(1)
Aschaffenburg, Germany
2.1 Introduction
Literature research was accomplished in 1962 as far as it was possible at that time. It was found until then obviously no relevant surgical procedure for the treatment of therapy-resistant “Epicondylitis humeri medialis” had been published. Hohmann in 1949 mentioned this localisation in the context of tennis elbow, especially in diagnostic aspect; he does not describe any relevant surgical procedure, however. In volume 10, part 1 of the Allgemeine und Spezielle Chirurgische Operationslehre, a corresponding presentation is missing as well (Wachsmuth 1956).
This fact surprises at first, but it becomes understandable taking into account how rarely golf elbow occurs. Thus, it was advisable to apply the principle of denervation also to the treatment of resistant golf elbow (GE), based on the already promising surgical results in tennis elbow (Wilhelm and Gieseler 1963).
2.2 Surgically Relevant Anatomy and Physiology
Golf elbow (GE), also called thrower elbow (Demmer and Rettig 1982), as a contrast to tennis elbow (TE) only causes slight functional impairment of the hand and is also characterised by a relatively small pain area. This is frequently limited to the peak and the entire circumference of the medial epicondyle. In severe cases also pain areas at the medial collateral ligament and the humeral forearm flexor region of origin, especially the pronator teres muscle, are found. Contrary to TE, where the pain region is solely innervated by fibres of the radial nerve, innervation of the corresponding region in GE is accomplished by branches arising from two main nerve stems, being the median nerve (C7–Th1) and the ulnar nerve (C6–Th1).
The innervation of the medial epicondyle region has already been extensively described by Wilhelm in 1958, 1963 and 1972. The innervation of the anterior pain area is mainly accomplished by the final median nerve fibres shown in Fig. 2.1 (right). These arise from recurrent muscle branches, innervating both portions of pronator teres muscle origin as well as of the flexor digitorum communis muscle. The pain-leading fibres can be seen up to the epicondyle peak and the medial collateral ligament. The cranial circumference of the medial epicondyle is innervated by a short branch, arising from both the median nerve and the musculocutaneous nerve. This branch innervates the periosteum below the distal fibres of the brachial muscle coming from the medial intermuscular septum. The peak of the medial epicondyle on the front side is additionally innervated by a delicate branch of a cutaneous nerve, the macroscopic innervation area of which is set off by a hatched area in Fig. 2.1 (right). This is a thin branch of 3 cm length escaping from the posterior branch of the cutaneous medial nerve of the forearm above the epicondyle and then separating dichotomically. The stronger branch runs subcutaneously towards the epicondyle peak separating in a bundle and innervating the anterior proximal area of the epicondyle peak. Shortly afterwards a stronger nerve strand separates, ending together with a little branch of the medial collateral artery above the epicondyle (Fig. 2.2).
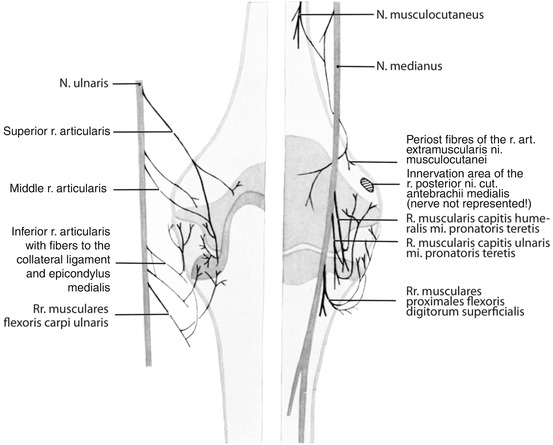
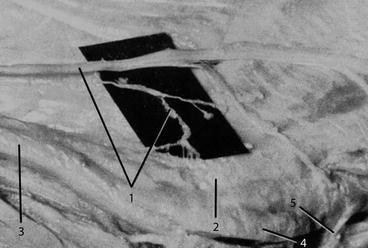
Fig. 2.1
Innervation of medial epicondyle region posterior and anterior, ulnar nerve drawn off. (From Wilhelm 1972)
Fig. 2.2
Preparation of medial epicondyle innervation 2 by a branch of the posterior medial cutaneous nerve of the forearm (1 and 2), 3 ulnar nerve, 4 epitrochleoanconeous muscle and 5 tendinous arch of ulnar flexor carpi muscle. (From Wilhelm and Gieseler 1963)
The posterior pain area of GE is exclusively innervated by articular and periosteum branches of the ulnar nerve (Fig. 2.1 left). According to Rüdinger (1857), three branches are possible. The upper joint nerve can have diverse strengths and already springs from the main stem several centimetres above the epicondyle, then reaching the anteromedial area of the triceps muscle medial head. Here it can already give a fine thread innervating the humeral capsule above the olecranon fossa. Afterwards the first articular branch is found slightly in front of the triceps muscle tendon with branches in the proximal section of the capsule, medial of the elbow. Figure 2.1 (left) as a variety shows a connection between the first and second articular nerve, together innervating the capsule area. The medial articular nerve usually is stronger and innervates the distal humeroulnar section of the capsule together with the main branch of the upper articular nerve. A fine fibre, coming directly from the ulnar nerve, might be distinguished between both articular branches, innervating the capsule in the immediate posterior area of the epicondyle massif. The lower articular branch arises either directly from the ulnar nerve or from the proximal ulnar branch, innervating the humeral head of the flexor carpi ulnaris muscle (FCU), with recurrent fibres reaching the collateral medial ligament and the distal medial section of the capsule.
In order to be complete, it has to be mentioned there is a collateral branch of the radial nerve on the medial side as well; it already escapes from the main stem in the axilla and soon afterwards has close connection to the ulnar nerve, breaking through the intermuscular medial septum together in posterior direction and running on the free surface of the triceps muscle medial head in distal direction, finally ending as an articular branch at the olecranon fossa. This branch, however, is not responsible for pain conduction in GE. This is also true for a posterior branch of the medial cutaneous antebrachii nerve, innervating the medial rim of the elbow and the capsular area in the immediate neighbourhood. This is why both nervous branches were not mentioned in Fig. 2.1 (left).
2.3 Epidemiology
Golf elbow (GE) is relatively rare. According to Nigst (1993), its frequency is 5–10 % compared to 90–95 % in tennis elbow. Median age is 43 (21–65) years (Vangsness and Jobe 1991). The authors regarded surgical therapy as necessary in 38 (11.4 %) out of 334 patients. Thirty-five follow-ups consisted of 32 males and 3 females. In 33 out of 35 patients, the symptom affected the dominant arm. Side distribution was 28:7 in favour of the right side. Depending on patient volume, the frequency of GE per year according to Vangsness and Jobe (1991) is 3.5 %; according to Schwarz et al., it is 1.4 %; and in our own patient population, it is 1.1 %.
2.4 Aetiology and Pathogenesis
Anamnestically patients mention occupational as well as leisure activities as exogenous causes of GE, leading to an overexertion of the muscles in the upper arm and the humeroulnar region. In professional life this can be caused either by an acute event, for instance, a sudden sticking fast of a pneumatic drill (so-called backlash injury), or by chronic stress in certain professional procedures, demanding continuous flexion and extension of the elbow joint, especially in combination with simultaneous pronation. A typical example is the ongoing service of the lever of a drill or a punching machine. This exertion can result in pressure damage of the ulnar nerve at its sulcus and the median nerve at the humeral trochlea, possibly also leading to pain radiation in the medial epicondyle region.
Patients with ulnar nerve irritation sometimes also report pain in both outer fingers, connected with the sensation of falling asleep and a certain loss of crude strength as well as precision movement. These symptoms are also found in an early proximal ulnar compression syndrome (PUKS), which is not surprising, as identical compression mechanisms cause PUKS and GE.
This also applies to the median nerve. In this case patients complain not only about pain in the cubital fossa and the medial epicondyle region but also about symptoms of an early pronator syndrome. Patients also report a deterioration of pain in the cubital fossa in strong grip. Numbness is minor, but reduction of strength is some stronger.
Still insertional tendopathies and degenerative tendon processes are held responsible as an endogenous precondition for GE. Anatomical, clinical and intraoperative findings as a contrast and finally the convincing postoperative results prove that the endogenous precondition in fact is a functionally caused pressure damage of median and ulnar nerve in various extents.
In sports exogenous causes are found in golf, as well as in javelin throw, discus throw, baseball, racketball, bowling, weight lifting, and cross-country skiing (Fulkerson 1980). Weight lifting deserves special interest with regard to pathogenesis. Especially in this discipline, Neugebauer saw (1974, quoted according to Machacek 1976) especially medial “epicondylitis” in 24 weight lifters 19 times altogether.
Promoters of a tendinogenous pathogenesis find a causal relation in pain of golf elbow and insertion tendinopathy or a degenerative process of the muscles coming from the medial epicondyle as result of a functional overexertion (Wirth 2007). The consequence of eliminating the pain by traction relief in shape of a tendon notch or of loosening the originating fibres is convincing at first sight. It was logical then to perform surgery of resistant GE also according to the Hohmann principle (1949). Machacek (1976) among others reported four successfully surgically treated patients, where “the muscle origins were loosened at the medial epicondyle down to the bone”. It was not mentioned, however, which muscles were involved.
A similar surgical procedure was also published by Vangsness and Jobe (1991), where after preparation of the epicondyle the common origin of the forearm muscles including the humeral head of the FCU is cut horizontally, loosened, sparing the medial collateral ligament and finally being replaced again. After drilling the epicondyle several times, the loosened forearm flexors are reinserted with several sutures in “length of relaxation” in order to reconstitute the normal muscle tension. Despite this controversial reinsertion, the authors report excellent results in 24 (69 %) out of 34 cases and good results in 10 patients (19 %). This is surprising and cannot be explained from the pathogenetic point of view, as the end of the procedure results in the original traction tension at the medial epicondyle. Again the question arises how pain relief was accomplished in 88 %. A transitory elimination of traction stress at the epicondyle cannot be the reason for the surgical success. If the extension of the corresponding pain area and its nervous supply by final fibres of the median nerve and the ulnar nerve is taken into account, only one explanation remains: an unconscious denervation. Here in loosening the anterior soft tissue flap not only the nerve fibres coming from the subcutis to the epicondyle and supraepicondyle are cut but also the pain conducting final fibres of the median nerve muscle branches, providing the supply for the humeroulnar muscles.
The significance of an exclusively neurogenous genesis of GE is supported by the following facts and conclusions:
1.
Anamnestic notes concerning exogenous causes of GE (cf. above): patients mainly report pain at the inner side of the elbow joint as main symptom, developing or deteriorating in motion of the elbow joint, especially against resistance, for example, in carrying a bag. In maximum extension of the elbow joint, for example, in playing golf and in carrying and lifting heavy weights, pain is reported as well. These pain radiations are also demonstrated by some patients (Fig. 2.15). Additionally minor pain radiation distally and proximally is reported as well as minor disturbance of sensibility and some impairment of crude strength and delicate motion.
2.
Maximum extension of the pain area does not only include the corresponding epicondyle region but also the humeroulnar muscle origin, being the pronator teres muscle, the flexor digitorum superficialis muscle and the humeral head of the FCU, including the medial collateral ligament.
3.
The anterior pain area apart from a periosteal fibre of the forearm medial cutaneous nerve posterior branch is mainly innervated by final fibres of median nerve muscular branches destined for the humeral origins of the pronator teres muscle and the superficial finger flexor muscle (Fig. 2.1 right). These structures can be confirmed by a corresponding nerve blockade, at the same time localising the pain area.
4.
As early as 1963, “neuro-irritation impulses” have been discussed as cause of anterior pain radiation, transferred by the median nerve, the causes remaining obscure, however. Systemic clinical and intraoperative examinations of the median nerve and its proximal myokinetic branches have shown a predominant localisation for irritations in the proximal area of the cubital fossa. This was confirmed in 7 out of 12 surgically treated GE of this series, supporting that also in GE there are pain radiations caused by further proximal nerve irritation. In the remaining five patients, the cause was finally supposed to be in the area mentioned above.
5.
A median nerve and myokinetic branches pressure damage of minor degree (irritation!) at the humeral trochlea, caused by direct pressure of the bicipital aponeurosis in 5 out of 12 patients is responsible for the anterior pain radiation (Figs. 2.16 and 2.17). In these cases after resection of the bicipital aponeurosis, a protruding and broadened median nerve with parallel fascicles and missing subepineural blood flow at the humeral trochlea is found in extension of the elbow joint, so also a disturbance of the intraneural flow can be concluded in both remaining cases, clinically initially also presenting as a compression syndrome of the bicipital aponeurosis. The main cause was a pressure damage by a fascia bridge of several cm, lying deep and being tense, connecting the pronator teres muscle and the brachial muscle, as well as disturbing the median nerve in its side movement (Figs. 2.18, 2.19, and 2.20). After resection of this fascia, there is a severe disturbance of blood flow and a slight broadening of the nerve diameter and in one case even a circumscribed loosening of the epineurium, as well as a stronger notch. In extension of the elbow joint, the results of this compressing fascial plate are evident (Figs. 2.18, 2.19 and 2.20).
6.
As the bicipital aponeurosis spreads into the forearm fascia, in contraction of the biceps muscle, a certain functional tension band wiring effect develops, pushing a contracted pronator teres muscle stronger against the humeral trochlea and the brachial muscle above. As a result, also the median nerve and its motoric branches suffer from additional pressure, as shown in two patients. This finding supports the technique of always resecting the bicipital aponeurosis in decompression of the median nerve. A neural irritation by a supracondylar process or by a Struther ligament was not seen in this series.
7.
The posterior pain area, including the origin of the flexor carpi ulnaris humeral head and the medial collateral ligament in contrast to the anterior area, is exclusively innervated by fibres of the three articular branches of the ulnar nerve (Rüdinger 1857) (Fig. 2.1 left) and can be extinguished, as well as identified by blocking this nerve 2 cm proximal to the epicondyle peak. On demand, the subcutaneous posterior branch of the cutaneous medial nerve of the forearm can be blocked from here as well. Routine blocks like this are not necessary in GE and TE contrary to wrist denervation.
8.
Locally, apart from pressure pain, in some cases limited to the peak of the epicondyle, an ulnar nerve sensitive to pressure pain in increase of passive flexion radiating pain in the direction of the epicondyle, sometimes down to the small finger, is found. Slight hypaesthesia can be noticed in this area. Identical symptoms are found in the flexion test of the elbow joint in proximal ulnar compression (PUKS).
9.
In pathogenetic aspect of pain radiation to the posterior part, the following endogenous causes are found as predisposing factors: in a normal grooved sulcus of the ulnar nerve (Fig. 2.3), the nerve is found dorsal of the elbow joint axis, thus permanently experiencing traction and pressure stress in articular flexion, caused and at the same time caught by the epicondyle mass. Hereby in changing pressure and extension of the joint, the nerve experiences a continuous change of its diameter, resulting in repeated shifting of individual fascicles, change of nerve pressure and traction stress as well as a recurrent medial shift of the nerve. This can even be supported by the effect of the short triceps muscle head. These irritations lead to disturbances of nervous blood flow and axonal flow, basically responsible for pain radiation and the change in surface sensitivity. In a normal epicondyle, there can still be a tendency towards luxation if the ulnar nerve in increasing flexion finds its hypomochlion in the distal area of the epicondyle circumference, at this point moving into a more or less obtuse angle into the trochlea (Güney et al. 1977).
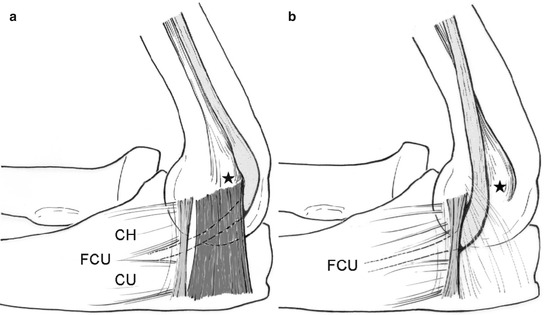
Fig. 2.3
Presentation of ulnar nerve luxation mechanism. (a) Proximal compression syndrome in subluxation (Wachsmuth and Wilhelm 1968). (b) Distal compression in luxation (Osborne 1957). Asterisk medial epicondyle, yellow ulnar nerve with pseudoneuroma, red epitrochleoanconaeus muscle, orange tendinous arch of FCU, CH humeral head, CU ulnar head. (From Suden and Wilhelm 1987, with kind permission from Thieme)
10.
Main causes of GE in endogenous aspect are dysplasia of medial epicondyle and quality of roof above the ulnar nerve sulcus. Whether there is subluxation or luxation of the ulnar nerve depends on the ulnar nerve sulcus roof stability. This is accomplished either by the atavistic epitrochleoanconaeus muscle, first described by Gruber (1866), bridging the sulcus in diagonal direction, innervated by a branch of the ulnar nerve, or by its ligamentary rudiment, being the epitrochleoanconaeus ligament. The rudimentary character of this ligament is supported by the fact that it can contain transverse muscle fibres, corresponding to the fibre flow of the epitrochleoanconaeus muscle. According to anatomic research, this muscle is found in 17.9–28.7 %, according to clinical findings in 9–17.3 % (Table 2.1). Intraoperatively the muscle was found in 9.0–17.3 % (Table 2.2). The epitrochleoanconaeus muscle and its ligamentary rudiment come from the medial epicondyle mass and connect to the opposite olecranon circumference between articular capsule and final tendon fibres of the triceps muscle medial head (Figs. 2.3 and 2.5). The epitrochleoanconaeus muscle and the ligament develop a rhombic shape in articular extension, whereas in increase of flexion a trapezoid shape develops, due to change of distance and transposition of the points of origin and insertion. At the same time a significant extension of these structures up to one third is accomplished, as seen in Fig. 2.4, leading to a very strong tension of the proximal muscular and ligamentary rim, whereas only a slight lengthening is seen at the distal rim (Fig. 2.6). The epitrochleoanconaeus muscle is innervated by a branch coming from the ulnar nerve together with the upper articular branch (Fig. 2.2) (Wachsmuth and Wilhelm 1968). Mummenthaler (1961) described the tension of the epitrochleoanconaeus ligament, possibly “leading to a compression of the nerve in the sulcus itself”; in this context, the author also elaborates that “the nerve is more or less compressed between the descending triceps and the ulnar epicondyle”.
Table 2.1
Epitrochleoanconaeus muscle: anatomic findings
Authors | Preparations | Cases | % |
|---|---|---|---|
Gruber (1866) | First description | ||
Kudo a. Li (1956) | 472 | 85 | 18.0 |
Mummenthaler (1961) | 56 | 10 | 17.8 |
Bando (1979) | 157 | 45 | 28.7 |
Table 2.2
Epitrochleoanconaeus muscle: clinical findings
Authors | PUKS | M. epitr. | % | |
|---|---|---|---|---|
1. James | ? | 1 | – | |
2. Wachsmuth a. Wilhelm | ? | 5 | – | |
3. Vanderpool | 1968 | ? | 2 | – |
4. Kojima et al. | 44 | 4 | 9.0 | |
5. Nigst | 1983 | 338 | 31 | 9.3 |
6. Own patient population | 1962–1969 | ?
Related posts: The Controversial Pain Syndrome of the Shoulder Joint (So-Called Coracoiditis): Pathogenesis and Treatment of Resistant Cases The Controversial Pain Syndrome of the Shoulder Joint (So-Called Coracoiditis): Pathogenesis and Treatment of Resistant Cases
 The Controversial Pain Syndrome of Proximal Radial Compression Syndrome (PRKS): Pathogenesis and Surgical Treatment of Resistant Cases The Controversial Pain Syndrome of Proximal Radial Compression Syndrome (PRKS): Pathogenesis and Surgical Treatment of Resistant Cases
 The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases The Controversial Pain Syndrome of Tennis Elbow (TE): Pathogenesis and Surgical Treatment of Resistant Cases
 Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases Controversial Pain Syndrome of M. Sudeck (RSD, CRPS I): Pathogenesis and Surgical Treatment of Resistant Cases

Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|