Chapter 42 The Difficult Airway in Neurosurgery
II The Neurosurgical Patient
The American Academy of Neurological Surgeons (AANS) estimates that almost 1 million neurosurgical procedures are performed annually in the United States. Spine procedures are performed at three times the rate of cranial surgeries.1 When considering the range of potential neurosurgical procedures, the variety of patient pathophysiology is substantial. A patient presenting for neurosurgery may appear to be completely normal or can present with clinical symptoms of intracranial hypertension. The airway might be assessed as “normal” but the patient’s head is fixed in a frame. Also, the patient may present with acromegaly for pituitary surgery or may have a previous history of difficult intubation. Additionally, the unanticipated difficult airway becomes an even greater challenge in patients at risk for cerebral aneurysm rupture. Other challenges include the spine surgery patient in the prone position and considerations for extubation after prolonged surgery. Patients with central nervous system (CNS) disease can be sensitive to the effects of hypnotic agents, rendering them susceptible to apnea when premedication is given.
Neurosurgical procedures comprise only 7% of cases in the American Society of Anesthesiologists (ASA) closed-claims database but are associated with settlements that are 1.6 to 4 times more than general surgical procedures.2 Understanding the patient’s physiologic requirements, in addition to the surgeon’s plan, is extremely important in these patients. It is wise to have a number of techniques for achieving, maintaining, and rescuing the neurosurgical airway.
A Intracranial Dynamics and the Airway
Intracranial pressure (ICP) is the pressure within the rigid skull. Airway management in the face of intracranial hypertension is a frequent challenge for the neuroanesthesiologist, as well as the emergency physician. The patient who does not require immediate airway control may benefit from the simple maneuver of elevating the head. The head-up position may have beneficial effects on ICP through changes in mean arterial pressure (MAP), airway pressure, central venous pressure, and cerebrospinal fluid displacement.3 Cerebral perfusion pressure (CPP) is the effective perfusion pressure driving blood through the brain, defined as the difference between mean arterial and intracranial pressures (CPP = MAP − ICP). A frequent consideration in the neurosurgical patient is the need to balance and maintain intracranial dynamics, avoiding increases in ICP, yet maintaining cerebral perfusion. Although head elevation may reduce ICP, raising the head above 30 degrees may place the patient at risk for venous air entrainment and should be done with caution.
Ventilation is intimately related to cerebral blood flow (CBF) and is an integral part of neuroanesthesia management. The avoidance of hypercarbia is essential in management of patients with intracranial hypertension. Carbon dioxide dilates the cerebral blood vessels, increasing the volume of blood in the intracranial vault and therefore increasing ICP. Periarteriolar hydrogen ion concentration, [H+], powerfully influences cerebral arteriolar tone, and as the arterial carbon dioxide tension (PaCO2) rises, [H+] increases, causing arteriolar dilatation. This leads to a concomitant decrease in cerebrovascular resistance, causing an increase in CBF, and an increase in cerebral blood volume (CBV).4 Difficult mask ventilation may quickly lead to hypercarbia, hypoxemia, and increased CBF. Hypoxia also remains one of the more potent arteriolar cerebrovascular dilators. Changes in the arterial oxygen tension (PaO2) are associated with late increases in CBF. Hypoxia or ischemia leads to marked vasodilation, increased arterial vascular volume, and intracranial hypertension.5
Laryngoscopy and intubation, if performed with difficulty or improperly, can severely compromise intracranial dynamics and increase morbidity. Both the sympathetic and the parasympathetic nervous system mediate cardiovascular responses to endotracheal intubation.6 Acute increases in ICP and MAP during laryngoscopy and endotracheal intubation have been well documented.7 In 1975, Burney and Winn8 measured ICP in 12 patients undergoing craniotomy and two patients for carotid arteriography. ICP did not change in response to the injection of contrast medium but increased significantly and dramatically in response to laryngoscopy and intubation. The increase appeared related to the initial ICP of these patients, possibly representing exhaustion of compensatory mechanisms. Special attention must be given to this factor during manipulation of the larynx in neurosurgical patients with initially increased ICP or space-occupying intracranial lesions.
Techniques to blunt this sympathetic response have included (1) an additional dose of thiopental or propofol, (2) use of beta-blockers or other antihypertensive agents, and (3) use of intravenous (IV) lidocaine. Esmolol or lidocaine as an IV bolus of 1.5 mg/kg before laryngoscopy and intubation did not completely prevent the increase in MAP and ICP.9,10 Etomidate has been shown to cause an early “burst” suppression pattern on the electroencephalogram (EEG), minimal changes in CPP, and a marked reduction in ICP. This decrease in ICP was maintained during the first 30 seconds and the following 60 seconds after intubation, as MAP and heart rate remained unchanged.11 Although not practical, this approach demonstrates the extent of efforts often made to obtund this response. Numerous methods have been advocated to prevent undesirable cardiovascular disturbances at intubation.12 Whereas the cardiovascular response can be dramatic and substantial, the ICP response may lag behind and persist longer. Once the patient is intubated, ventilation parameters may be adjusted to the clinical situation.
III Clinical Strategies for the Neurosurgical Patient
A Patient for Craniotomy
Patients who are neurologically intact may demonstrate no evidence of intracranial pathology or alteration. In addition to the history and physical examination, preoperative computed tomography (CT) or magnetic resonance imaging (MRI) scans of the head may give valuable information, because lesions associated with greater than 10 mm in midline shift or cerebral edema usually indicate intracranial hypertension.13 These patients should be appropriately managed to avoid undue increases in ICP and CBF. Such measures include proper head positioning, preoxygenation, and appropriate dosing of induction agents and relaxants to achieve a smooth intubation. The primary challenge in anesthetizing a patient with a supratentorial mass lesion is to avoid further increases in ICP when one has limited intracranial compliance. There is no “ideal anesthetic” for this group of patients, and the perioperative management should be individualized. However, the practitioner should be aware of the effects of anesthetic agents on intracranial dynamics.
The preoperative use of midazolam for anxiety in these patients should not cause harm if they are carefully observed. A 1-mg to 2-mg dose of IV midazolam in adult patients may facilitate the induction of anesthesia without altering intracranial dynamics.14 Opioids, on the other hand, should be restricted to very small amounts and given preoperatively under constant supervision because of possible hypercarbia and resultant effects. The efficacy of depth of anesthesia was recognized early on as a technique for avoiding intracranial hypertension.15 Deep inhalation anesthesia was replaced by a combination of intravenous induction agents, notably thiopental, in combination with fentanyl. Thiopental produces a dose-dependent reduction in CBF and cerebral metabolic rate of oxygen consumption (CMRO2). Other barbiturates, such as pentobarbital and methohexital, essentially have similar effects. ICP is reduced by barbiturates, likely because of the reduction in CBF and CBV. Propofol has largely replaced thiopental as the induction agent of choice for neuroanesthesia. Despite initial concerns about decreasing MAP and CPP, propofol provides a smooth transition to unconsciousness without an increase in heart rate, as observed with thiopental. This often produces less hypertension with laryngoscopy and intubation.16
Clinical doses of most opioids have minimal to modest depressive effects on CBF and CMRO2. Early studies demonstrate that ICP is either not elevated or slightly decreased with fentanyl alone or in combination with droperidol. Reported ICP increases in patients with space-occupying lesions have been attributed to hypercapnia. The variability in response to opioids appears to be caused by the background anesthetic. When vasodilating drugs are used as part of the anesthetic management, the effect of the opioid is consistently that of a vasoconstrictor. Sufentanil was thought to produce an increase in ICP in patients with intracranial mass effect, but this was later attributed to a decrease in MAP.17 Alfentanil produces little changes or slight decreases in CBF.18 The beneficial effect of synthetic opioids is their ability to blunt the hemodynamic response to laryngoscopy and intubation without affecting intracranial dynamics. Remifentanil produces the most profound and consistent response, with lack of hypertension, tachycardia, or increase in ICP.19 A continuous infusion throughout induction may provide the most effective hemodynamic control, while adequate ventilation is maintained.
The volatile agents, including nitrous oxide, can be considered dose-dependent cerebral vasodilators.20 As a component of neuroanesthesia, volatile agents are typically used in moderate doses, in combination with opioids and hypnotic agents. The effects on cerebral circulation and metabolism of sevoflurane and desflurane are largely comparable to isoflurane. Both induce a direct vasodilation of the cerebral vessels, resulting in a less pronounced increase in CBF, compared to the decrease in cerebral metabolism.
Induction may be followed by hyperventilation with a volatile agent to deepen the anesthetic, decrease CMRO2 (and CBF), and provide bronchodilation in patients with asthma or chronic obstructive pulmonary disease. Sevoflurane is useful in both pediatric and adult patients by allowing inhalation induction without the adverse effects of coughing or breath-holding.21 A frequently employed technique in the cooperative patient is the use of active hyperventilation before induction, to initiate hypocapnia and decrease CBF as the patient loses consciousness. The use of topical anesthesia applied to the larynx and trachea can also prevent further response to laryngoscopy and intubation.22 The large number of techniques recommended to suppress cardiovascular responses indicates that no single method has gained widespread acceptance (Table 42-1).
Table 42-1 Anesthetic Techniques to Avoid Increased Intracranial Pressure
| Technique | Precaution(s) |
|---|---|
| Avoid hypercapnia. | |
| Avoid hypoxia. | |
| Avoid marked hypertension. | |
| Avoid severe neck rotation. | |
| Avoid compression of jugular veins. | |
| Elevate head. | |
| Decrease blood viscosity and intracerebral vascular volume. | |
| Avoid sustained increases in intrathoracic pressure. | |
| Avoid cerebral venodilators. |
PEEP, Positive end-expiratory pressure.
Alternative devices, such as the lightwand, can be useful in failed intubation, particularly in patients with a small chin or limited mouth opening. Because a lightwand is inserted without use of a laryngoscope, there is potential for less hypertension and tachycardia. This finding was demonstrated by Nishikawa and associates23 in 60 patients undergoing awake intubation for emergency surgery. Its successful use in the difficult airway requires experience and practice. Brimacombe and Kihara24 compared the hemodynamic responses of the lightwand and intubating laryngeal mask airway (ILMA) to direct laryngoscopy in hypertensive and normotensive patients. In their series, both the ILMA and the lightwand attenuated the hemodynamic stress response to tracheal intubation compared with direct laryngoscopy in hypertensive, but not in normotensive, anesthetized paralyzed patients. Optical stylets, such as the Shikani Optical Stylet scope or the Clarus Video System, have similar characteristics and insertion technique with the added benefit of laryngoscopic viewing (Fig. 42-1) The ILMA is particularly useful in the failed intubation sequence, and the ability to ventilate is extremely important in neurosurgical patients. The success of the ILMA as a ventilatory device has been impressive, as demonstrated in several of the early evaluation studies.25,26 It is also extremely useful in the setting of a failed fiberoptic intubation.27

The patient for aneurysm surgery who presents with a difficult airway is particularly problematic. If the airway is anticipated or known to be difficult, fiberoptic intubation is often the method of choice. This is assuming that one is skillful using the fiberoptic scope and is prepared to perform this technique in the awake, cooperative patient (see Chapter 11). IV fentanyl and midazolam may be carefully administered if the patient does not exhibit signs of intracranial hypertension. An arterial line is generally placed before induction. Additional techniques include remifentanil infusion (0.05 µg/kg/min) and dexmedetomidine infusion.28,29 Both techniques require careful patient monitoring and may be useful. Once the glottis is viewed, a dose of lidocaine may be given via the fiberoptic scope to prevent coughing and “bucking” with intubation.
B Head-Injured Patient
Traumatic brain injury (TBI) remains a prevalent disease in the United States and the world. The incidence of TBI is 175 to 300 per 100,000 population and accounts for 56,000 deaths per year in the United States.30 With the increased use of seatbelts, motor vehicle crashes are now secondary to gunshot wounds as the leading causes of TBI. Early intubation of the head-injured patient is critical and is often established in the field if providers are so trained. It is essential for optimal management of the patient, providing for efficient ventilation and oxygenation, helping to prevent aspiration of gastric contents, and allowing for suction of the lungs and pulmonary toilet. However, patients who are unconscious and breathing adequately may be transported with oxygen by mask throughout their initial assessment. This is intuitive in the apneic and unresponsive patient with a Glasgow Coma Scale (GCS) score of 8 or less.
The anesthesiologist caring for the patient with TBI must understand that although primary mechanisms of injury (primary insults) are a large determinant of patient outcome, attention to secondary insults, such as hypoxia, hypotension, intracranial hypertension, and decreased CPP, can impact dramatically on morbidity, mortality, and quality of life of the TBI patient.31 Evidence supports this, with mortality from TBI nationally decreasing over the decades.32 Hypoxia in TBI patients is a frequent occurrence, particularly in the prehospital setting. Interestingly, hypoxia was identified in 44% of patients with TBI on arrival in the emergency department.33 Similarly, Jeremitsky and colleagues34 report that hypoxia is one of three predictors of mortality in adult brain-injured patients (with hypothermia and hypoperfusion). Hypoxia dramatically impacts morbidity and mortality in TBI, and hypercapnia further increases mortality.
Hypotension is the secondary insult that has been most frequently cited as contributing to poor outcome after TBI. Hypertension is independently related to mortality in multivariate analysis.34 Information from the Traumatic Coma Data Bank shows that a systolic blood pressure less than 80 mm Hg was one of five factors that worsened patient outcome at 6 months.35 Hypotension during any phase in the brain trauma patient’s hospital course is associated with a greater likelihood of severe disability and vegetative state.36 However, early in the course of brain trauma, especially when combined with hypoxia, hypotension is devastating. When hypotension and hypoxia occur together, mortality is 75%.35
Techniques minimizing head movement should be used in TBI patients and by the most skilled clinicians. However, concern about a cervical fracture should never take precedence over relieving hypoxemia. It is of critical importance to ensure that appropriate monitoring is present throughout airway maneuvers. Nasal intubation should be avoided in head injury, particularly in patients with known or suspected basilar skull fractures and sinus injuries. Alternative airway devices, such as video laryngoscopes, any of the indirect rigid laryngoscopes, ILMA, or fiberoptic stylets, may be useful when the head must remain immobilized.37 Most emergency patients are assumed to have a “full stomach,” so it is important to weigh the risk of aspiration, which is a potential problem during laryngoscopy and intubation. If the situation warrants, surgeons should be prepared to perform a rapid cricothyrotomy if intubation attempts fail and ventilation becomes impossible.
C Patient with Cervical Spine Disease
1 Management of Acute Injury and the Unstable Spine
Spinal injuries occur in approximately 13% to 30% of polytrauma patients, and cervical spine injury (CSI) represents about 0.9% to 3% of all polytrauma patients.38,39 The relative risk of CSI is increased in the presence of severe head injury by a factor greater than 8.40 In the United States, cervical trauma has an incidence of approximately 5 per 10,000 population annually, making up 4% of all blunt trauma. In trauma victims with a GCS score of 13 to 15, the incidence of CSI is 1.4%, but this rises dramatically to 10.2% if the GCS score is less than 8. It is of vital importance to capture all injuries in the unconscious polytrauma patient within an emergent time frame. If a CSI is missed or its detection delayed, the incidence of secondary neurologic deficit increases from 1.4% to 10.5%. For this reason, the Advanced Trauma Life Support (ATLS) protocol was created, constantly updated, and broadly followed in most trauma centers.41 When a diagnosis of CSI is delayed, almost one third of patients may develop permanent neurologic deficit.42 One of the areas of controversy is how best to “clear” the cervical spine in the trauma patient. Detection of CSI requires a variety of modalities that vary in sensitivity, including clinical evaluation, plain radiography, CT, MRI, and dynamic fluoroscopy.
Clinical Evaluation
To clear the cervical spine clinically, the following criteria must be met:
1. GCS score of 15, with the patient alert and oriented
2. Absence of injuries that may draw attention away from a CSI
3. Absence of drugs or intoxicants that may interfere with the patient’s sensorium
4. Absence of signs or symptoms on examining the neck, specifically:
Clearly, there will only be a small number of trauma patients who fulfill these criteria.
Plain Radiography
The cross-table lateral view alone, even if technically adequate and interpreted by an expert, will still miss 15% of cervical injuries. Of cross-table lateral films taken in emergency rooms, approximately a quarter of the films are anatomically inadequate, necessitating further imaging modalities for evaluation, usually of the cervicothoracic junction. A three-view cervical series includes the cross-table lateral view, open-mouth odontoid view, and anteroposterior (AP) view (Figs. 42-2 to 42-4). Using these views, the sensitivity increases to detect 90% of those with an actual injury. Again, anywhere from 25% to 50% of these series may be inadequate anatomically. In low-risk patients, plain radiography is an efficient diagnostic examination with specificity of 100%. In high-risk patients, plain radiography is a good adjunctive screening test in conjunction with a CT scan, with sensitivity of 93.3% and specificity of 95%.

Figure 42-2 Normal lateral cervical x-ray view.
(Courtesy of Prasanna Vibhute, MD, Department of Radiology, Mount Sinai Medical Center.)
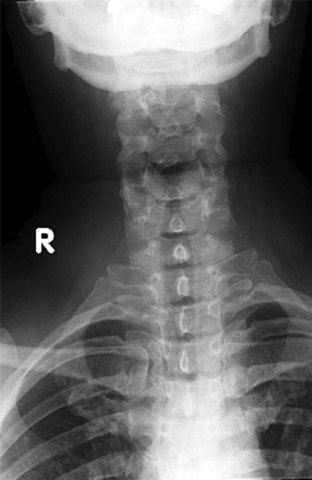
Figure 42-3 Normal anteroposterior cervical spine x-ray view.
(Courtesy of Prasanna Vibhute, MD, Department of Radiology, Mount Sinai Medical Center.)

Computed Tomography
CT scanning, either of the entire cervical spine or directed at areas missed by plain radiographs, provides a complementary approach when used in addition to the three-view cervical series, reducing the risk of missing a CSI to less than 1%. In the evaluation of the cervical spine, a helical CT scan has higher sensitivity and specificity than plain radiographs in the moderate-risk and high-risk trauma population, but it is more costly. In fact, a helical CT scan is the preferred initial screening test for detection of cervical spine fractures among moderate- to high-risk patients seen in urban trauma centers, reducing the incidence of paralysis resulting from false-negative imaging studies and institutional costs, when settlement costs are taken into account.42
a Intubation
The anesthesiologist or emergency physician may be confronted with a patient with CSI who requires intubation. In one series, 26% of patients admitted to a large trauma center required intubation over the first day of admission. Furthermore, a growing body of literature indicates that any patient with a CSI above C5 should be intubated electively, early in the course of presentation.43 The following survey reviews airway devices and assigns utility based on clinical presentation of cervical injury.
i Direct Laryngoscopy
If performed appropriately, direct laryngoscopy is safe in the patient with CSI.44–46 No neurologic sequelae were noted in a review of 73 patients with known cervical spine fractures intubated after rapid-sequence induction with the application of cricoid pressure and manual in-line stabilization (MILS) of the head and neck and direct laryngoscopy.47 When intubating the patient with direct laryngoscopy, the anterior portion of the hard cervical collar can be removed to facilitate opening of the mouth at intubation.
The major concern during the initial management of patients with potential CSI is the further deterioration of the neurologic function caused by pathologic motion of the injured vertebrae. Therefore, to protect the spinal cord, it is crucial to maintain spinal alignment and preserve spinal stability by establishing early immobilization of the spine. Techniques to provide cervical spine immobilization include sandbag-tape immobilization and cervical collars of various consistency.48 The same rationale is applied when management of the airway is required in the patient with suspicious CSI. The goal is to achieve endotracheal intubation as quickly as possible with the least amount of cervical motion. Although thorough evaluation for respiratory failure is necessary, current consensus is that early intubation is mandatory in patients with complete CSI, and evidence of respiratory failure should prompt immediate airway intervention.49 As currently recommended by ATLS protocol, direct laryngoscopy with MILS is most often performed and has been extensively investigated.50
The effects of direct laryngoscopy have been studied in a range of patients, including those with normal neck anatomy under anesthesia, as well as in cadavers, including those with cervical lesions caused to simulate fractures at a variety of levels. In the anesthetized patient with normal cervical anatomy, using neuromuscular blockade and a no. 3 Macintosh blade, a variety of movements occur. On elevation of the blade to obtain a view of the larynx, there is superior rotation of the occiput and C1 in the sagittal plane, C2 remains near-neutral, and there is mild inferior rotation of C3 to C5.51 The most significant movement is produced at the atlanto-occipital and atlantoaxial joints.45 In cadaveric models of unstable cervical segments (C1-C2), the movements associated with maneuvers such as chin lift and jaw thrust are greater than those produced by the intubation itself. The application of cricoid pressure produced no significant movement at the site of injury in these patients.6
ii Immobilization
In view of the risk of secondary neurologic injury to the acutely injured, unstable cervical spine, it is widely viewed as standard of care to immobilize the cervical spine when this is suspected. The most common measures include manual in-line immobilization, immobilization of the head between two sandbags, and placement of a rigid cervical collar and a spinal board. This management is itself associated with significant morbidity and mortality. It may increase the difficulty of intubation or increase the likelihood of airway compromise and risk of aspiration. Nonetheless, the use of manual in-line immobilization (not traction) is the best means to minimize movement of the cervical spine during airway manipulations and should always be practiced. It should be recognized, however, that the presence of a cervical collar does not necessarily protect against movement at the occipitocervical and cervicothoracic junctions.52
In all these studies, a certain degree of movement of the cervical spine was detected during direct laryngoscopy with MILS. The magnitude of the reported displacement was within the physiologic ranges. In addition, no difference was detected in the movements recorded by using three different blades (Macintosh, Miller, McCoy). Santoni and colleagues53 recently reported a direct correlation between the worsening of the glottic view caused by MILS and the increase in maximum applied pressure by the laryngoscope blade. They concluded that this increase in the force applied through the laryngoscope could worsen cervical instability. In the presence of cervical instability, impaired glottic visualization and secondary increases in pressure application with MILS have the potential to increase pathologic craniocervical motion.
The laryngoscopic pressure, which reflects a degree of difficulty in glottic visualization, can be significantly diminished by using video laryngoscopes, such as the Airtraq and the Pentax AirwayScope54,55 (Fig. 42-5). These channeled video laryngoscopes allow for indirect laryngoscopy and provide optimal view of the glottis without alignment of the oropharyngeal and orotracheal axes. For these reasons, they have been successful in allowing tracheal intubation in the presence of cervical collars. The GlideScope is a widely used video laryngoscope with a record of success in cervical spine immobilization.56,57 Using cinefluoroscopy, Robaitaille and colleagues58 found that the GlideScope did not produce less cervical spine movement than the Macintosh blade but did provide an improved laryngoscopic view and successful intubation (Fig. 42-6).


iii Awake Intubation
In a cooperative patient, awake fiberoptic intubation can be performed. One of the benefits of this technique is that it allows for the patient to be intubated without movement of the cervical spine. It may be performed with a hard collar in place. The patient’s airway may be topicalized, but this may, in theory, increase the potential for aspiration in patients at risk for regurgitation and aspiration. Ovassapian and others,59 however, found no evidence of aspiration in 105 patients at risk. Awake fiberoptic intubation may prove to be time-consuming and requires expert topicalization and operator skills for success. Because of the lack of assurance of expedient intubation and the risk of aspiration, we advocate that the fiberoptic scope be used in the cooperative patient in the urgent situation and in the nonurgent patient who is not at risk of aspiration. This recommendation is a general guideline, and expertise with any given airway device must be considered when using an airway technique in a specific clinical situation.
iv Laryngeal Mask Airway
Another alternative to direct laryngoscopy is the intubating LMA. Waltl and associates60 reported that the ILMA produced less extension of the upper cervical spine than direct laryngoscopy.61 Ferson and colleagues,62 in 254 difficult-to-manage airways, reported that 70 patients with acutely unstable necks were all successfully intubated with the ILMA, 92.6% on the first attempt and 7.4% on the second attempt.62 There was no report of worsening neurologic outcome or aspiration as a result of this intervention. The authors were skilled users of the device and practicing anesthetists who had vast clinical experience with the ILMA. Other studies were not as successful. Bilgin and Bozkurt63 reported that optimum conditions for ventilation through the ILMA could be achieved at the first attempt only in 59% of the patients wearing a semirigid neck collar, and that two to four attempts were necessary in 42% of the patients. Successful blind intubation could be performed in all patients, but only 53% at the first attempt. On the contrary, first-attempt and overall success rates were reported to be higher than with blind techniques using a flexible fiberoptic scope or lightwand-guided tracheal intubation under vision through the ILMA. The clear disadvantage of this approach was the prolonged intubation time.63
This information must be viewed, however, in light of cadaveric experiments in which the intubating LMA has been demonstrated to create posterior pressure on the midportion of the cervical spine.64 This may be particularly relevant in cervical flexion injuries. If the ILMA is to be used in a patient in a hard cervical collar with cricoid pressure, one should be aware of difficulties described in this scenario. Wong and associates65 presented two cases where the ILMA was used in awake topicalized patients with unstable cervical spine without difficulty. In light of these studies indicating that the ILMA may produce cervical motion and excessive pressure on the cervical spine, and that it is difficult to place with application of cricoid pressure and the presence of a hard cervical collar, the ILMA cannot be recommended as a primary device in the patient with acute cervical injury. It should be viewed as a rescue device if direct or fiberoptic intubation fails.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Ultrasonography in Airway Management
Ultrasonography in Airway Management
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


