The United States is one of two countries in the Organisation for Economic Cooperation and Development (OECD) that do not offer health coverage to all of its citizens (Mexico is the other one).16 Although the elaborate patchwork of public and private coverage options works well for many of those who have employer-sponsored health benefits or who are eligible for public programs, it has many holes. While nearly all of the elderly are eligible for Medicare, 15% of individuals younger than 65 years are not covered by employment-based health insurance, are not eligible for Medicaid or other public programs, and are left uninsured.17 The resulting uninsured population was 41.3 million in 2013.17
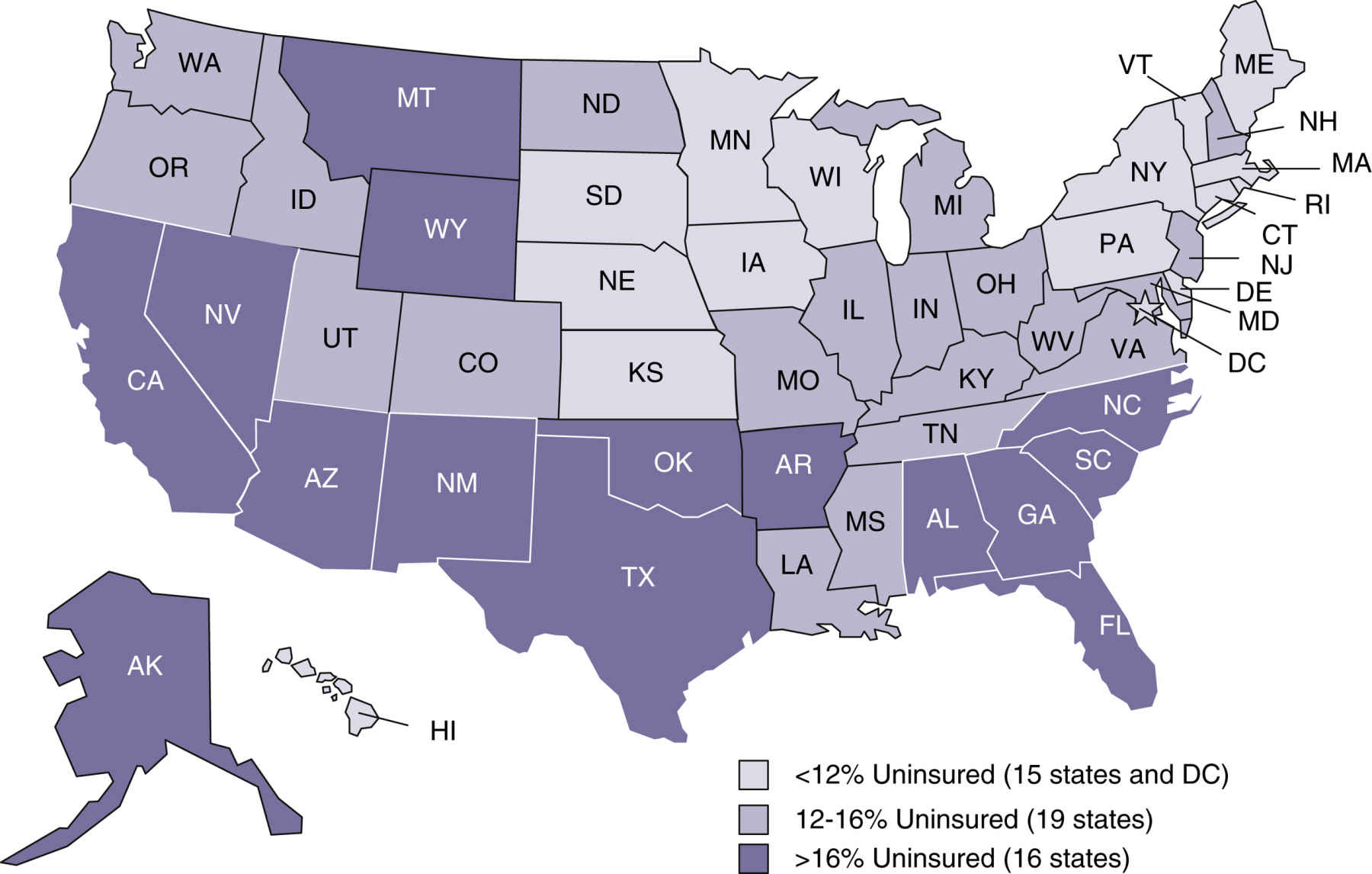
From 2010 to 2012, the percentage of uninsured young adults (ages 19 to 25) dropped from 48% to 41%, mostly likely resulting from the PPACA’s requirement that children under age 26 be permitted to stay in or join a parent’s health plan.17 The uninsured rates for other age groups increased or stayed the same during the same time period (Fig. 6.1). Noncitizens (legal and undocumented) are approximately threefold more likely to be uninsured than citizens.17 Insurance rates vary across states because of differences in average income, employment opportunity, and Medicaid policy at the state level (Fig. 6.2). Massachusetts has an uninsured rate of less than 5%, whereas the rate exceeds 20% in Nevada, Florida, and Texas.17
Having no health insurance negatively affects the financial condition, health-seeking behavior, and health outcomes of the uninsured. Two out of five uninsured adults reported having problems paying medical bills or having accrued medical debt, nearly twice the rate of the insured population.18 Because they have to pay medical bills out of pocket, the uninsured are inclined toward delaying or skipping needed health care. More than two thirds of adults who were uninsured experienced one or more of the following: failing to fill a prescription; skipping a medical test, treatment, or follow-up visit; choosing not to see a doctor when sick; or not seeing a specialist because of cost.18 Emergency department services are often the only option for the uninsured when medical care is unavoidable. The uninsured are more likely to be in poor health than the insured. Uninsured adults were more than twice as likely to report being in fair or poor health as those with private insurance.19
Moreover, 31 million, or 23% of insured people between the ages of 19 and 64 years, were underinsured (out-of-pocket costs or deductibles amounted to 5% or more of their household incomes) in 2014. Similar to the uninsured, half of underinsured adults reported problems with medical bills or debt and two out of five reported skipping needed care because of cost.20
Health Care Workforce
A capable and motivated health care workforce is essential to achieve national health goals. The health care industry is the largest employer in the nation. More than 12 million people worked in this enterprise in 2014.21 Major categories of health care professionals include physicians, dentists, registered nurses, licensed practical nurses (LPNs), pharmacists, health services administrators, and allied health professionals (Table 6.1). In addition, millions more work in health-related industries to produce supplies, capital goods, and services for people providing direct patient care.
Physicians are central to the delivery of health care services. They are responsible for the evaluation, diagnosis, and treatment of patients. Even as insurance companies and health care organizations create incentives to influence the preferences of patients and the practice patterns of physicians, physicians still exert enormous power in controlling and directing the use of medical inputs in the production of health care services. Those wishing to practice allopathic medicine must get a 4-year undergraduate degree and a doctor of medicine (MD) degree from an accredited medical school, pass a series of U.S. Medical Licensing Examination tests offered by the National Board of Medical Examiners, and complete a supervised residency program. Physicians must be licensed by every state in which they practice. Those who wish to further specialize in areas such as cardiology or pediatric surgery must complete a fellowship beyond the residency and typically sit for specialty board examinations to achieve voluntary board certification. Similar requirements exist for practitioners of osteopathic medicine (i.e., doctor of osteopathic medicine).
Table 6.1
Selected Health Care Employment and Corresponding Wages
Data from CDC/National Center for Healthcare Statistics: Table 96. Healthcare employment and wages, by selected occupations: United States, selected years 2001–2013 (website). www.cdc.gov/nchs/data/hus/2014/096.pdf. Accessed May 26, 2015
Physicians can be grouped into generalists and specialists. Generally speaking, physicians trained in general internal medicine, pediatrics, and family medicine are considered to be primary care physicians. Primary care physicians provide services to meet the routine needs of patients such as health maintenance, initial diagnosis, and continuing treatment of common illness. Physicians who have additional training to practice in a medical specialty are referred to as specialists. Typical specialties include anesthesiology, subspecialties of internal medicine, surgical subspecialties, obstetrics and gynecology, dermatology, ophthalmology, and psychiatry.
Once they are licensed, physicians can start their own solo practice, join a group practice, or accept a position as an employee of a health care organization. The former path has become less popular in recent years because of the capital required to start a private practice, the financial pressure on physician owners, and the burden of marketing and managing the practice. Although most physicians practice in office-based settings, an increasing number of physicians choose to become hospitalists whose primary professional focus is the general medical care of hospitalized patients.22 Hospitalists function as primary care providers in the inpatient setting, coordinating care provided by specialists and other health care personnel.23
Nurses are major caregivers for patients. In addition to supporting care for patients, nurses are the leading force in conducting case management, utilization review, quality assurance, and patient education. Advanced practice nurses (APNs)—clinical nurse specialists, nurse anesthetists, nurse-midwives, and nurse practitioners—assume relatively independent responsibilities for more complicated patient services for primary care as well as in acute care settings.
To practice, a nurse must be licensed by a state’s board of nursing. Licensure requires graduation from an approved nursing program and the completion of a national examination. Nurses have varying degrees determined by different educational paths. Registered nurses must have a baccalaureate degree in nursing (BSN) offered by a college or university, an associate degree in nursing (ADN) obtained from a community or junior college, or a diploma from an approved hospital nursing program. LPNs or licensed vocational nurses (LVNs) must complete a state-approved training program in practical nursing. This program usually takes 1 year. The 2010 IOM report, The Future of Nursing: Leading Change, Advancing Health, recommends an increase in the proportion of nurses with baccalaureate degrees to 80% by 2020.24 Currently, APNs must have a minimum of a master’s degree with a requirement from the American Association of Colleges of Nursing that the APN have a doctorate of nursing practice (DNP) as a minimum educational level by 2015. The DNP is designed for nurses seeking a terminal degree in nursing practice and offers an alternative to research-focused doctoral programs. The practice doctorate is the graduate degree for advanced nursing practice preparation, including but not limited to the four current APN roles previously mentioned. The majority of nurses work in hospitals. A large proportion of nurses also work in the offices of physicians, home health care services, and nursing care facilities. Many nurses have sought careers in other fields such as insurance companies, emergency medical centers, worksites, schools, government agencies, and social assistance agencies. Some nurses pursue a PhD and are research scientists.
Major Medical Services
There are three major types of medical services: outpatient services, inpatient services, and long-term care (LTC). Outpatient medical services consist of diagnostic and therapeutic services that do not require an overnight stay in a health care facility. In 2013, it is estimated that 47.0% of the population had one to three visits to hospital emergency departments, doctor offices, or home visits by a clinician in the past year, while 37.2% had four or more visits.25 In terms of service volume, there were 126 million visits to hospital outpatient departments and 136 million visits to hospital emergency departments in 2011.25
Advances in medical and surgical technology enable increasingly more inpatient services such as surgical procedures, rehabilitative therapies, renal dialysis, and chemotherapy to be performed in outpatient settings. Pressure from payers to reduce medical expenses also promotes the use of ambulatory care settings as alternatives to expensive inpatient care. Currently, as many as 70% of all surgeries are performed in ambulatory settings.26 Outpatient services can be rendered in physicians’ offices, hospital outpatient departments, hospital emergency departments, freestanding ASCs, medical laboratories, hospice facilities, and through home health agencies in the patient’s home. The number of Medicare-certified ASCs increased from 1460 to 5364 between 1991 and 2013 although the growth rate has slowed down recently.27,28
Inpatient services refer to medical services received during one or more overnight stays in a health care facility. These services include room and board, physician services, inpatient pharmacy, skilled nursing care, rehabilitation services, and ancillary services such as imaging and laboratory services. The use of inpatient services per capita has declined over the years. In 2013, 6.7% of the population had one or more hospital stays in the past year. By contrast, 7.8% of the population had one or more hospital stays in 1997.25 The length of a hospital stay declined sharply after the CMS adopted a prospective payment system for reimbursing hospital care in 1983. This system pays a fixed amount for each case in the same diagnosis-related group regardless of the actual days spent in the hospital or services used. The average length of stay in community hospitals was 5.4 days in 2012 compared with 7.6 days in 1980.25
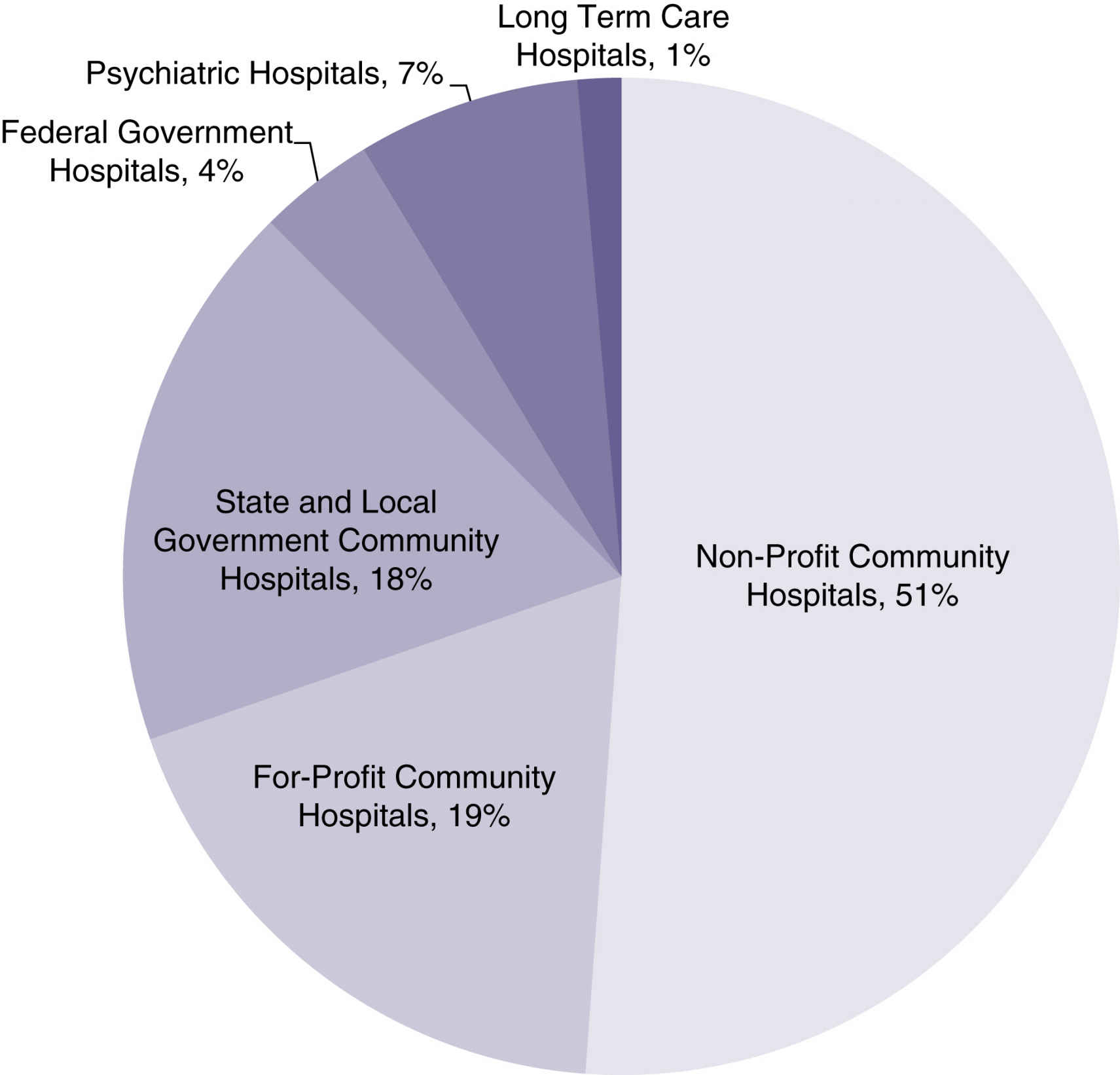
Hospitals are the major source of inpatient services. There were 5686 hospitals in the United States in 2013 (Fig. 6.3). Of these, 4974 were nonfederal, community, short-term hospitals with an average patient stay of less than 30 days.29 Other types of hospitals serve special population subgroups, including federal hospitals, long-term hospitals, psychiatric hospitals, and hospital units of institutions (e.g., prison hospitals, college infirmaries).
Hospitals can be classified into three main groups by ownership structure: public hospitals, nonprofit hospitals, and for-profit hospitals. Public hospitals are owned by the federal, state, or local government. Federal hospitals serve specific populations such as Native Americans, veterans, or military personnel and their dependents. State hospitals usually focus on providing mental health services. Public hospitals operated by county, city, and sometimes state governments tend to be community hospitals that are open to the general public. These hospitals usually serve a large proportion of Medicaid and uninsured patients.
FIG. 6.3 Proportion of hospitals by type of hospital, 2013. (From the American Hospital Association: Fast facts on U.S. hospitals (website). www.aha.org/research/rc/stat-studies/fast-facts.shtml. Accessed May 28, 2015.)
Approximately half of the hospitals in the nation are private, nonprofit hospitals. They are owned by local communities or other nongovernmental organizations and operated on a nonprofit basis. Nonprofit hospitals can earn surpluses or accounting profits (i.e., an excess of revenues over expenses), but they may not distribute surpluses to any private shareholder or individual. Nonprofit hospitals receive a tax exemption from federal income tax and are often exempt from local property taxes. They also have access to charitable donations that are tax deductible for donors, and they can also use tax-exempt bond financing.
An increasing number of hospitals are operated as for-profit organizations. In 2000, there were 749 for-profit community hospitals. In 2012, the number increased to 1068.25 These hospitals are typically owned by national or regional health systems; fewer are freestanding facilities. For-profit hospitals operate at a relatively smaller scale. The average number of beds among for-profit hospitals was 126 in 2012 compared with 188 beds for nonprofit hospitals.25
With the aging of the population, LTC services delivered to patients with physical or mental disabilities are increasingly important. LTC recipients can be elderly individuals with Alzheimer disease, strokes, complications of diabetes, or visual impairments. Young people with permanent or temporary disabilities may also need LTC. Individuals needing LTC services have varying degrees of difficulty in performing some ADLs or instrumental ADLs without assistance. Instrumental ADLs include more complicated tasks such as preparing food, housekeeping, and handling finances.
Nursing homes are the most common providers of LTC. There were 15,663 certified nursing homes with 1,697,484 beds in 2013. The average occupancy rate was 80.8%.25 LTC can also be provided by assisted living facilities, home health agencies, or family members and other informal caregivers in various noninstitutional settings. A study by the U.S. Department of Health and Human Services estimated that people who reach age 65 have a 40% chance of entering a nursing home. Among those entering a nursing home, approximately 10% will stay there for 5 years or more.30 Most of the nursing homes are for-profit entities owned by multifacility chains.
Governments’ Role in Health Care
Federal, state, and local governments are deeply involved in every aspect of the health care system. Government intervention mainly takes four forms: (1) commodity taxes and subsidies (e.g., government at several levels imposes taxes on tobacco to discourage smoking, and the federal government offers tax credits to employers who provide health benefits to their employees); (2) direct provision (the federal government provides medical care to Native Americans, veterans, and military personnel and their dependents); (3) transfer programs (e.g., Medicaid as discussed in the previous section); and (4) regulation (e.g., state licensure of health care professionals).31 This section discusses the responsibilities of the federal, state, and local governments with an emphasis on their role as regulators.
Role of the Federal Government
The federal government’s duty is to protect the health of all Americans and to provide essential human services as executed by the U.S. Department of Health and Human Services. Departmental leadership is provided by the Office of the Secretary, which is directly supported by the Deputy Secretary, Chief of Staff, and a number of assistant secretaries, staff offices, and operating divisions. The 11 operating divisions include eight agencies within the U.S. Public Health Service and three human services agencies. In the Public Health Service Division, the National Institutes of Health, the Food and Drug Administration, and the Centers for Disease Control and Prevention are the primary federal agencies that conduct research and establish regulations aimed at protecting the health and safety of the U.S. population. CMS is the federal agency that administers Medicare, Medicaid, and CHIP (the latter two are administered jointly with the states). To achieve better efficiency and improve the overall quality of care, CMS has taken significant steps toward a strategy that links payment to health care providers’ performance. For example, after October 1, 2008, CMS ceased to pay for a series of hospital-acquired conditions (“never events”) that are deemed avoidable in most cases through the application of evidence-based guidelines.32 One of these “never events” is surgical site infection after certain surgical procedures. The CMS payment policy, which is often adopted by private payers and state governments, imposes financial pressure on health care organizations to redesign the process of care and also requires every health worker to change clinical practices and follow recommended quality guidelines more closely.
Only gold members can continue reading. Log In or Register to continue