and Ángel Zorraquino González2
(1)
Department of Abdominal Wall Surgery, Faculty of Medicine at the University of Valencia, La Fe University Hospital, Valencia, Spain
(2)
Department of General Surgery, Abdominal Wall Surgery Unit, Faculty of Medicine at the Basque Country University, Basurto University Hospital, Bilbao, Basque Country, Spain
Keywords
Abdominal wall reconstructionSeparation of componentsPreoperative progressive pneumoperitoneumBotulinum toxinIntra-abdominal pressureVacuum-assisted therapyBiomaterialBiofilmIntroduction
At the end of the 1980s, the situation of abdominal wall surgery was paradoxical. While the techniques of autoplasty represented a great technological development (Albanese, Lázaro da Silva), and prosthetic materials were used to reinforce plasties, mainly polypropylene meshes in retro muscle options (Rives) or onlay (Chevrel), it was significant that at the time little attention was given to this type of surgery by the surgeons themselves, who delegated this procedure to surgeons-in-training: the opening and closing of the abdominal wall was looked upon as merely a step prior to what was then considered the main surgery on the abdominal viscera.
In the late 1990s and mainly in the last decade, we have witnessed a drastic change in this sense, due to two facts that occurred simultaneously. On the one hand, the publication of the Component Separation Technique by Oscar Ramirez in 1990 acted as a catalyst for the abdominal wall restorative surgery described by Albanese in 1951; and on the other hand, the development of laparoscopic surgery and the emergence of minimally invasive surgery in gastrointestinal pathology affected access to the peritoneal cavity and treatment of the abdominal wall. Both coincide in timing to polarize the attention of general surgeons regarding a surgery that was left behind, considered a complication of digestive system surgery more than a pathology by itself: the abdominal wall hernia surgery.
With the use of the laparoscopic approach, attention is on the development of prostheses that can be placed on the parietal peritoneum covering the defect without the risk of a visceral injury, and on devices to hold the prosthesis, such as helical staples, applied via trocars.
With the Component Separation Technique, the interest in abdominal wall anatomy and physiology has risen again, bringing back old techniques of autoplasty and procedures to reverse the content of large hernia sacs to a reduced abdominal cavity, adapting it to a smaller volume, such as in the case of the preoperative progressive pneumoperitoneum.
The creation of a whole arsenal of surgical techniques and prosthetic materials has led to the emergence of specific departments or sections devoted to Abdominal Wall Surgery that can be seen as a subspecialty of General Surgery in large hospitals, and to the creation of scientific societies for the study and dissemination of the knowledge that is emerging in this surgical field still experiencing advances today.
The Preoperative Period
When we consider the surgical treatment of eventration, we must have a protocol established for the global study of the patient, for the request of preoperative tests, and for the preparation of the patient for surgery. Its implementation will allow for the best chances for a successful intervention, both in terms of a definite cure of the hernia and in terms of the reduction of complications that may arise in the postoperative period. The protocol includes:
1.
Performing a Valsalva CT
2.
Performing Preoperative Progressive Pneumoperitoneum
3.
Use of Botulinum Toxin
4.
Use of Muscle Expanders
Imaging Tests
The diagnosis of eventration and abdominal wall hernias is usually clinical, and a physical examination is sufficient in most cases. However, in cases of complicated hernias or atypical locations and in obese patients or in those with a history of previous abdominal surgery, the clinical diagnosis may be difficult.
Imaging techniques effectively establish the diagnosis in these uncertain cases, differentiating other situations that may look like hernias or eventrations, such as asymmetries, muscle atrophy and paralysis, bruising, or tumors of abdominal wall. Also, imaging allows for evaluation of related complications, abdominal volume, and hernia sac volume; helps in terms of assessing the availability of the aponeurotic muscle plane; and assists with choosing the best therapeutic options.
The development of imaging techniques in recent years has allowed us to obtain very precise and quantifiable information regarding hernia orifices, location, content, and muscle condition.
Ultrasound is a technique that has a variable sensitivity and specificity as demonstrated in published series, since it depends upon the skill and experience of the operator and also depends on the physical characteristics of the patient. It is an imaging technique that, due to its noninvasive features, is considered a technique of choice for pediatric patients.
Computerized Tomography (CT) is currently the most widely used technique in the overall assessment of the condition of the abdominal wall. It is an effective technique in the detection of hernias and allows classification with low operator variability. Also, with the current multi-detector equipment, it is an extraordinarily rapid test that can be performed in just a few seconds. Although there are different imaging protocols, it is normally recommended to obtain reconstructed images with a thickness less than 3 mm, which would allow for obtaining high-quality multiplane images (sagittal, coronal, oblique) later.
In studies of abdominal wall with CT, it is not required to systematically use intravenous contrast media, although its use is indispensable for performing the test to evaluate possible complications and to study the vascularization of the abdominal wall. The positive oral contrast (iodinated or barium) can help with the identification of small bowel herniated loops and differentiate hernias from seromas or other liquid content collection.
Magnetic Resonance Imaging (MRI) is a safe imaging technique that uses magnetic properties of protons to produce high contrast resolution images. Compared to CT, MRI is less available, has lower spatial resolution, has more sensitivity to motion artifacts, and takes longer to perform; therefore, most centers use it less than CT to evaluate the abdominal wall.
It is recommended that CTs and MRIs be carried out with the Valsalva 1 maneuver, since the supine position reduces intra-abdominal pressure, therefore reducing the herniated content and even decreasing the orifice diameters (see Fig. 47.1a, b).
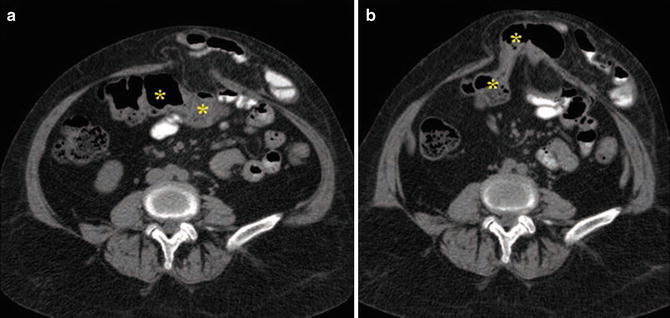
Fig. 47.1
Midline eventration with herniation of jejunal loops. Transverse CT images in apnea (a) and with Valsalva maneuver (b) where the hernia contents increased after the maneuver, including also the transverse colon (a, b: Used with permission from Carbonell-Tatay F, Moreno-Egea A (eds). Eventraciones. Otras hernias de pared y cavidad abdominal. Valencia (Spain): Spanish Association of Surgeons (AEC); 2012)
The Valsalva maneuver (such as coughing and defecation) simulates abdominal pressure originating from daily life activity. When performing it during the study, it not only allows for a better evaluation of the herniated content but also minimizes false negatives. It is important to highlight that up to a 10 % of hernias are not detected in the studies performed without the Valsalva maneuver.
Preoperative Progressive Pneumoperitoneum (PPP)
Surgical repair of large hernias requires the preparation of the patient to receive the visceral content from the hernia sac into an abdominal cavity reduced by the retraction of anterolateral abdominal muscles and the secondary loss of the diaphragm muscle’s function that cannot find support to recover its concavity after contracting due to the loss of the abdominal wall’s tone.
To make the reduction of hernia content possible without the negative consequences of the increased intra-abdominal pressure and the respiratory restriction that would cause its immediate reduction, the PPP is used.
The Argentine surgeon Iván Goñi Moreno (1905–1976) (Fig. 47.2) noticed the abdominal distension that occurred in some patients after accidental air leakage into the peritoneal cavity during the diagnostic retro-pneumoperitoneum that was performed at the time as double contrast technique to study kidneys and adrenal glands, reporting its usefulness to repair large eventrations in the XII Argentine Congress in October 1940 and publishing his experiences years later (1946). Since then, the preoperative progressive pneumoperitoneum has been used to increase the size of the abdominal cavity in the repair of large eventrations, facilitating the reduction of the hernia sac content and the closure of the abdominal wall without tension. It has avoided space conflicts, high intra-abdominal pressure, and its most severe consequence, the Abdominal Compartment Syndrome (ACS).

Fig. 47.2
Iván Goñi Moreno, M.D., (1905–1976) (Used with permission from Carbonell-Tatay F, Moreno-Egea A (eds). Eventraciones. Otras hernias de pared y cavidad abdominal. Valencia (Spain): Spanish Association of Surgeons (AEC); 2012)
The way to conduct the pneumoperitoneum may vary, but it basically consists of the introduction of environment air through a catheter that is placed in the peritoneal cavity through the abdominal wall. At our hospital, an eight French catheter is introduced, with the guidance of ultrasound, into the peritoneal cavity at one of the sides of the abdomen, based on the characteristics and location of the eventration. Usually patients are admitted 7–10 days before surgical intervention in order to conduct progressive pneumoperitoneum. The preoperative progressive pneumoperitoneum is intended to stabilize the diaphragm muscle, stimulating its function, and to dissect lax adherences inside the hernia sac by the action of introduced air. To prevent the air from distending only the hernia sac, where it will usually settle itself because of its lower pressure, an abdominal binder will be placed on the patient, allowing air distribution in the abdominal cavity and increasing the efficacy of the procedure as the total volume of air required is reduced, shortening the duration of the procedure.
The increase in the abdominal cavity affecting anterolateral muscles of the abdominal wall requires the procedure to be longer, in the experience of Dr. León Herszage (Fig. 47.3), no less than 30 days.

Fig. 47.3
León Herszage, M.D.
In our experience, admitting the patient 7–10 days before the surgical intervention is sufficient to achieve the first two objectives of developing the pneumoperitoneum: give functional support to the diaphragm muscle and promote a pneumatic dissection of the hernia content, achieving its partial or complete reduction to the abdominal cavity. To increase the capacity of this cavity, we have always been confident in the use of autoplastic techniques, with good results. During the preoperative period, a functional respiratory study and chest physiotherapy should be conducted.
The Botulinum Toxin
Some medical schools, such as those in Mexico, combine performing the PPP with the use of Botulinum Toxin on the muscles of the abdominal wall, so that the pneumoperitoneum results are more effective due to muscle paralysis.
This is a technique described by Dr. Tomás Ibarra (Fig. 47.4) in 2007 and published in 2009. The botulinum toxin type A is used by infiltrating it in the side muscles of the abdomen (transverse and oblique of both sides) in order to cause a temporary paralysis, reducing therefore the pressures that tend to separate the rectus muscles and enlarge the hernia defects, allowing also an increase of the abdominal cavity volume up to a maximum of 20 % of its initial capacity in a period of 30 days [1].

Fig. 47.4
Tomás R. Ibarra-Hurtado, M.D.
The effect of the toxin is to block the release of acetylcholine at the motor plate of the nerve ending. This effect is complete and fully reversible in a period of 5–8 months. Subsequently, the release of acetylcholine will return to its previous values with no adverse effect on muscle contractility.
The right place for the infiltration of the toxin is determined by electromyography, locating the sites with more electrical activity. There are 5 points in which, constantly and in most patients, a total paralysis of the 3 muscles can be induced with post-infiltration electromyography control. The points are located as follows: two at the midaxillary line, equidistant between the lower costal edge and the iliac crest, and another three points at the level of anterior axillary line. Nowadays Dr. Ibarra and cols. They determine these five points using anatomical references with the help of transverse CT images to measure the distance from the skin to the muscle planes in both abdominal sides (see Fig. 47.5).
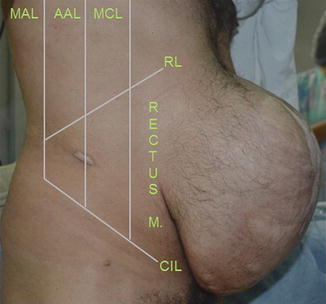
Fig. 47.5
References to locate the infiltration points of the Botulinum toxin. MAL medium axillary line, AAL anterior axillary line, MCL Medium clavicular line, RL Ribs line, ICL Iliac crest line, Rectus M Abdominal rectus muscle. Two punctures between MAL and AAL, and three between AAL and MCL; the same punctures on the left side (Used with permission of Dr. Tomás Ibarra-Hurtado)
For this technique, 50 U of the toxin is infiltrated in each of the five specific points of the right side and five of the left side, for a total of 500 U. The toxin is prepared by diluting the lyophilized powder in 10 ml of saline solution (1 ml = 50 U) or, if preferred, in 20 ml (2 ml = 50 U).
Total paralysis of the muscles is achieved during the first 10 days, and dilatation of the abdominal wall and the reduction of the hernia defect horizontally, without compromising the trunk movements or respiratory function, will commence. Usually, patients have no discomfort, and only some of them referred to feeling a slight flaccidness at the sides of abdomen. The maximum muscle relaxation is reached within 30 days, with an average of 20 % of volume gain, and, according to the authors’ experience, there are no more volume increases afterwards (see Fig. 47.6).
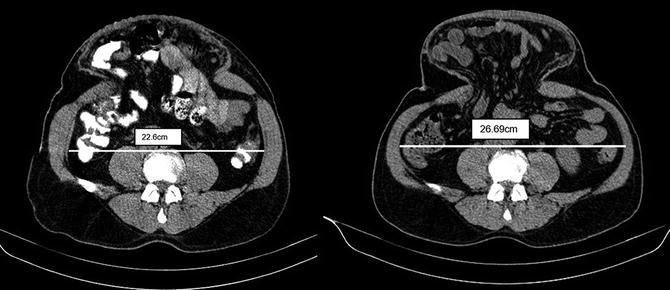
Fig. 47.6
CT images: Increased volume and abdominal muscle relaxation after injection of botulinum toxin (Used with permission of Dr. Tomás Ibarra-Hurtado)
It is therefore suggested that the wall repair procedure be performed after 30 days, with the advantage of still having 5–6 months of toxin effect so as to protect the suture line of the repair, which should always be reinforced with a mesh.
Muscle Expanders
Another option to achieve progressive distension of lateral muscles prior to surgical repair is placing silicone expanders between the bellies of the oblique muscles. The tissue expansion obtained provides autologous tissue, as well as vascularized, with contractile capacity for the repair of defect in the abdominal wall. This procedure can be combined with the use of Botulinum Toxin.
In 1989, Henry Stephenson Byrd, a surgeon from Texas, published on the use of expanders in children with congenital abdominal abnormalities (bladder exstrophy and absence of lower half of the abdominal wall) [2]. Paul Creighton Hobar in 1994 published on the first case of abdominal wall reconstruction of an acquired defect.
The skin incision should be performed to ensure that there are no injuries in the neurovascular bundles that supply the abdominal wall, strictly respecting the anatomical planes. Normally, expanders are placed between the external oblique and the internal oblique deep complex and the fascia transversalis, this being one of the safest areas to place the expander, without interrupting blood supply or innervations of abdominal wall muscles.
A transversal incision has to be made, not a vertical one, in the costal margin, through the fascia of external oblique, so that no nerves or vessels are affected; at this plane level, between the fascia of the external oblique and the internal oblique, the pocket where the expander is placed is formed, limiting its lower edge with the inguinal ligament, medially with the lateral margin of the rectus, laterally with the midaxillary level, where the neurovascular perforating vessels of the external oblique can be found, and at superior level, with the costal margin (see Fig. 47.7).
Fig. 47.7
Scheme showing the muscle expander in site (Used with permission of illustrator, Pedro Sánchez Abril. Previously published in Carbonell-Tatay F, Moreno-Egea A (eds). Eventraciones. Otras hernias de pared y cavidad abdominal. Valencia (Spain): Spanish Association of Surgeons (AEC); 2012)
The first expansion is started within 3 weeks, and the total process lasts approximately between 6 and 12 weeks until there is enough tissue; at that moment, the expander is removed and we proceed with the advance of the flap. Later, a layered closure without tension of the obtained tissue will be performed. The frequency and volume of the expansion will depend on the tolerance level of the patient, and it is normally performed every 2 weeks. The expansion at both sides of the abdominal wall defect will speed up the resolution time.
However, it is obvious that this procedure should be done in selected patients with good skin coverage.
Repair of the Abdominal Wall
The objectives of an ideal reconstruction of the abdominal wall should include prevention of acute eventration, the establishment of an adequate coverage of the abdominal content, closure without excessive tension, and adequate functional muscle support. Sometimes we must also add a fifth objective: achieving an adequate aesthetic result. Although is not always possible to achieve all these objectives, it is wise to remember them before facing a new case of eventration, as it will help with the planning of the parietal reconstruction.
Although the extremes of the defect may be brought closer with a primary closure, this usually creates quite a lot of tension at the closure line, which normally leads to poor results with a high recurrence rate.
Meshes prevent the tension, but do not achieve an adequate muscular dynamic and can present a great variety of additional complications (infection, sepsis, material extrusion, sinus formation, and fistulas).
Tissue expansion techniques and autoplasties are efficient methods of repair that, well indicated and in selected patients, could be the solution of choice, as we use the abdominal wall tissue itself, well innervated and functional, to complete the repair and restore biomechanics of the abdominal wall.
In the past decade, the dissemination of prostheses has quickly changed the way many surgeons operate, but the knowledge of these anatomical techniques below remains basic and crucial in order to be able to solve many situations successfully and combine various procedures (autoplasty plus aloplasty) into a surgery with more guarantees for the patient:
1.
Autoplasty Technique described by Albanese in 1951
2.
Component Separation Technique popularized by Oscar Ramírez
3.
Anatomical Component Separation Technique described by Fernando Carbonell and Santiago Bonafé
4.
Posterior Component Separation Technique
5.
Laparoscopic Approach applied to the treatment of eventration
6.
Prostheses
Autoplasties
In May 1946, Dr. Alfonso R. Albanese (1906–2008) (Fig. 47.8) operated on a 4-year-old patient who had a large midline hernia with an 8–10 cm diameter hernial ring due to a surgery done 8 months before in order to repair the obstructive symptoms that caused the peritoneal bands on the duodenum after an intestinal malrotation (Ladd’s bands).

Fig. 47.8
Dr. Alfonso R. Albanese (1906–2008) (Used with permission from Carbonell-Tatay F, Moreno-Egea A (eds). Eventraciones. Otras hernias de pared y cavidad abdominal. Valencia (Spain): Spanish Association of Surgeons (AEC); 2012)
Dr. Albanese worked in the Surgery Department of the Hospital Rawson (Buenos Aires), and the chief was Dr. Ricardo Finochietto. There they usually applied the Quénu-Noble technique to repair incisional hernias. Albanese also was an assistant in the Department of Topographical Anatomy of the University of Buenos Aires where he prepared anatomical materials for the classes of Professor Eugenio A. Galli. Albanese had passion for anatomy, a dedication that made him the creator of various surgical procedures, pioneering surgical repair of cardiac malformations in addition to the surgical technique for repairing large abdominal hernias.
His technique is designed to free the rectus muscle from the lateral traction of the oblique muscles as a result of the loss of continuity of the oblique muscles on each other.
With the completion of three longitudinal incisions in every hemiabdomen—one over the aponeurosis of the external oblique muscle (Fig. 47.9a), the second one in the anterior lamina of the internal oblique muscle just on the outer edge of the rectus muscle (Fig. 47.9b), and the third one on the inner third of the anterior sheath of rectus muscle (Fig. 47.9c)—this technique:
Fig. 47.9
 End Points of Resuscitation
End Points of Resuscitation
 Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
 The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
 New Minimally Invasive Treatments for Acid Reflux
New Minimally Invasive Treatments for Acid Reflux
 Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
 Laparoscopic Approaches in General Surgery: Is There Anything New?
Laparoscopic Approaches in General Surgery: Is There Anything New?



The technique developed by Dr. Albanese and reported in 1951, designed to free the rectus muscle from the lateral traction of the oblique muscles as a result of the loss of continuity of the oblique muscles (a–c: Used with permission of illustrator, Pedro Sánchez Abril. Previously published in Carbonell-Tatay F, Moreno-Egea A (eds). Eventraciones. Otras hernias de pared y cavidad abdominal. Valencia (Spain): Spanish Association of Surgeons (AEC); 2012)
Related posts:
End Points of Resuscitation
Cardiac Surgery Advances: Do We Still Remember How to Do the Open Bypass?
The Role of Robotics in Selective Thoracic Surgical Problems: Technical Considerations
New Minimally Invasive Treatments for Acid Reflux
Minimally Invasive Hepato-Pancreato-Biliary Surgery and Associated GI Interventions
Laparoscopic Approaches in General Surgery: Is There Anything New?
Full access? Get Clinical Tree
