Chapter 10 The ASA Difficult Airway Algorithm
Analysis and Presentation of a New Algorithm*
I Introduction
The original ASA DAA was developed over a 2-year period by the ASA Task Force on Guidelines for Management of the Difficult Airway.1 The task force included academicians, private practitioners, airway experts, adult and pediatric anesthesia generalists, and a statistical methodologist. The algorithm was introduced by ASA as a practice guideline in 1993. In 2003, the ASA task force presented a revised algorithm that essentially retained the same concept but recommended a wider range of airway management techniques than was previously included, based on more recent scientific evidence and the advent of new technology.
II the ASA Difficult Airway Algorithm
A side-by-side comparison of the original (1993) and the updated (2003) versions of the ASA DAA is presented in Figure 10-1. The differences between the two algorithms are listed in Box 10-1. Certain aspects of the algorithm require further explanation.
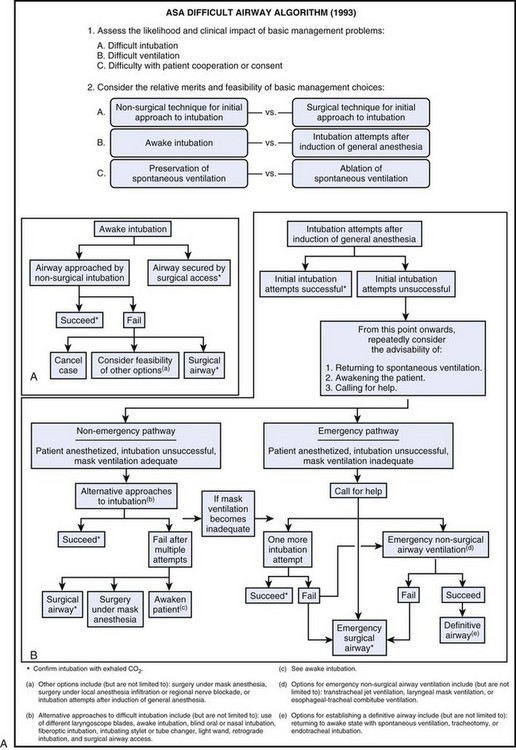
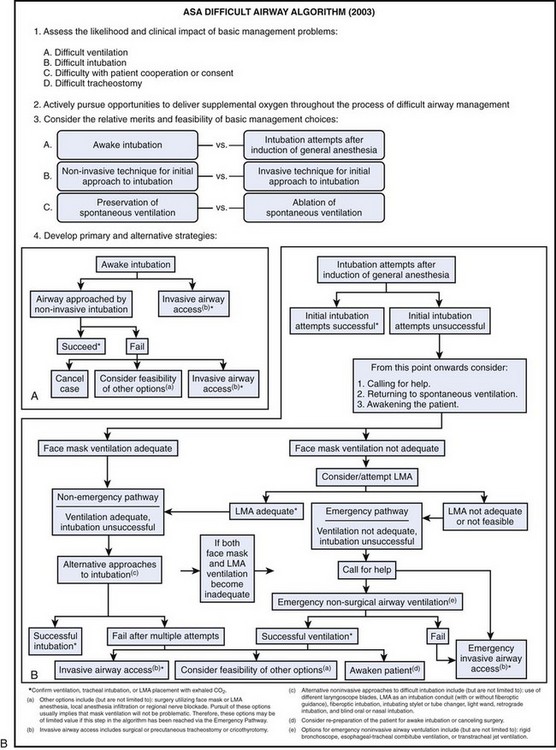
Box 10-1 Differences between 1993 and 2003 ASA Management of the Difficult Airway Algorithms
1. Difficult ventilation is now listed first under item 1, “Assess the Likelihood and Clinical Impact of Basic Management Problems.” Also, in the same category, Difficult tracheostomy was added.
2. A new item 2 was inserted: “Actively pursue opportunities to deliver supplemental oxygen throughout the process of difficult airway management.”
3. When considering the relative merits and feasibility of basic management choices (item 3), awake intubation versus intubation attempts after induction of anesthesia should now be considered first, before noninvasive versus invasive techniques as the initial approach to intubation.
4. Use of the laryngeal mask airway (LMA) was incorporated into the algorithm in the awake induction limb and in both the nonemergency and emergency pathways for induction after general anesthesia (either as a ventilatory device or as a conduit for tracheal intubation).
5. The option for “One more intubation attempt” was removed.
6. Use of the rigid bronchoscope was added as an option for emergency noninvasive ventilation.
A Patient Evaluation and Risk Assessment
The ASA DAA begins with the most basic question of whether or not the presence of a DA is recognized (see Chapter 9). Recognizing the potential for difficulty leads to proper mental and physical preparation and an increased chance of a good outcome. In contrast, failure to recognize this potential results in unexpected difficulty in the absence of proper mental and, likely, physical preparation, with an increased chance for a catastrophic outcome.
Airway evaluation should take into account any characteristics of the patient that could lead to difficulty in the performance of (1) bag-mask or supraglottic airway ventilation, (2) laryngoscopy, (3) intubation, or (4) a surgical airway. Routine patient evaluation can be best structured as follows (see Chapter 9 for details):
1. Obtain an airway history to identify medical, surgical, and anesthetic factors that may indicate the presence of a DA.
2. Evaluate for systemic diseases (e.g., respiratory failure, coronary artery disease) that might place limits on awake intubation, such as increased fraction of inspired oxygen (FIO2), or require special attention, such as prevention of sympathetic nervous system stimulation.
3. Examine previous anesthetic records, which can yield useful information about previous airway management.
4. Conduct a physical examination of the airway to detect physical characteristics that might indicate the presence of a DA (Table 10-1):
TABLE 10-1 Components of the Preoperative Airway Physical Examination
| Airway Examination Component | Nonreassuring Findings |
|---|---|
| Length of upper incisors | Relatively long |
| Relation of maxillary and mandibular incisors during normal jaw closure | Prominent “overbite” (maxillary incisors anterior to mandibular incisors) |
| Relation of maxillary and mandibular incisors during voluntary protrusion of the jaw | Patient’s mandibular incisors anterior to (in front of) mandibular incisors |
| Interincisor distance | <3 cm |
| Visibility of uvula | Not visible when tongue is protruded with patient in sitting position (e.g., Mallampati class III or IV) |
| Shape of palate | Highly arched or very narrow |
| Compliance of mandibular space | Stiff, indurated, occupied by mass, or nonresilient |
| Thyromental distance | <3 ordinary finger breadths |
| Length of neck | Short |
| Thickness of neck | Thick |
| Range of motion of head and neck | Patient cannot touch tip of chin to chest or cannot extend neck |
The findings of the airway history and physical examination may be useful in guiding the selection of specific diagnostic tests and consultation to further characterize the likelihood or nature of the anticipated airway difficulty.2
B Difficult Bag-Mask Ventilation
The risk for difficult mask ventilation (DMV) is the first issue addressed in the most recent version of the DAA. Evidence from the literature3 suggests that the incidence of DMV is 5% in the general adult population, that the presence of DMV is associated with difficult intubation, and that DMV is not accurately predicted by anesthesiologists.
Five independent criteria predict DMV (age >55 years, body mass index >26 kg/m2, lack of teeth, presence of mustache or beard, and history of snoring), and the presence of two such risk factors indicates a high likelihood of DMV.3 It is important to keep these risk factors in mind, because some of them can be reversed. For example, DMV may possibly be preventable by shaving a patient’s beard, leaving dentures in place during bag-mask ventilation (BMV), and performing a workup and treating for possible obstructive sleep apnea.
C Awake Tracheal Intubation
Awake intubation is generally more time-consuming for the anesthesiologist and a more unpleasant experience for the patient. However, if a difficult intubation is anticipated, awake endotracheal intubation is indicated for three reasons: (1) the natural airway is better maintained in most patients when they are awake (i.e., “no bridges are burned”); (2) the orientation of upper airway structures is easier to identify in the awake patient (i.e., muscle tone is maintained to keep the base of the tongue, vallecula, epiglottis, larynx, esophagus, and posterior pharyngeal wall separated from one another)4,5; and (3) the larynx moves to a more anterior position with the induction of anesthesia and paralysis, which makes conventional intubation more difficult.6
Crucial to the success of endotracheal intubation while the patient is awake is proper preparation (see Chapter 11 for further details). Most intubation techniques work well in patients who are cooperative and whose larynx is nonreactive to physical stimuli. In general, the components of proper preparation for an awake intubation are the following:
• Psychological preparation (awake intubation proceeds more easily when the patient knows and agrees with what is going to happen)
• Appropriate monitoring (i.e., electrocardiography, noninvasive blood pressure monitoring, pulse oximetry, and capnography)
• Oxygen supplementation (e.g., nasal prongs, nasal cannula, suction channel of a fiberoptic bronchoscope [FOB], transtracheal catheter)7–10
• Vasoconstriction of the nasal mucous membranes (if performing nasal intubation)
• Administration of a drying agent
• Judicious sedation (keeping the patient in meaningful contact with the environment)
• Adequate airway topicalization (consider performance of bilateral laryngeal nerve blocks, blocking the lingual branch of the glossopharyngeal nerve and the superior laryngeal nerve)
• Aspiration prevention (see Chapter 12)
Box 10-2 lists the suggested ASA guidelines for contents of a portable airway management cart.11
Box 10-2 Suggested Contents of the Portable Storage Unit for Difficult Airway Management
1. Rigid laryngoscope blades of alternative design and size from those routinely used; may include a rigid fiberoptic laryngoscope
2. Endotracheal tubes of assorted sizes
3. Endotracheal tube guides, such as semirigid stylets, ventilating tube changer, light wands, and forceps designed to manipulate the distal portion of the endotracheal tube
4. Laryngeal mask airways (LMAs) of assorted sizes; may include the Fastrach intubation LMA and the ProSeal LMA (LMA North America, San Diego, CA).
5. Fiberoptic intubation equipment
6. Retrograde intubation equipment
7. At least one device suitable for emergency nonsurgical airway ventilation, such as the esophageal-tracheal Combitube (Tyco Healthcare, Mansfield, MA), a hollow jet ventilation stylet, and a transtracheal jet ventilator
8. Equipment suitable for emergency surgical airway access (e.g., cricothyrotomy)
9. An exhaled carbon dioxide detector
There are numerous methods to intubate the trachea or ventilate a patient (see Part Four of this text). Box 10-3 shows a list of the techniques contained within the ASA guidelines. The techniques chosen depend, in part, on the anticipated surgery, the condition of the patient, and the skills and preferences of the anesthesiologist. Based on recent evidence from the literature12–14 considerations should also include the use of video laryngoscopy, despite the fact that this technique is not mentioned in the recent ASA algorithm, but likely will be included in future revisions of the guidelines.
• Surgery may be canceled (e.g., the patient needs further counseling, airway edema or trauma has resulted, different equipment or personnel is necessary).
• General anesthesia may be induced (the fundamental problem must be considered to be a lack of cooperation, and mask ventilation must be considered nonproblematic).
• Regional anesthesia may be considered (careful clinical judgment is required to balance risks and benefits; see Chapter 45).
• A surgical airway may be created (if the surgery is essential and general anesthesia is considered to be inappropriate until intubation is accomplished); this may be the best choice to secure the airway in patients with laryngeal or tracheal fracture or disruption, upper airway abscess, or combined mandibular-maxillary fractures.
D Difficult Intubation in the Unconscious or Anesthetized Patient
All of the intubation techniques that are described for the awake patient1,15 can be used in the unconscious or anesthetized patient without modification. However, direct laryngoscopy and fiberoptic laryngoscopy are likely to be more difficult in the paralyzed, anesthetized patient compared with the awake patient, because the larynx may move to a more anterior position, relative to other structures, as a result of relaxation of oral and pharyngeal muscles.6 In addition and more importantly, orientation may be impaired because the upper airway structures can coalesce into a horizontal plane instead of separating out in a vertical plane.4,5
In the anesthetized patient whose trachea has proved difficult to intubate even with a video laryngoscope it is necessary to try to maintain gas exchange between intubation attempts (by mask ventilation) and, whenever possible, during intubation attempts through the use of (1) supplemental oxygen11; (2) positive-pressure ventilation via an anesthesia mask that incorporates a self-sealing diaphragm for entry of the FOB airway intubator (instead of the standard oropharyngeal airway)5,16; or (3) a laryngeal mask airway (LMA; LMA North America, Inc., San Diego, CA) as a conduit for the FOB (see Chapters 19 and 22).17
One must not continue with the same technique that did not work before. The amount of laryngeal edema and bleeding is likely to increase after every intubation attempt, particularly with the use of a laryngoscope or retraction blade. The most common scenario in the respiratory catastrophes in the ASA closed claims study was the development of progressive difficulty in ventilating by mask between persistent and prolonged failed intubation attempts. The final result was inability to ventilate by mask and provide gas exchange (see Chapter 55).18
For each additional attempt, consider modifications, such as improved sniffing position, external laryngeal manipulation, a new blade or new technique, or involvement of a much more experienced laryngoscopist. However, the number of intubation attempts should be limited and the following options should be considered: (1) awaken the patient and do the procedure another day; (2) continue anesthesia by mask or LMA ventilation; (3) perform a surgical airway (tracheostomy or cricothyrotomy) before the ability to ventilate the lungs by mask is lost (see Fig. 10-1).
• Immediately apply Trendelenburg position.
• Turn the head, and perhaps the body, to the left.
• Suction the mouth and pharynx with a large-bore suction device.
• Try endotracheal intubation while the patient is in the lateral position (the tongue may be more out of the way, but this position is unfamiliar to most anesthesiologists).
• If the endotracheal tube (ETT) has been passed into the esophagus, it may be left there; this may allow decompression of the stomach, and it identifies the esophagus during subsequent intubation attempts (the disadvantage is that it interferes with satisfactory mask seal).
• After securing the airway, consider tracheal suctioning, mechanical ventilation, positive end-expiratory pressure, fiberoptically guided saline lavage, steroids, antibiotics (see Chapter 35).
E The “Cannot Intubate, Cannot Ventilate” Scenario
The development of the LMA was a major advance in the management of difficult intubation and difficult ventilation scenarios. The LMA is suggested as a ventilation device or a conduit for a flexible FOB,19,20 and the Fastrach intubating LMA (ILMA) may also be utilized.10,17,21 The LMA and the Combitube are supraglottic ventilatory devices and are not helpful if the airway obstruction is located at or below the glottic opening.22 Use of the rigid bronchoscope may be required to establish a patent airway because it allows ventilation even past an obstruction at these levels. If immediately available, TTJV is relatively easy to perform and can be life-saving.23 However, it carries significant risks such as subcutaneous emphysema (if the upper airway is not patent or the catheter is not entirely tracheal) and barotrauma (too forced ventilation or proximal airway obstruction)24 The techniques mentioned can provide time until definitive airway management by tracheal intubation (via direct, fiberoptic, or retrograde technique) or by formal tracheostomy can be performed.25,26 Future research will determine the role of the new rigid video laryngoscopes in the rescue of the “cannot intubate, cannot ventilate” scenario.
Ultimately, a cricothyrotomy may be necessary, but fewer than 50% of anesthesiologists feel competent to perform one.27 Nevertheless, when one is faced with a failed airway, preparations for a surgical airway must begin immediately, and once the decision is made, it is essential to use an effective technique (see Chapters 30 and 31). Despite limited familiarity with the procedure, the risks of an invasive rescue technique must be weighed against the risks of hypoxic brain injury or death.28
F Extubation of a Patient with a Difficult Airway
• Awake extubation versus extubation before return of consciousness
• Clinical symptoms with the potential to impair ventilation (e.g., altered mental status, abnormal gas exchange, airway edema, inability to clear secretions, inadequate return of neuromuscular functions)
• Airway management plan if the patient is not able to maintain adequate ventilation
• Short-term use of a ventilating tube exchanger (TE) or jet stylet (can be used for ventilation and guided reintubation)
The ideal method of extubation of a patient with a DA is gradual, step by step, and reversible at any time. Extubation over a ventilating TE or jet stylet closely approximates this ideal.16 The equipment that should be immediately available for the extubation of a DA includes that necessary for intubation of the DA (see Chapter 50).29
G Follow-up Care of a Patient with a Difficult Airway
• Description of the airway difficulties, which should distinguish between difficulties with mask ventilation and those with tracheal intubation
• Description of the airway management techniques used, which should indicate the beneficial or detrimental role of each technique in management of the DA
• Information given the patient (or responsible person) concerning the airway difficulty that was encountered. The intent of this communication is to assist the patient (or responsible person) in guiding and facilitating the delivery of future care. The information conveyed may include, for instance, the presence of a DA, the apparent reasons for the difficulty, and implications for future care.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


