(1)
Aschaffenburg, Germany
3.1 Introduction
3.3 Epidemiology
3.5 Diagnostics
3.6 Classification
3.7 Therapy
3.7.1 Conservative Treatment
3.7.2 Surgical Treatment
3.8 Results
3.1 Introduction
At the axilla and the upper arm, the radial nerve can be damaged by acute and chronic pressure influence, depending on the strength and duration of the influence even leading to paresis.
Exogenous causes at the axilla may be the incorrect use of crutches, supporting body weight resulting in pressure damage of the nerve between the proximal section of the humerus and the tendons of the latissimus dorsi and teres major muscles (Tackmann et al. 1989). Pressure damage of the radial nerve is more frequent in the course of its flat spiral channel, as here it runs in direct contact with the humeral shaft. Typical examples are the “park paralysis”, the “Saturday-night paralysis” and the “Paralysie des Amoureux”, which can develop in sleeping deeply, further on the paralysis caused by tourniquet and by position, during surgical procedures with anaesthesia. In literature the special vulnerability of the radial nerve at the spiral channel is connected to its unique situative conditions at the humeral shaft. Further damage of the radial nerve can occur during birth, by compression, by traction or by masses (haematoma, tumour).
There was no proof of the existence of a proximal radial nerve compression mechanism, even though Gowers as early as 1892 reported three complete radial pareses after a sudden contraction of the triceps muscle, for instance, by throwing a heavy stone. Similar pareses have been described in the past, especially after chronic overexertion of the triceps muscle, as in harbour and garbage workers, weavers, waiters and violinists. This is also true for secondary pareses in the further course of an upper arm fracture and in infectious and tumourous change, already predicting the existence of a proximal compression mechanism at the upper arm.
Only accidental work with radial paresis after certain motion patterns in the elbow joint with overexertion of the triceps muscles, for example, after long travels by car, and in work with compressed air equipment in 1969 led to a solution concerning localisation and pathogenesis of a proximal radial compression syndrome (PRKS), first published by Wilhelm in 1970 (Tables 3.1 and 3.2), based on eight patients surgically treated in the Surgical Department of the Teaching Hospital Aschaffenburg between 1969 and the beginning of 1970.
Table 3.1
Proximal radial compression syndrome (PRKS): N p (1969–1990) = 30, N op = 30
Pat. no. | Operation no. /year | m | w | Age | Profession | Loc. R/L | Causes | ||
|---|---|---|---|---|---|---|---|---|---|
Acute trauma | Chron.trauma | Triggering factor | |||||||
1 | 1,263/69 | + | 27 | Machine setter | L | + | Ball callus | ||
2 | 1,560/69 | + | 63 | Metal worker | R | + | Profession | ||
3 | 2,670/69 | + | 34 | Driver | L | + | Profession | ||
4 | 2,746/69 | + | 65 | Housewife | R | + | Osteitis | ||
5 | 238/70 | + | 27 | Drill worker | L | + | Profession | ||
6 | 785/70 | + | 41 | Varnisher | L | + | Profession | ||
7 | 1,364/70 | + | 20 | Plumber | L | + | Osteitis | ||
8 | 1,648/70 | + | 50 | Retired | R | + | Anat. spec. feature | ||
9 | 3,050/70 | + | 65 | Housewife | L | + | FA-fracture | ||
10 | 275/71 | + | 50 | Bricklayer | L | + | Profession/anat. spec. feature | ||
11 | 3,625/71 | + | 63 | Housewife | R | + | Edema/TIS | ||
12 | 1,721/72 | + | 45 | Worker | R | + | Profession | ||
13 | 3,096/73 | + | 40 | Housewife | R | + | FA-pseudarthrosis | ||
14 | 3,339/75 | + | 26 | Roughcaster | R | + | Hard work | ||
15 | 3,357/75 | + | 37 | Bricklayer | R | + | Hard work | ||
16 | 1,666/78 | + | 52 | Bricklayer | R | + | Profession | ||
17 | 1,838/78 | + | 19 | Seamstress | L | + | Profession | ||
18 | 3,103/78 | + | 38 | Worker | L | + | FA-fracture/AO-PL | ||
19 | 983/80 | + | 48 | Housewife | L | + | Edema/TIS | ||
20 | 1,859/84 | + | 57 | Housewife | L | + | Anat. spec. feature | ||
21 | 1,958/84 | + | 70 | Retired | L | + | Intraneur. splinter | ||
22 | 2,921/84 | + | 45 | Carpenter | R | + | FA-fracture/AO-PL | ||
23 | 2,674/86 | + | 18 | Student | R | + | FA-fracture/nail | ||
24 | 2,796/86 | + | 46 | Hairdresser | R | + | Edema/TIS | ||
25 | 2,066/87 | + | 45 | Housewife | L | + | Edema/TIS | ||
26 | 730/88 | + | 33 | Examiner | L | + | FA-fracture/AO-PL | ||
27 | 1,799/88 | + | 47 | Draftsman | L | + | Anat. spec. feature | ||
28 | 11.11.89 | + | 66 | Retired | L | + | FA-fracture | ||
29 | 07.11.90 | + | 38 | Nurse | L | + | Anat. spec. feature | ||
30 | 13.09.90 | + | 49 | Housewife | L | + | Anat. spec. feature | ||
Table 3.2
PRKS – patient – population: N p (1969–1990) = 30, N op = 30. Follow-ups: 27a + (3b)
Age | (18–70) Ø 45 years |
Sex | 17m: 13 f |
Localisation (right:left) | 12:18 |
Triggering causes: | |
Occupation | 11 |
Upper arm fracture | 8 (sec. pareses) |
Upper arm osteitis | 2 |
Hand edema (TOS) | 4 |
Intraneural fragment | 1 |
Anatomical variety | 4 |
Radial nerve trauma: | |
Acute | 7 |
Chronic | 23 |
3.2 Surgically Relevant Anatomy and Physiology
Main areas for this kind of compression are the tendinous portion of origin of the triceps muscle lateral head, crossing the radial nerve directly in front of the lateral intermuscular septum (Fig. 3.2b), and the hiatus of the radial nerve. The latter functions as a relatively short osteofibrous channel, which can as an exemption also be supplemented by crossing fibrous strands running from the humeral shaft or the base of the brachial muscle to the septum (Fig. 3.3b).
Bosworth in 1971 already accepted the compression mechanism we described as explanation for the relatively frequent radial pareses in garbage workers. In the same year Lotem et al. (1971) confirmed PRKS, based on anatomic examinations and three patients treated conservatively. They also blamed a fibrous arcade of the lateral head of the triceps muscle as compressive cause (Bosworth DM, 1971, personal information).
The first surgical confirmation of PRKS was published by Manske (1977). Further publications are by Lubahn and Lister (1983), Wilhelm and Suden (1985), Wilhelm (1986), Mitsunaga and Nakano (1988), Nakamichi and Tschibana (1991) and Wilhelm (1993).
A partial or even a complete paralysis of the forearm muscles innervated by the radial nerve and disturbances of sensibility at the inferior lateral cutaneous brachii nerve, the posterior cutaneous antebrachii nerve and the superficial branch of the radial nerve can be the result (Fig. 3.2a). Irritations of the radial nerve at this site often result in pain radiation into the lateral epicondyle region (TE), into the extension side of the hand (posterior interosseous nerve neuralgia; Wachsmuth and Wilhelm 1967) and into the region of the radial styloid process (so-called radial styloiditis), summarised as radial irritation syndrome (RIS) (cf. Fig. 3.1; Wilhelm 1972, see references of Chap. 1).
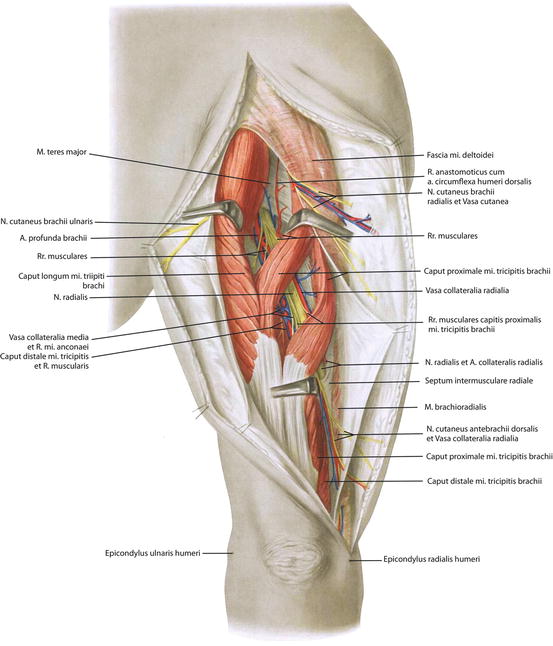
Fig. 3.1
Posterior brachial region and radial nerve channel. Tendon of lateral triceps muscle head obscured by muscles. (From von Lanz and Wachsmuth 1959)
The fibrous border of the radial nerve hiatus arcade is the next physiological bottleneck, sometimes narrowed even more by transverse fibrous strands of the septum (Fig. 3.3b). In this case there is also a pressure damage of the nerve and pain radiation into these regions without the supraepicondyle and posterior pain area, innervated by the lateral collateral branch of the radial nerve and the anconeus muscle branch. Disturbance of sensibility in this case is only found at the superficial branch of the radial nerve (Fig. 3.3a).
A further quite rare physiological narrowness is found at a fibrous band structure distal to the radial nerve hiatus, stretching between the bases of the brachial muscle and the lateral intermuscular septum of the humeral shaft in low height (Fig. 3.4a).
Myokinetic and sensitive disturbance corresponds to those in radial nerve hiatus compression.
Localisation of pressure damage is demonstrated in Table 3.3.
Table 3.3
PRKS: localisation of pressure damage
A. Triceps muscle lateral head | 13× |
B. Radial nerve hiatus | 10× |
C. Combination of A and B | 5× |
D. Localisation distal to the hiatus | 2× |
3.3 Epidemiology
Apart from the author’s statistics, there are no other significant publications on the subject; consequently at this point, no definite answer can be given concerning the frequency of PRKS. The occurrence of PRKS can be estimated indirectly, for example, by comparison to the supinator syndrome. This relation was 27:29 in favour of the supinator syndrome between the years 1968 and 1988. This result, however, does not allow for reliable conclusions concerning the prevalence.
Based on patient population, an average age of 45 years (18–70 years) and a preference of the male sex in a ratio of 17:13, as well as a side localisation of 12:18 in favour of the left arm, are seen.
Triggering factors are mainly occupational, acute and chronic overexertion of the triceps muscle in a ratio of 10:20 with special significance of favourable anatomic conditions and variations (Table 3.1).
3.4 Aetiology and Pathogenesis
The most essential triggering causes of PRKS have already been mentioned in the preceding sections and have been presented in Tables 3.1 and 3.2.
Four mechanisms of compression were found as the cause of PRKS.Related posts:
 The Controversial Pain Syndrome of the Shoulder Joint (So-Called Coracoiditis): Pathogenesis and Treatment of Resistant Cases
The Controversial Pain Syndrome of the Shoulder Joint (So-Called Coracoiditis): Pathogenesis and Treatment of Resistant Cases
 The Controversial Pain Syndrome of GE: Pathogenesis and Surgical Treatment of Resistant Cases
The Controversial Pain Syndrome of GE: Pathogenesis and Surgical Treatment of Resistant Cases
 The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases
The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases
 Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases
Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases
 Swimmer’s Headache
Swimmer’s Headache
 Cervical Facet Syndrome
Cervical Facet Syndrome

Full access? Get Clinical Tree


