Chapter 52 Teaching Airway Management Outside the Operating Room
I Background
Management of the airway is the most important and potentially the most life-saving (or life-threatening) task that an anesthesiologist, emergency department (ED) physician, or intensivist performs. Missteps in airway management can result in mortality or significant morbidity. In 1985, the American Society of Anesthesiologists (ASA) Committee on Professional Liability began to analyze closed-claim malpractice cases to objectively assess adverse outcomes from anesthesia. The initial analysis of the data, published in 1990, revealed that respiratory events accounted for 34% of the claims (522/1541 cases) and that 85% of the respiratory events resulted in permanent neurologic injury or death.1 Three mechanisms of adverse outcome from respiratory events accounted for 73% of the events: inadequate ventilation (38%), esophageal intubation (18%), and difficult endotracheal intubation (DI; 17%).
The reviewers concluded that 90% of the cases of inadequate ventilation and esophageal intubation could have been prevented if monitoring with capnography and pulse oximetry had been employed. It was also concluded that only 36% of the cases of DI were easily preventable. In response to this finding, the Task Force on Management of the Difficult Airway (DA) was formed by the ASA. After an exhaustive search and evaluation of the medical literature concerning airway management published between 1973 and 1991, the task force published Practice Guidelines for Management of the Difficult Airway in March, 1993.2 These guidelines included recommendations for evaluation of the airway, basic preparation for DA management, strategy for intubation of the DA, and postoperative care. The Task Force also developed an algorithm for management of the DA. Updated guidelines, based on information accrued since 1993, were published in 2003.3 It can be anticipated that future updates based on experience with new airway devices will occur.4 Other organizations with interest in airway management have also published airway management guidelines.5
A Is There Evidence That the Difficult Airway Guidelines Have Been Effective in Reducing Adverse Airway Events?
A review of the closed claims database in 1999 revealed a decline in claims for adverse respiratory events, primarily related to a reduction in claims for inadequate ventilation and esophageal intubation.6 Claims for adverse events secondary to DI remained relatively constant, and claims for trauma to the upper airway increased. The claims for pharyngeal and esophageal trauma were frequently associated with DI. Another study, published in 2005, compared claims for DA management during two time periods: 1985–1992 (before DA guidelines) and 1993–1999 (after DA guidelines). Claims for adverse respiratory outcomes (death or brain death) during induction of anesthesia decreased by 67% during the latter period compared with the former. However, claims for similar adverse respiratory outcomes occurring during the maintenance phase of anesthesia, at extubation, or during recovery did not change.7
Although respiratory events are more likely to result in an adverse outcome, the incidence of patients with a DA in clinical anesthesia practice is actually quite low. The incidence of failure to intubate the trachea in a large series of surgical patients was only 0.3%.8 Although the most comprehensive published data have concerned perioperative airway management, airway management in the prehospital setting, in the ED, and in the intensive care unit (ICU) is no less important and must be included in any airway education program.9 Airway management is not an easy skill to learn, and educators must give careful consideration to the complexity of airway management and the ability of different types of health care providers to manage ventilation and endotracheal intubation.
Objectives for education in airway management include the theoretical and practical aspects of airway devices and techniques and a time-based environment that mimics actual clinical situations. The student must also gain an appreciation of the relationship between the practitioner and the patient and the effects that clinical decisions may have on outcome.10 The teaching program must allow the learner in a nonclinical environment to make choices that may result in an adverse outcome.
II Miller’s Learning Pyramid
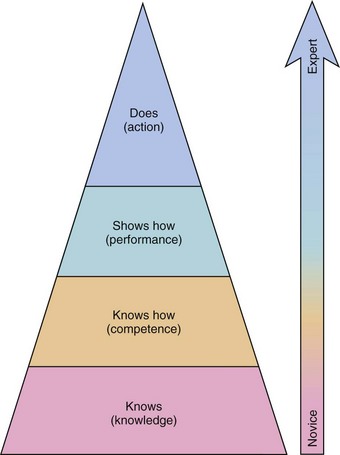
An airway teaching program must teach simple maneuvers (e.g., performing a jaw thrust) as well as complex skills such as awake fiberoptic intubation (FOI). The design of a successful education program begins with the development of clear objectives. What has to be taught, to whom, and how? The program must also address different knowledge and skill levels. Miller’s learning pyramid for assessment of clinical skills has four stages of ability: Knows, Knows How, Shows How, and Does (Fig. 52-1).11
Because skills and scientific information gained during simulator training may not be easy to transfer directly to clinical practice, the clinical environment is the best environment for developing airway management skills.12 Practicing techniques such as airway assessment, bag-mask ventilation (BMV), supralaryngeal airway (SLA) insertion, direct laryngoscopy, and FOI in actual patients would be ideal. The highest competence level (Does) in airway management ultimately requires practice in the clinical environment. There are, however, a number of barriers to training exclusively in the clinical arena (Box 52-1). Training outside the operating room (OR) or ICU is done to minimize the risk to patients and promote efficient clinical learning.
Box 52-1 Barriers to Teaching Difficult Airway Management in the Clinical Environment
III Computer-Based Learning
The pace of development of interactive computer-assisted instructional programs has surpassed simulation development over the past 10 years. Computer-assisted instruction can facilitate the organization and linkage of information directly applicable to clinical situations.13 A major advantage of computer-based instruction is the low cost after development and the lack of need for a human instructor. The learner can use the program at his or her own pace and as many times as necessary to achieve mastery of the subject. The increased power of laptop computers has reduced the need for computer centers and provides the learner with exceptional mobility. Computer-assisted instruction can also provide alternative learning methods for students who do not learn well with traditional teaching methods.
A clinical department can develop its own instructional programs or access existing programs via the Internet. The number of Web sites relevant to anesthesia continues to grow, and the Internet provides rapid access for users in remote locations.14 However, Internet programs are not peer-reviewed, and quality can be variable.15 The transition from Web 1.0 to Web 2.0 has encouraged more interactivity and improved the quality of Web-based education.16 The disadvantages of Web-based education, such as insufficient feedback and instructional ambiguity, can be overcome by providing local faculty input to supplement the Web-based program.
There are several objectives of an interactive airway management program (Box 52-2). One is to familiarize the learner with the anatomy and physiology of the upper airway. The complexity of the upper airway is often overlooked, and understanding of upper airway function can provide an early warning of impending respiratory difficulty. The structure and function of various airway devices can be displayed with diagrams, photographs, and videotapes. Computer-based multimedia programs can demonstrate device function and technique with a much more effective presentation than a traditional lecture format.
Box 52-2 Instructional Components of an Airway Management Educational Program
IV Efficacy of Simulation in Education
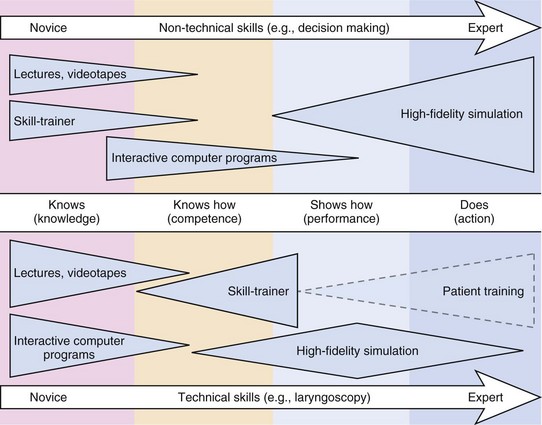
Simulation has been used for decades to address training problems in high-risk disciplines such as military science and aviation. Medical simulation began in the mid-1990s and has grown rapidly.17 Simulator training programs incorporate psychomotor and decision-making skills that address the highest level of competence in Miller’s pyramid: Does. When the programs are appropriately designed, simulation can close the gap between acquisition of skills and meaningful use of the acquired skills (Fig. 52-2). This may be especially true for rare situations. Because the incidence of the DA is low in clinical practice, two questions must be addressed: How can an anesthesiologist in clinical practice learn new airway skills? and How can the ramifications of critical decision points in airway management be learned?
The inherent nature of airway management includes uncertainty, complexity, time pressure, and high costs for failure. Simulation provides the ideal method for closely replicating the clinical situation and may help to scientifically evaluate strategies, decision points, and algorithm adherence.18,19 The efficacy of education with medical simulation is well established, but its effect on reducing the incidence of adverse patient outcomes is more controversial.18,20–24 It is easy to prove the effect of a theoretical lecture or workshop with a pretest and post-test. It is not easy to prove the effect of simulation on patient outcome in rare but life-threatening situations such as the DA. Nevertheless, there is evidence in the literature that simulator- and scenario-based training improves patient care.
V Types of Simulators
Simulators can be classified as low-fidelity (static) or high-fidelity (dynamic).
A Low-Fidelity Simulators
Mannequins do not always accurately replicate human anatomy and cannot be altered to represent abnormal anatomy. Such low-fidelity simulators provide neither physiologic data nor clinical feedback for the learner. Despite these shortcomings, however, effective skill transference to clinical use may be facilitated.25
B High-Fidelity Simulators
High-fidelity simulators, more commonly referred to as human patient simulators, offer many advantages over low-fidelity simulators. Physiologic parameters such as blood pressure, heart rate, pulse oximetry, capnography, breath sounds, peripheral pulses, and temperature can be programmed into the simulator. High-fidelity simulators cannot accommodate the variations in human anatomy.26 This is especially true for DI scenarios in which insertion of an SLA may be clinically effective. The reason is that the DI scenario in the simulator is created by supraglottic obstruction rather than laryngeal displacement.
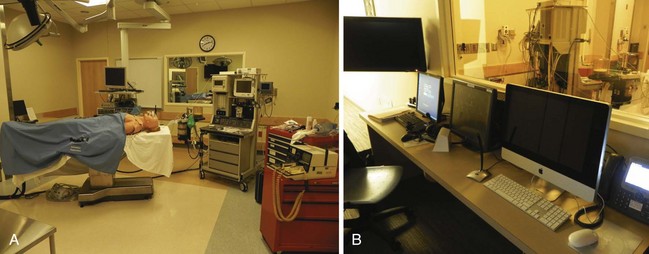
Many medical institutions and health care consortiums have invested in multipurpose simulation centers to provide training for different types of health care providers. These centers replicate ORs, ICU beds, ward beds, examination rooms, and ambulance bays to provide a realistic setting for trainees (Fig. 52-3). Simulation centers can employ full-time technicians to manage the technical aspects of simulation. This allows the teaching faculty to concentrate their efforts on curriculum development and the direction of simulation sessions.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Ultrasonography in Airway Management
Ultrasonography in Airway Management
 Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation
Nonintubation Management of the Airway: Airway Maneuvers and Mask Ventilation

Full access? Get Clinical Tree


