Sympathetic nerve supply
Target organs
Splanchnic nerves
Stomach, duodenum, jejunum, ileum, pancreatic head, proximal colon, kidneys, proximal ureters
Celiac plexus
Stomach, duodenum, jejunum, ileum, pancreas, proximal colon, spleen, gall bladder, liver
Superior hypogastric plexus
Distal colon, bladder, uterus, vagina, cervix, prostate, testes, urethra
Inferior hypogastic plexus
Distal colon, urinary bladder, penis, vagina, rectum, anus, perineum
Ganglion impar
Coccyx, cervix, distal rectum, perineum, prostate, sigmoid colon, distal urethra, vulva, scrotum, distal vagina
Splanchnic Nerve Block
Anatomy and Related Structures
The greater, lesser, and least splanchnic nerves arise from preganglionic fibers which course through the crura of the diaphragm before synapsing in the celiac ganglion. Cadaveric studies have revealed that the greater splanchnic nerves originate between T5 and T10, while the lesser splanchnic nerves arises from T9 to T10, and the least splanchnic nerves from T11 to T12. Interventional approaches target these nerves at T11 and T12 when the nerves are in close proximity to the vertebral body (Fig. 15.1). The splanchnic nerve block offers the ability to both avoid the celiac artery and selectively interrupt transmission before the splanchnic nerves reach the celiac plexus [5].
Fig. 15.1
Both the splanchnic and celiac nerve blocks can be performed via a dorsal approach. The sympathetic chain courses in a cranial-caudad direction and transmits the greater, lesser, and least splanchnic nerves which can be blocked at the level of the T11 and T12 vertebral bodies. The celiac plexus lies anterior to the abdominal aorta and is comprised of a complex meshwork of nerves surrounding the celiac and superior mesenteric arteries
At the level of the lower thoracic vertebral bodies, the splanchnic nerves have a predictable course bordered laterally by the pleura, ventrally by the posterior mediastinum, medially by the thoracic vertebral bodies, and dorsally by the pleural attachments to the vertebra. Additionally, this location is amenable to radiofrequency neurotomy for those patients who experience temporary, but non-sustained relief with local anesthetic blocks [6–8].
Indications
The splanchnic nerve block can be performed for a wide variety of malignant and non-malignant pain conditions arising from the stomach, pancreas, small bowel, proximal large bowel, kidneys, and proximal ureters.
Interventional Approach
Since the splanchnic nerve block was initially described, the technique has evolved with respect to the amount of fluoroscopic obliquity used, the needle chosen, the level of the block, and the type and volume of injectate.
A dorsal approach performed under fluoroscopy can be accomplished by positioning the patient prone and identifying the T11 and T12 vertebral bodies using radiographic imaging. After squaring the vertebral end plates and introducing a 10- to 15-degree ipsilateral oblique fluoroscopic angle, the junction of the ribs and the vertebral body will become visible. This junction marks the skin entry point for both the T11 and T12 levels (Fig. 15.2). Following aseptic preparation of the injection site, a local anesthetic skin wheal is created and a 22 or 25 gauge spinal needle is advanced coaxially hugging the lateral aspect of the mid-portion of the T11 or T12 vertebral body. The needle trajectory should course along the mid-portion of the vertebral body to avoid inadvertent entry into the disc or illiciting paresthesia along the nerve root. A cross-table lateral fluoroscopic image will reveal the needle advancing ventrally to lie at the middle third of the T11 vertebral body (Fig. 15.3). Two milliliters of radio-opaque contrast demonstrates spread posterior to the aorta and anterior to the foramen (Figs. 15.4 and 15.5). A diagnostic (and potentially therapeutic) unilateral or bilateral block of the greater, lesser, and least splanchnic nerves can be performed with 2 mL of injectate, such as 0.5 % bupivacaine, via a single injection. This volume is thought to be sufficient to block all three splanchnic nerves, though the technique can be modified by introducing a second needle at the T12 level and employing a smaller volume of injectate. Because of the proximity to the pleura, the final needle position should not extend beyond the anterior third of the vertebral body.
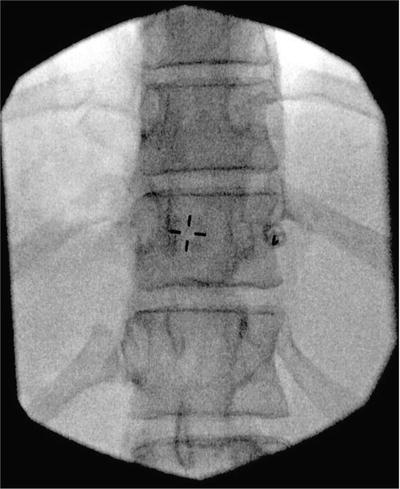
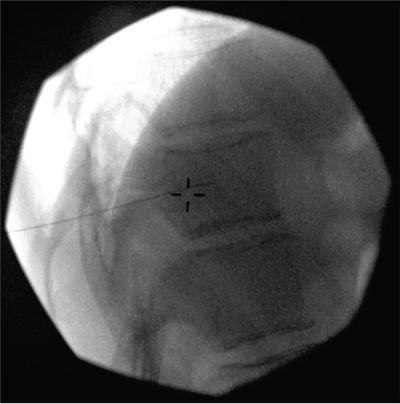
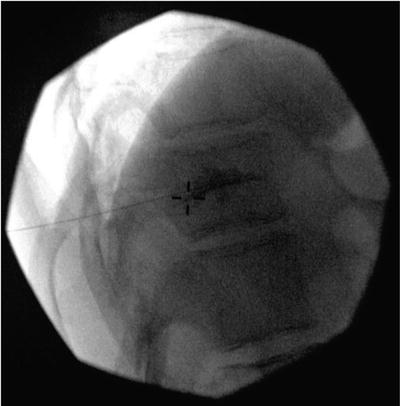
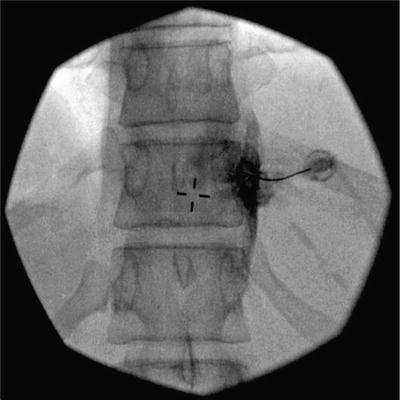
Fig. 15.2
Splanchnic nerve block. This anterior–posterior radiograph shows the needle advancing ventrally along the midpoint of the vertebral body to avoid contact with the spinal nerves and preventing penetration of the intervertebral disc
Fig. 15.3
Splanchnic nerve block. A cross-table lateral fluoroscopic image will reveal the needle advancing ventrally to lie at the middle third of the T11 vertebral body
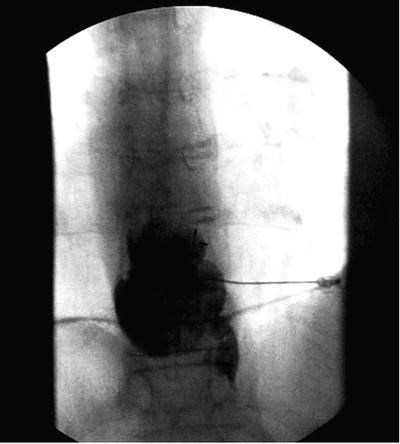
Fig. 15.4
Splanchnic nerve block. Contrast is seen hugging the vertebral body along the course of the splanchnic nerves. A small volume injectate targets the greater and lesser splanchnic nerves at the level of the T11 vertebral body. Performing the injection at the T12 level will target the least splanchnic nerve
Fig. 15.5
Splanchnic nerve block. Contrast is seen hugging the vertebral body. A large volume injection at T11 can spread caudally to cover the least splanchnic nerve obviating the need to perform the block at the T12 level. A similar approach to the paired splanchnic nerves would be carried out on the contralateral side
Choice of Injectate
Boas quantified the volume of the area bounded by the crura and the vertebral body to total 10 mL on each side and this represents a reasonable maximum injectate volume [1]. Local anesthetics, neurolytic agents, and steroids have all been used alone or in combination when performing the splanchnic nerve block. No randomized controlled trials have demonstrated the superiority of a single agent or combination agents over another [9].
When considering radiofrequency ablation, we advocate increasing specificity by performing at least one diagnostic block at both the T11 and T12 levels with a small volume of injectate which best approximates the size of the radiofrequency lesion.
Complications
Similar to the celiac plexus block, diarrhea, transient back pain, and hypotension may result from the splanchnic nerve block. Additional risks include subarachnoid or epidural injection, vascular or intradiscal injection, pneumothorax, chylothorax, and retrothoracic hematoma. Phenol neurolysis of the splanchnic nerves has generated reports of cardiac dysrhythmia and diaphagramic paralysis, thus favoring radiofrequency ablation as the preferred method of neurolysis.
Celiac Plexus Block
Anatomy and Related Structures
Surrounding the origin of the celiac and superior mesenteric arteries from the abdominal aorta lies the confluence of the splanchnic, parasympathetic, and sensory nerve fibers collectively termed the celiac plexus (Fig. 15.1). Neural blockade at the celiac plexus is not specific to sympathetic fibers, instead involving multiple types of fibers that course through the ganglion. For this reason, patient response to celiac block may vary from the response to the splanchnic nerve block.
Indications
The celiac plexus block, like the splanchnic nerve block, can be performed for a wide variety of malignant and non-malignant pain conditions arising from the stomach, small bowel, pancreas, proximal large bowel, kidneys, and proximal ureters. It is perhaps best characterized as an accepted technique for malignant pain arising from pancreatic cancer. A large meta-analysis demonstrated that when celiac neurolysis is utilized for patients with pancreatic cancer, 90 % of patients report sustained pain relief at three-month follow-up [1, 2, 5, 10–12].
Technique
Nearly a dozen interventional techniques have been described by way of dorsal or ventral approaches, employing endoscopic ultrasound, fluoroscopy, CT, or MRI. Surgical approaches have also been described and include thorascopic and open approaches via laparotomy [13–23].
The celiac plexus can be approached with relative ease via a dorsal transaortic approach. Whereas once this technique was performed primarily with fluoroscopy, CT-guidance is gaining widespread acceptance due to the fact that this can identify anatomic variations, particularly those that develop with cancer progression [24].
After positioning the patient prone and visualizing the left L1 transverse process, a skin wheal is created approximately 6 cm to the left of midline. A 22 gauge spinal needle is then advanced ventrally avoiding the transverse process and coursing adjacent to the mid-portion of the L1 vertebral body. If the vertebral body is encountered, the needle should be redirected ventrally or “walked-off” employing rotation of the bevel. When the needle passes the anterior border of the body of L1, the stylete is removed and the needle is advanced under continuous aspiration until the appearance of pulsatile heme is evident suggesting an intra-aortic position. The needle is then advanced further until a change in resistance is again noted suggesting passage through the anterior wall of the aorta and the aspiration of heme is no longer possible. Some use a saline-filled syringe to appreciate the change in resistance as the anterior wall of the aorta is penetrated. Injection of 3 mL of radio-opaque contrast demonstrates cranio-caudal spread and excludes vascular uptake (Figs. 15.6 and 15.7).

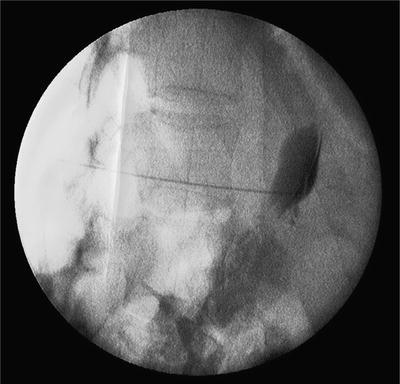
Fig. 15.6
Celiac plexus block. In the transaortic approach, the spinal needle is seen after having advanced through the aorta with contrast spreading anterior to the great vessels
Fig. 15.7
Celiac plexus block. A cross-table lateral image demonstrates the cranio-caudal spread of contrast anterior to the great vessels when approaching the celiac plexus with a transaortic approach
Aortic puncture can be avoided via a similar dorsal approach. Upon identification of the L1 vertebral body, a skin wheal is introduced over an entry point corresponding to the lateral fluoroscopic aspect of both the left and right L1 transverse processes. A 22 gauge spinal needle is then introduced in a similar manner to the transaortic approach and advanced to terminate just beyond the anterior aspect of the L1 vertebral body behind the posterior wall of the aorta. 3 mL of radio-opaque contrast material is injected confirming precrural contrast spread and the injectate volume is increased to augment the ventral spread of local anesthetic by gravity. If the contrast spread is unilateral as visualized by an antero-posterior fluoroscopic image, the procedure often needs to be repeated via an identical approach on the contralateral side of the L1 vertebral body. Increasing the volume of injectate is one approach to account for anatomic variations in the take-off of the celiac artery along the cranio-caudal axis if the procedure is performed with fluoroscopy rather than CT.
Complications
Similar to the splanchnic nerve block, diarrhea is an expected outcome of the procedure; thus we recommend indicating this possibility as part of the informed consent. Reported complications include retroperitoneal abscess, bowel perforation, aortic wall dissection, aortic pseudoanyerism, and paraplegia. The transaortic route is not recommended in patients with aortic aneurisms or calcifications in proximity to the area of aortic puncture [25].
Superior Hypogastric Plexus Block
Anatomy and Related Structures and Indications
The superior hypogastric plexus contains sympathetic fibers that innervate the distal colon, bladder, uterus, vagina, cervix, prostate, testes, and urethra. The plexus is a paired structure located ventral to the L5–S1 disc space and medial to the bifurcation of the common iliac arteries (Fig. 15.8). Malignant and non-malignant pain arising from these organs is amenable to a superior hypogastic block if the pain condition is entirely, or in part, maintained by sympathetic transmission [1, 2, 4, 26–28].
Fig. 15.8
The superior hypogastric plexus, inferior hypogastric plexus, and ganglion impar blocks can be performed via a dorsal approach. The paired sympathetic chains extend into the pelvis and coalesce at the ganglion impar. The superior hypogastric plexus lies anterior the L5–S1 disc space. The inferior hypogastric plexus is located along the ventral aspect of the sacrum at the level of the S2 foramen. The ganglion impar is ventral to the located at the sacrococcygeal junction
Interventional Approaches
Several approaches to the superior hypogastric plexus have been identified. Plancarte first described a posterior approach that involves needle entry at the level of the L4–L5 disc space coursing caudally toward the anterior body of the L5 vertebral body. After positioning the patient prone on a procedure table, the L4–L5 disc space is identified via an anterior–posterior view. Following aseptic preparation of the injection site, a skin wheal is created over the needle entry site 5 cm from midline at the level of the L4–L5 disc. A 22 G spinal needle is then inserted through the skin wheal directed toward the midline with a 30-degree caudal and 45-degree medial angle to contact the lateral aspect of L5. Upon contact with the vertebral body, the needle should be walked off ventrally and a lateral fluoroscopic image will demonstrate the needle tip in front of the L5 vertebral body. A change in resistance will be noted with advancement of the needle 1 cm anterior to the vertebral body as the tip passes through the anterior aspect of the psoas muscle. Injection of 3 mL of radio-opaque contrast material will spread along the midline with anterior–posterior fluoroscopy and along the anterior psoas fascia via a lateral fluoroscopic view (Figs. 15.9 and 15.10). Radiofrequency neurotomy can be performed in a similar manner.
 Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
 Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
 Peripheral Nerve Stimulation for Chronic Abdominal Pain
Peripheral Nerve Stimulation for Chronic Abdominal Pain
 The Epidemiology of Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain



Related posts:
Gastroparesis: Pathophysiology of Chronic Abdominal Pain and Current Treatment
Chronic Abdominal Pain of Gynecologic Causes: Diagnosis and Treatment
Gastric and Other Visceral Stimulation for Chronic Painful Gastrointestinal Motility Disorders
Establishing Diagnosis of Chronic Abdominal Pain: Gastroenterologist View
Peripheral Nerve Stimulation for Chronic Abdominal Pain
The Epidemiology of Chronic Abdominal Pain
Full access? Get Clinical Tree
