A. Stellate Ganglion Block
Nashaat N. Rizk
Cheryl D. Bernstein
 Patient Position:
Patient Position: Supine, with a roll placed under the shoulders to extend the neck.
 Indications:
Indications: Diagnosis and treatment of sympathetically mediated pain of the face, neck, and upper extremity; treatment of postherpetic neuralgia of the cervical dermatomes.
 Needle Size:
Needle Size: 25-gauge precision Glide needle.
 Medication/Volume:
Medication/Volume: 5 to 10 mL of 0.25% bupivacaine.
 Anatomic Landmarks:
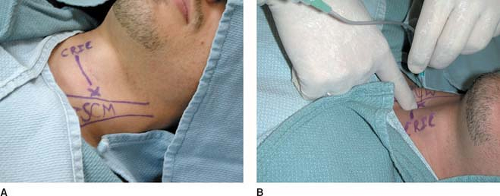
Anatomic Landmarks: Stellate ganglion, which is composed of the fusion of C7 and T1 sympathetic ganglia, which lies anterior to the transverse process of C7 and T1 on the anterior surface of the longus colli muscles, lateral to the trachea and esophagus, anteromedial to the vertebral artery, and medial to the common carotid artery. The block is performed lateral to the cricoid cartilage at the level of the C6 transverse process (Chassaignac tubercle)
(Fig. 63-1A).
 Approach and Technique:
Approach and Technique: Prepare the skin with a sterile solution lateral to the cricoid cartilage. Insert the needle perpendicular to the skin plane approximately one fingerbreadth lateral to the cricoid cartilage to make contact with the C6 transverse process
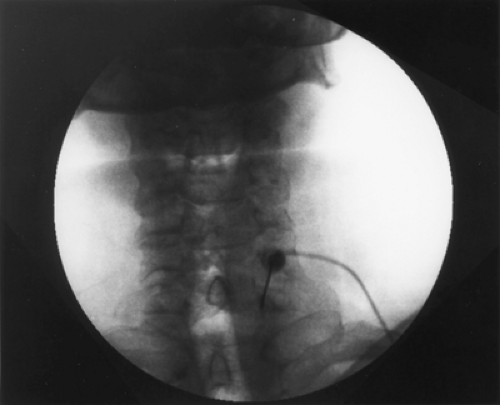
(Fig. 63-1B). After negative aspiration, inject 0.5 mL of 0.25% bupivacaine test dose. After the negative aspiration and the injection of a test dose, inject the remaining 5 to 10 mL of 0.25% bupivacaine. Under fluoroscopy, insert the needle at the junction of the transverse process and the C7 vertebral body
(Fig. 63-2). Use 2 mL of Isovue-200 (Bracco Diagnostics, Princeton, NJ) for verification of needle position.
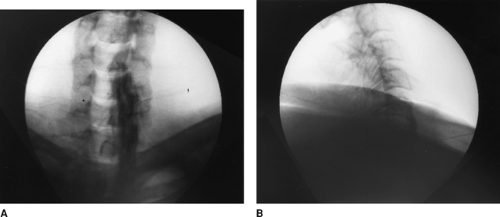
Figure 63-3 presents an anteroposterior
(A) and lateral view
(B).
 Complications:
Complications: Bleeding, infection, intravascular injection, pneumothorax, hoarseness and dysphagia, and epidural, subdural, or subarachnoid injection.
 Tips
Tips
Application of routine monitors, including blood pressure and pulse oxygen, is required.
Having the patient’s mouth slightly open decreases skin tension and facilitates palpation of the landmarks.
To avoid the risk for aspiration, the patient should avoid oral intake for 4 to 6 hours after the block and then resume with clear liquids as tolerated.
B. Celiac Plexus Block (Anterocrural)
Nashaat N. Rizk
 Patient Position:
Patient Position: Prone.
 Indications:
Indications: Abdominal pain associated with malignancy. Nonmalignant abdominal pain (controversial).
 Needle Size:
Needle Size: 22-gauge Quincke type, 178-mm.
 Medication/Volume:
Medication/Volume: For diagnostic purposes: 15–20 cc of bupivacaine 0.5%, lidocaine 2%, or ropivacaine 0.5%. For neurolysis: 10–15 cc of alcohol 50–100% or phenol 6.5%.
 Anatomic Landmarks:
Anatomic Landmarks: At T
12-L
1, the celiac plexus lies anterior to the aorta. Traditionally, a single-needle technique is used on the left side.
 Approach and Technique:
Approach and Technique: Fluoroscopy is used to take an anterior–posterior (AP) view and mark the T12-L1 junction
(Fig. 63-4A). The beam is oblique to hide the ipsilateral transverse process (left side) behind the shadow of the upper third of the L
1 vertebral body. A slight cephalad–caudad tilt of the beam may be necessary to square the endplates. This point should be marked and is approximately 6–8 cm from midline. After skin wheal and deep infiltration of local anesthetics, advance the needle parallel to the x-ray beam. Of great importance is taking frequent AP views to assess needle direction and lateral views
(Fig. 63-4B) to assess depth. Once the anterior third of the vertebral body is reached, the stylet is removed from the needle and 0.1 cc–0.2 cc of PFNS is injected to occupy the needle and prevent air embolization. Once the aorta is pierced, very gentle aspiration is continuously applied until negative aspiration for blood. Advance 2–3 mm. Inject a small amount of the dye. Injection should be very slow and you should not feel any resistance. Resistance to injection may indicate injection in the wall of the aorta and may cause dissection. Injection of the local anesthetic should commence after desirable AP
(Figs. 63-4D and E) and lateral
(Figs. 63-4C and F) views are obtained with adequate propagation of the dye without intravascular runoff. Following the local anesthetic, absolute alcohol is injected slowly. Needle tip is about 1½ -2cm anterior to the vertebral body. The same is done on the right side, stopping just anterior to the vertebral body.
If splanchnic blocks are to be done, the needle tip should not be deeper than the anterior third of the vertebral body.
Only gold members can continue reading.
Log In or
Register to continue
Related

Full access? Get Clinical Tree