Chapter 31 Surgical Airway
I Introduction
A General Principles
Emergency surgical airway management comprises four distinct but related techniques that gain access to the infraglottic airway. These are needle cricothyrotomy, percutaneous cricothyrotomy, surgical cricothyrotomy, and surgical tracheostomy. In emergency situations, cricothyrotomy is greatly preferred over tracheostomy because of its relative simplicity, speed, and lower complication rate. The airway is very superficial at the level of the cricothyroid membrane (CTM), separated from the skin only by the subcutaneous fat and anterior cervical fascia. The trachea moves progressively deeper in the neck as it travels caudally, making anterior access more difficult and introducing additional anatomic barriers (e.g., thyroid isthmus.) Needle cricothyrotomy with percutaneous transtracheal ventilation may provide temporary oxygenation in some patients, but the technique does not provide a secure (protected) airway and cannot support ventilation. Needle cricothyrotomy is reviewed elsewhere in this textbook (see Chapter 30). The emphasis in this chapter is on surgical and percutaneous cricothyrotomy; because the former, and in some cases the latter, places a cuffed endotracheal tube (ETT) in the trachea.
Any discussion of surgical airway management techniques must account for three important concepts:
1 Those Responsible for Surgical Airway Management Have Limited or No Experience
Contemporary emergency department studies using RSI demonstrate high success rates (97% to 99%) and an infrequent need for surgical airway rescue (0.5% to 2.0%) even though the unselected nature of the patients and the large percentage with trauma result in a high proportion of DAs compared with those seen in elective surgery.1–5 Despite increasing familiarity with alternative airway rescue devices (e.g., flexible and semirigid fiberoptic bronchoscopy, video laryngoscopy, retroglottic airways, supraglottic airways, retrograde intubation, lighted stylet) that further reduce the need for cricothyrotomy, the surgical airway remains the final pathway on all failed airway algorithms.6 Therein lies the dilemma. As clinicians embrace new technologies and devices that make the need for surgical airway management increasingly rare, acquisition and maintenance of the skills necessary to perform surgical airway management, which in some cases is the only method capable of sustaining a patient’s life, become increasingly elusive.
B Historical Perspective
The surgical airway as a life-saving procedure has been appreciated for thousands of years. The first depictions of surgical tracheostomy were found on Egyptian tablets dating from 3600 BC.7 In the second century AD, Galen suggested tracheostomy, utilizing a vertical incision, as an emergency treatment for airway obstruction.8–10 Vesalius later published the first detailed descriptions of tracheostomy in the 16th century, using a reed to ventilate the lungs. Ironically, his alleged resuscitation of a Spanish nobleman through tracheostomy and ventilation led to condemnation by the Spanish Inquisition and his ultimate death.11 The first record of a successful tracheostomy performed in the United States was in 1852; the patient later died of airway stenosis, a common complication at that time. A paper from 1886 described a mortality rate of 50% for tracheostomy and a high incidence of stenosis, which accounted for many of the deaths.12
Chevalier Jackson published a landmark paper on tracheostomy in 1909, which enumerated principles still relevant today.13 He described a surgical mortality rate of only 3%, which he attributed to several factors: optimal airway control before surgery, use of local anesthesia rather than sedation, use of a well-designed tube, and meticulous surgical and postoperative care. Jackson achieved international recognition; however, so did his condemnation of “high tracheostomy” as the cause of subglottic stenosis. The high tracheostomy he referred to was a cricothyrotomy, which at that time involved division of the cricoid or thyroid cartilage. Modern cricothyrotomy involves incision of the CTM only. In 1921, Jackson published a study of 200 patients referred to him for postcricothyrotomy stenosis. Aside from the obvious referral bias, the indication for a surgical airway at that time was primarily inflammatory lesions of the upper airway, which probably accounted for the high incidence of subglottic stenosis.14
Although in retrospect it was the technique and the underlying condition that were largely responsible for the high rate of stenosis, fear of this complication condemned the technique of cricothyrotomy for over half a century. In the interest of developing a technique that was safer and quicker than Jackson’s open dissection, Toye and Weinstein described the first percutaneous tracheostomy in 1969.15 However, cricothyrotomy was not widely reconsidered as a surgical airway option until 1976, when Brantigan and Grow published the results of cricothyrotomy for long-term airway management in 655 patients.16 In their series, the rate of stenosis was 0.01%, no major complications were described, and the procedure was found to be faster, simpler, and less likely to cause bleeding than tracheostomy. Subsequent studies have supported their conclusion that cricothyrotomy is a safe and effective surgical airway procedure and should be the preferred technique when emergent surgical airway control is needed.7,17,18 Contemporary case series have demonstrated that cricothyrotomy can be performed with a high success rate and a reasonably low complication rate by hospital-based physicians and other clinicians (i.e., nurses, paramedics) providing prehospital care.13,19–25
C Definitions of the Surgical Airway
The terms surgical cricothyrotomy and surgical tracheostomy refer to the use of a scalpel and other surgical instruments to create an opening in the airway.26,27 This technique allows the creation of a definitive, protected airway by the insertion of a cuffed tracheostomy tube with an internal diameter sufficient for ventilation, oxygenation, and suctioning.
The percutaneous dilational technique utilizes a kit or device that is intended to establish a surgical airway without requiring a formal surgical cricothyrotomy (see Chapter 30 for a detailed discussion). Following a small skin incision, the airway is accessed by a small needle through which a flexible guidewire is passed using the Seldinger technique. The airway device is then introduced over a dilator and passed over the guidewire and into the airway in a manner analogous to that of central line placement. An alternative percutaneous technique has been used that relies on placement of an airway device using a direct puncture into the airway; an example is the Nu-Trake Adult Emergency Cricothyroidotomy Device (Smiths Medical, Keene, NH). A large-bore metal needle or a sharp trocar within the catheter is used to puncture the airway directly, without the use of a guidewire. Direct puncture devices are more hazardous and have fallen out of favor because of a higher incidence of complications and a lower success rate compared with other percutaneous techniques.28–32
Transtracheal catheter ventilation, considered the least invasive surgical technique, involves the direct placement of a moderate-bore catheter through the CTM.33 The small caliber of these devices does not allow adequate oxygenation without attachment to a high-pressure oxygen source or jet ventilator, except in small children, and does not support adequate ventilatory gas exchange. A 6-F reinforced fluorinated ethylene propylene, kink-resistant emergency transtracheal airway catheter (Cook Critical Care, Bloomington, IN) has been designed as a kink-resistant catheter for this purpose.
D Role of the Surgical Airway
The relative merit of percutaneous dilatational tracheostomy versus open surgical tracheostomy continues to be a subject of debate. Although formal open tracheostomies are primarily performed by surgeons, the percutaneous dilatational tracheostomy is frequently performed by anesthesiologists and other nonsurgical intensivists, particularly in the intensive care setting. This technique was originally described by Toye and Weinstein in 1969, but it did not gain popularity until the results with a modified device were reported by Ciaglia and colleagues in 1985.12,15 There have been no clinical studies to date demonstrating the superiority of any one approach over another or of any of these devices over formal surgical cricothyrotomy.
II Anatomy
A Bones and Cartilages
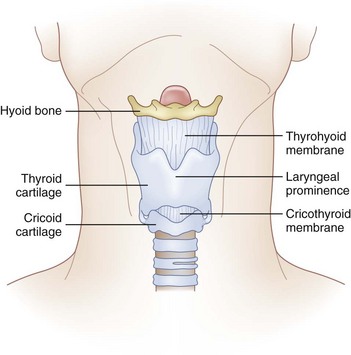
The cricoid cartilage, the only complete cartilaginous ring in the upper airway, defines the inferior aspect of the larynx (Fig. 31-1). It is shaped like a signet ring, with the wider lamina posterior. Superiorly, the lamina has synovial articulations with the arytenoids and thyroid cartilage. Anteriorly, the cricoid ring is attached to the inferior thyroid cartilage by the CTM.
C Vascular Structures
The right and left cricothyroid arteries are branches of the right and left superior thyroid arteries, respectively, and in most patients they cross the superior aspect of the CTM to anastomose in the midline.34 Although they are at risk for injury during a cricothyrotomy, they do not appear to be clinically significant. Bleeding is often self-limited and is easily controlled with gauze packing. There is no venous plexus over the CTM.
E Anatomic Variations
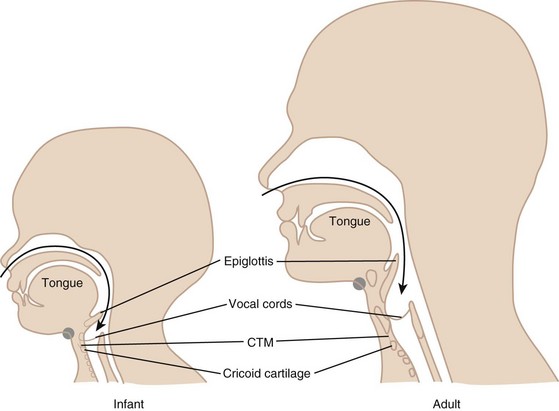
In infants, the hyoid bone and cricoid cartilage are the most prominent structures in the neck. The laryngeal prominence does not develop until adolescence. The larynx also starts higher in the neck of the child; it descends from the level of the second cervical vertebra at birth to the level of the fifth or sixth in the adult.35 The laryngeal prominence is more acute and therefore more prominent in adult males compared with females. This also results in longer vocal cords and accounts for the deeper voices of males.
The CTM varies in size among adults and can be as small as 5 mm in height. This space may narrow further with contraction of the cricothyroid muscle.36 The CTM in the child is disproportionately smaller in area than that in the adult (Fig. 31-2). In an infant, the width of the membrane constitutes only one fourth of the anterior tracheal diameter, as opposed to three fourths in the adult. Because of this smaller area and the difficulty in identifying landmarks in children, emergency surgical cricothyrotomy is difficult and hazardous in small children and is not recommended in those younger than 10 years of age. In this age group, placement of a needle catheter with percutaneous transtracheal ventilation is the preferred method.
III Surgical Cricothyrotomy
A Indications and Contraindictions
The primary indication for an emergent surgical airway (Box 31-1) is the failure of endotracheal intubation or alternative noninvasive airway techniques in a patient who requires immediate airway control. The American Society of Anesthesiologists (ASA) DA algorithm advocates a surgical airway as the final end point for the unsuccessful arm of the emergency pathway.37,38 There are a number of other DA algorithms in the literature, as well as numerous modifications of the ASA guidelines; however, all comprehensive pathways include the surgical airway as the technique of choice when others have failed.38–40 Despite the introduction of numerous alternative rescue devices, the most common error in the management of the DA is persistent attempts at laryngoscopy in a failed airway situation.41–43 This behavior has been associated with increased morbidity and mortality.41 Identification of the CICV scenario should result in immediate consideration of surgical airway access. If alternative methods are tried despite inability to oxygenate and ventilate the patient by bag and mask, precious time may be lost in what are ultimately futile attempts, and by the time cricothyrotomy is undertaken and accomplished, delays in achieving airway control and oxygenation will have led to hypoxic brain injury.
Box 31-1 Indications for Cricothyrotomy
In most circumstances, cricothyrotomy is regarded as an emergency rescue technique when other noninvasive rescue techniques, such as the laryngeal mask airway, have failed, are predicted to fail, or are unavailable.1 There are occasions, however, when a cricothyrotomy is the primary airway of choice. An example is the patient who has such severe facial trauma that nasal or oral approaches to the airway are deemed impossible. There also has been a renewed interest in the role of elective cricothyrotomy in the operative setting. Some cardiothoracic surgeons prefer cricothyrotomy to a tracheostomy in their patients with a median sternotomy, believing that the higher location of the airway wound reduces the potential for contamination of the sternal wound.11 A study described the use of elective cricothyrotomy instead of tracheostomy in the intensive care unit for trauma patients with technically challenging neck anatomy. The procedure was described as simpler with no difference in short- or long-term complications.44
Cricothyrotomy is considered safe in trauma patients with unstable cervical spine injuries provided that cervical spine immobilization is maintained.45,46 Although coagulopathy has been described as a relative contraindication, there are reports of successful cricothyrotomy after systemic fibrinolytic therapy for acute myocardial infarction.47
Contraindications for surgical airway management are few and, with one exception, are relative. That one exception is young age. Children have a small, pliable, mobile larynx and cricoid cartilage, making cricothyrotomy extremely difficult. For children younger than 10 years, unless the larynx and cricoid cartilage are teenage or adult sized, percutaneous transtracheal ventilation should be used as the surgical airway management technique of choice. Two other situations have been proposed as absolute contraindications: tracheal transection and laryngeal fracture.48 In either situation, tracheostomy has been recommended as the preferred method. Although anatomically and philosophically appealing, this assertion is clinically impractical. First, these injuries may not be readily apparent at the bedside. Second, there may be no other means of securing the airway in a dying patient. Third, expert surgical backup may not be readily available, and tracheostomy is a much more complicated procedure than cricothyrotomy. Therefore, these, too, should be considered relative contraindications; cricothyrotomy should be recognized as carrying significant risk in these situations and used when there is thought to be no other method to secure the airway. Relative contraindications also include preexisting laryngeal or tracheal pathology such as tumor, infections, or abscess in the area in which the procedure will be performed; hematoma or other anatomic destruction of the landmarks that would render the procedure difficult or impossible; coagulopathy; and lack of operator expertise.
Related posts:
 Prehospital Airway Management
Prehospital Airway Management
 Medical-Legal Considerations: The ASA Closed Claims Project
Medical-Legal Considerations: The ASA Closed Claims Project
 Performance of Rigid Bronchoscopy
Performance of Rigid Bronchoscopy
 Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)
Intubating Introducers, Stylets, and Lighted Stylets (Lightwands)

Full access? Get Clinical Tree


