombolytics as well as the neurosurgical and critical care infrastructure to care for stroke patients. Low- and middle-income countries often do not have neurology or neurosurgical subspecialty–trained practitioners.
Researchers postulate that primary care and prevention may be more sustainable and cost-effective as an initial initiative in low- and middle-income countries than building a treatment EMS infrastructure (Ovbiagele et al., 2013). Although this is a reasonable recommendation for policy planning, several countries such as India, China, Brazil, and Argentina have demonstrated positive steps to address both prevention and acute emergency response. As the United States and the more developed countries in Western Europe continue to develop new interventions to treat patients with stroke and new systems of care to improve overall stroke outcomes, the feasibility and sustainability of such efforts on a global scale must be considered.
United States Burden of Stroke
Stroke Statistics and Disparities
A recent analysis by the American Stroke Association projects the U.S. prevalence of stroke to increase to 3.4 million individuals in 2030 compared to 2012 statistics (Ovbiagele et al., 2013). The aging population in the United States plays a key role in this growth, as overall stroke incidence and mortality has declined in recent years. However, stroke is a disease primarily of the aged, and as the baby boomer generation ages into the 60s, the overall prevalence of stroke is expected to increase. An estimated 4% of the U.S. population will have survived a stroke in the year 2030, a statistic largely impacted by the falling mortality and improved stroke survival outcomes seen in recent years. This increase in stroke survivorship is expected to significantly impact the U.S. health care system and economy.
Further analysis of the U.S. statistics reveals the nation is experiencing its own disparities, and not all populations experience the decreased mortality and increased stroke survivorship seen at a national level (Ovbiagele et al., 2013). Stroke-related mortality is higher for the very old (>80 years of age) experiencing stroke, due in part to what appears to be a caregiver bias. Studies reveal that lifesaving interventions are often withheld in the very old experiencing stroke. Additionally, the very old appear to receive less stroke prevention interventions.
Stroke is a disease that disproportionally affects African Americans and Latino Americans in the United States. Although overall stroke incidence has decreased nationwide, the decrease is primarily in the Caucasian population. Stroke incidence continues to increase in African Americans and Latino Americans (Ovbiagele et al., 2013). When these groups experience stroke, their survival rates are also lower than those of Caucasians. Much like the global burden of stroke, these statistics are reflective of a multifaceted and complex problem. Access to primary care, acute stroke treatment, secondary prevention of stroke, as well as geographic and socioeconomic disparities likely all impact the higher stroke incidence and mortality experienced by African and Latino Americans. Additionally, there is some evidence that African Americans are less aware of stroke signs and symptoms than other races or ethnicities and less likely to call EMS when experiencing new stroke symptoms, resulting in delays in care (Ovbiagele et al., 2013). Furthermore, studies suggest that African Americans are less likely to receive standard stroke treatment once they arrive at the hospital with stroke signs and symptoms (Ovbiagele et al., 2013). These findings serve to further reinforce that stroke is not experienced in the same way by all races and ethnicities in the United States. Although national stroke incidence and mortality statistics are encouraging, additional research and initiatives are needed to ensure all Americans experience less strokes and receive the best treatments if they do experience a stroke.
Studies suggest that access to primary care as well as organized stroke care at the time of an acute event varies according to geographic region, with decreased access in regions with lower socioeconomic status (Ovbiagele et al., 2013). The stroke belt, a region in the southeastern United States in which stroke incidence and mortality is significantly higher than the rest of the nation, has been recognized for several decades in the stroke community. People experiencing a stroke in the stroke belt states have a 20% to 40% higher mortality rate compared to the rest of the nation. The exact cause for this significant disparity remains elusive, particularly as studies suggest that those who are born in the stroke belt states, but move to another area of the United States, are still at higher risk for stroke and death from stroke. The stroke belt is likely a confluence of factors including decreased access to primary care for management of stroke risk factors and decreased access to EMS care and stroke systems of care. Additional research and initiatives to address these disparities are needed.
Changing Causes of Stroke
As health care evolves and the burden of chronic disease such as heart disease, diabetes, and other risk factors for stroke evolve in coming decades, the causes of stroke are expected to shift (Ovbiagele et al., 2013). Some of the decrease in U.S. stroke incidence is attributed to improved primary prevention and control of risk factors such as hypertension and hyperglycemia. Although primary care of patients with hypertension has improved measurably, the rapid rise in obesity poses a significant risk for increasing the incidence of stroke in coming decades. Obesity is strongly associated with stroke risk factors, including hypertension, diabetes mellitus, dyslipidemia, and cardiovascular disease. The true impact of the obesity crisis has yet to be fully understood. Chronic obesity may contribute to increased stroke frequency and at a younger age.
With the aging population, chronic heart disease is expected to lead to an increased prevalence of heart failure and atrial fibrillation. Atrial fibrillation is a significant risk factor for ischemic stroke, and stroke prevention necessitates chronic anticoagulation. However, chronic anticoagulation is also a risk factor for hemorrhagic stroke. Therefore, the increase in heart failure and atrial fibrillation over the next several decades may result in an increase in both ischemic and hemorrhagic stroke.
 THE CHANGING STROKE LANDSCAPE
THE CHANGING STROKE LANDSCAPE
Several factors are expected to contribute to a changing stroke landscape over the next several decades. These factors build on significant work conducted thus far in the areas of clinical research, stroke systems of care, as well as health care structure and payment reform in the United States and internationally. The future of stroke care is expected to be molded by continued bench- and patient-focused clinical research as well as industry and technological developments at the level of the individual patient as well as population level.
National and International Advocacy
Several organizations support ongoing initiatives to measure and improve outcomes for stroke victims. At an international level, the WHO has supported epidemiological studies to measure the global impact of stroke and to build basic care infrastructures to improve stroke care infrastructure and outcomes. In the United States, the American Heart Association (AHA) established the American Stroke Association (ASA) in the late 1990s with the goal of decreasing disability and death due to stroke and reducing stroke death by 25% (Schwamm et al., 2010). The AHA/ASA has accomplished this mission through several initiatives including research, the development of stroke systems of care, and the development of a national database to measure the impact and outcome of stroke. The AHA/ASA has also worked in recent years to impact national and state legislation and set priorities for health care reform focused on stroke care and stroke recovery. The Brain Attack Coalition (BAC) and the National Institute for of Neurological Disorders and Stroke (NINDS) are two additional national organizations influencing stroke research, policy, and clinical care.
Research
Basic stroke research is uncovering the influence of genetics as a risk factor for stroke and biochemical genetic markers for stroke. For example, in a recent press release from the National Institutes of Health (NIH, 2014), the caption says, “Researchers Discover Underlying Genetics, Marker for Stroke.” Reporting on a study by Williams et al. (2014), the researchers studied the genomes of nearly 5,000 people and pinpointed a genetic variant tied to an increased risk of stroke. They also found that circulating homocysteine (tHcy), a product of the folate one-carbon metabolism pathway (FOCM) through the demethylation of methionine, is heritable and is associated with an increased risk of stroke, cardiovascular disease, cancer, and dementia. These findings may provide new clues to understanding the underlying genetic and biochemical influences in the development of stroke and cardiovascular disease and may also help lead to new treatment strategies (NIH, 2014). Although the translation from “bench to bedside” is a long road, this is a recent example of the kind of research that will lead to new knowledge and a better understanding of stroke. This research serves as a springboard for other research that will eventually lead to efficacy studies, clinical trials for effectiveness, and finally, translation into CPGs for better patient outcomes.
Another important area of research is pharmacogenomics, the study of the role of genetics in drug response. The goal of pharmacogenomics is to develop rational means to optimize drug therapy, with respect to the patients’ genotype, to ensure maximum efficacy with minimal adverse effects (Becquemont, 2009). This approach is tied to the development of “personalized medicine” in which drugs and drug combinations are optimized for each individual’s unique genetic makeup (Squassina et al., 2010). Clopidogrel (Plavix) is a thienopyridine-class antiplatelet agent used to inhibit blood clot formation in coronary artery disease and cerebrovascular disease. It is frequently prescribed for patients after stroke or stent placement. In 2010, the U.S. Food and Drug Administration (2010) announced a warning about Plavix to inform prescribers that the drug may not be effective in patients who carry a particular gene variant. About 30% of people cannot metabolize Plavix to convert it to an active drug. Without the intact functioning gene, the liver cells responsible for metabolism, known as cytochrome 2C19 (or CYP2C19), Plavix does not adequately suppress the platelets or prevent blood clots. The patient is placed unknowingly at risk. Without the knowledge of a person’s genetics, this drug could be prescribed to a patient with this genetic so-called loss-of-function allele (Topol, 2012).
The discussion of Plavix helps to frame a discussion of personalized medicine or personalized health care. With the recognition of genetic variability in an individual’s response to drug and other therapies, the need to tailor treatment according to the individual genetic profile of the patient is apparent. This challenge is overcome with individual patient genomics profiles generated by a growing number of high-throughput molecular platforms (Oracle Health Sciences, 2014). Personalized medicine focuses on delivering preventive and therapeutic treatments to those persons who will most likely benefit while sparing the expense and the side effects for those who will not benefit. Whole genome sequencing is a laboratory process that determines the complete DNA sequence of an organism’s genome at a single time (Harbron & Rapley, 2004). It includes gene sequencing at the single nucleotide polymorphisms (SNPs) level, enables scientists to pinpoint functional variants from association studies, and improves the knowledge available to researchers or predicting disease susceptibility and drug response (Li, Kadura, Fu, & Watson, 2004). The cost of whole genome sequencing is dropping significantly so that, in the future, it will be available to the general public as a tool to personalize and individualize health care. Are we there yet? The answer is no, but it is on the horizon. Biotechnology continues to make monumental strides in developing the methodology for clinical use.
Technology
New and innovative uses of technology are having a tremendous impact on stroke care now and will have in the future. The following briefly discusses a technology-rich future for stroke care.
Perhaps one of the most profound changes in the future will be with physiological monitoring in relationship to use of smart phones in association with new downloadable applications (apps) and other forms of wireless monitoring. In the past, a few physiological parameters such as blood pressure, pulse, respirations, and temperature were monitored with discrete measurements occurring over time. With available wireless technology and smart phones, the vital sign parameters plus many other parameters will be amenable to monitor on a continuous basis. Not only will the monitoring be continuous, but there will also be the ability to analyze the data continuously without having to download it to another program. Continuous monitoring of cerebral electrical activity with an ongoing electroencephalogram (EEG) will provide a mechanism to discern seizure activity and be able to associate it with activities in which the person is engaged. Monitoring a physiological parameter continuously around the clock has the advantage of being able to capture data through variations in real-life situations such as stress and sleep.
Although current intensive care unit (ICU) standard of care includes continuous monitoring of heart rate, heart rhythm, respiratory rate, and oxygen saturation, neurological assessment parameters such as monitoring of intracranial pressure (ICP) and EEG are generally collected in single discrete time samples hourly or less frequently. New bedside clinical care technology is attempting to integrate neurological physiology parameters such as ICP, EEG, and brain tissue oxygenation and adding cerebral microdialysis sampling of excitatory neurotransmitters such as glutamate to allow continuous monitoring of cellular cerebral function. Companies such as Moberg Research and Integra LifeSciences have recently launched neuromonitoring technologies aimed at continuous monitoring of these parameters (Integra LifeSciences, 2014; Moberg Research, 2014). The future ICU care for a stroke patient could include continuous multimodal neuromonitoring in addition to standard cardiopulmonary monitoring.
In the United States, the chronic disease burden largely results from a short list of risk factors including tobacco use, poor diet and physical inactivity (both strongly associated with obesity), excessive alcohol consumption, uncontrolled high blood pressure, and hyperlipidemia, all of which can be effectively addressed (Bauer, Briss, Goodman, & Bowman, 2014). All of these risk factors are also risk factors for stroke and need to be addressed simultaneously to prevent stroke or recurrent stroke in a patient who has had a previous stroke. Monitoring for these risk factors via smart phone and biosensor technology could help with immediate alerts both to the patient and health care provider. There could also be educational interventions that could be sent to the patient once a risk factor was identified. For stroke patients, in addition to the parameters already mentioned, sleep, blood coagulation, blood glucose, cardiac rate and rhythm for evidence of atrial fibrillation, and numerous other areas of interest can be monitored in a variety of settings across the continuum of care including home.
The medical appointment of the future may very well be a virtual appointment in which the health care provider will review data from these various sources with the patient and interaction with a real-time video presence. It remains to be seen if health policy, reimbursement, and the technology will support this possible future. Part of the criteria to measure quality may be to determine if care is safe, equitable, effective, efficient, timely, and patient-centered, as described by the IOM (2001).
Biotechnology
Biotechnology is defined as the manipulation (as through genetic engineering) of living organisms or their components to produce useful usually commercial products such as novel pharmaceuticals (Biotechnology, n.d.). It merges biological information with computer technology and includes nanotechnology. The size of technology is becoming smaller and portable. For example, the Vscan is a mobile echocardiogram unit that fits into the pocket of a laboratory coat. It is easy to use, provides reliable data, and allows the health care provider to give real-time feedback to patients about their cardiac function. One point to make about the technology for an echocardiogram is that it does not require ionizing radiation like an x-ray, computed tomography scan, fluoroscopy, or nuclear scans. The need for ionizing radiation is a limiting factor for making these diagnostics as small and mobile as the echocardiogram (Topol, 2012).
Nanotechnology is science, engineering, and technology conducted at the nanoscale, which is about 1 to 100 nanometers (nanometers = one billionth of a meter). A nanometer is 40,000 smaller than the thickness of human hair. Nanotechnology is the study and application of extremely small things and can be used across all the other science fields, such as chemistry, biology, physics, engineering, and medicine (National Nanotechnology Initiative, 2014). When applied to medicine, nanotechnology is the medical applications of nanomaterials, nanoelectronic biosensors, and even possible future applications of molecular nanotechnology. The possibilities of wireless sensors and genomics for targeted therapies are incredible. Nanotechnology is expected to revolutionize drug delivery, gene therapy, diagnostics, and many areas of research, development, and clinical application. Nanotechnology is being used for targeted drug therapies with more effective drug delivery systems leading to fewer side effects. It is in the early stage of developing scaffolding in nerve regeneration research which could someday lead to replacement of the brain tissue injured by stroke (Project on Emerging Nanotechnologies, 2014). The possibilities for stroke prevention and treatment are huge.
Robotics
Robotics is the use of computer-controlled robots to perform manual tasks. In medicine, robotics is used for surgery, patient care, and rehabilitation. It is frequently used after stroke, traumatic brain injury, spinal cord injury, or other nervous system conditions related to loss of function. For stroke patients, robotics could be used for surgical complexity and precision procedures such as hematoma removal. In stroke rehabilitation, robotics are being used to assist with cognitive disorders, communication deficits, sensorimotor training of paralyzed or paretic limbs, balance retraining, and other stroke-related deficits (Fasoli, Krebs, & Hogan, 2004; Volpe et al., 2000). For example, robot-based technologies such as the Lokomat (Sensory-Motor Systems Lab) are designed to combine medical and engineering approaches to help patients regain mobility faster, with less pain. The Lokomat uses a robot to automate treadmill training, affording patients longer and more frequent sessions and resulting in a faster and improved return to mobility. The robot intelligently adapts its behavior to the patient’s individual capabilities. Improved pelvis and hip actuation and control can make walking with the Lokomat more natural, and virtual training environments can increase patients’ motivation and engagement (Diana, 2011). Although robotics is not new to stroke rehabilitation, its use will expand and become a standard practice in stroke rehabilitation.
The integration of technology on the future of stroke care and management is sure to have a huge impact on both the prevention and treatment of stroke. The previous discussion is but a quick glimpse on what the future holds.
Improved Clinical Care
The current U.S. health care system disproportionality focuses on acute care rather than primary care and secondary prevention efforts. Improved primary prevention focused on mitigating stroke risk factors will have a clear impact on stroke incidence and stroke recovery. The Affordable Care Act (ACA), enacted in 2010, promises an increased focus on primary care and disease prevention. The act is still in the early phases of implementation, and the full impact of health care reform on primary care and the future of stroke remains to be seen. The potential impact of the ACA is discussed in more detail in the following text.
Related to recognition of stroke risk and prevention, current efforts are underway to develop electronic tools to calculate risk of stroke. One can envision a future where all people have the ability and accountability for measuring their future stroke risk using such tools. With the significant focus on the cost of health care and the individual’s role in risk reduction, one can envision a future where all individuals have calculate their risk for disease and will be held accountable for risk factor reduction. Although controversial, population-level interventions aimed at targeting high-risk health behavior using taxation, reporting, and adjustment of health premiums has been successful to change. Behaviors such as smoking, obesity, uncontrolled diabetes, and uncontrolled hypertension are all risk factors for stroke that the individual may be increasingly responsible for reporting and held accountable for behavior change.
Clinical care at a population level has been greatly impacted by the development of stroke systems of care. The past decade has seen the development of two stroke program certifications, primary stroke center (PSC) and comprehensive stroke center (CSC) certification offered by several regulatory safety and quality agencies. To date, approximately 1,400 of the 5,700 national hospitals are certified as PSCs, and 69 facilities are certified as CSCs (American Hospital Association, 2014). Additionally, nearly half of the states in the United States have enacted legislation guiding the development of stroke systems of care, generally supporting hospital stroke certification and prehospital bypass of non–stroke-certified facilities. Some states have developed registries and require health care organizations to submit outcomes to the state, in addition to national and regulatory reporting.
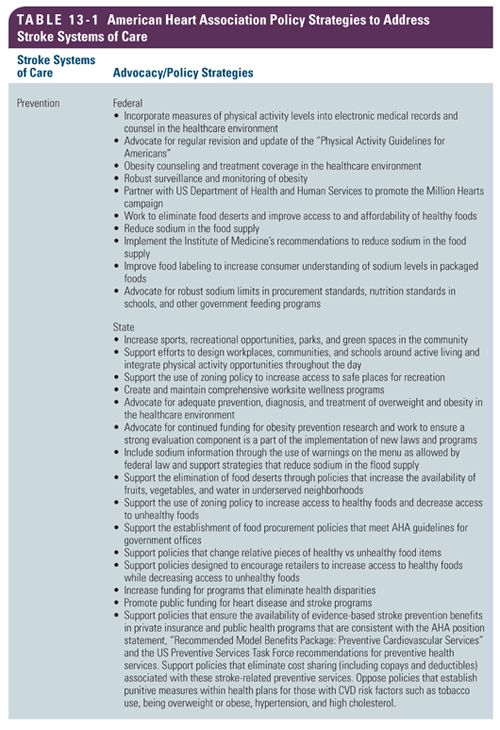
Although stroke certification levels have developed and gained popularity over the past decade, a full stroke system that allows all U.S. residents access to expert stroke care is yet to be realized. Currently, it is unclear how PSC and CSCs work together to ensure all people in the nation have access to organized stroke care. Furthermore, much of the rural United States remains more than 60 minutes away from a PSC or CSC. Although many states have enacted stroke system of care legislation, states vary in their level and stage of implementation and sophistication. The AHA/ASA recently outlined a series of national, state, and EMS policy priorities to further improve stroke systems of care in the United States. Table 13-1 shows a comprehensive list of ASA/AHA policy initiatives (Ovbiagele et al., 2013).


Full access? Get Clinical Tree


