Key Clinical Questions
What electrocardiographic findings help differentiate between the common supraventricular tachyarrhythmias (SVTs)?
What acute and chronic management strategies are indicated for various SVTs?
What comorbid conditions increase the risk of thromboembolic complications in patients with atrial fibrillation?
Which patients with atrial fibrillation deserve anticoagulation, and which of these patients need bridging anticoagulation until oral warfarin attains therapeutic international normalized ratio (INR)?
Which SVTs deserve electrophysiologic intervention over medical management?
Introduction
Supraventricular tachyarrhythmias (SVTs) comprise an array of narrow-complex arrhythmias that originate above the ventricles and include both the most commonly encountered arrhythmia, atrial fibrillation (AF), and the uncommon ones, such as Wolfe-Parkinson-White (WPW) syndrome. This chapter describes in detail the common atrial arrhythmias encountered by hospitalists, and explains the uncommon arrhythmias that hospitalists should recognize and manage with cardiologist or electrophysiologist consultation or referral. The chapter will briefly describe arrhythmia mechanisms while focusing on arrhythmia diagnosis, management options in the acute setting, and long-term management strategies—all essential for a seamless transition beyond the inpatient setting.
Presentation
Common presenting symptoms of SVTs include rapid palpitations, chest discomfort, dyspnea, presyncope, and syncope. Additionally, atrial fibrillation and atrial flutter may present with new stroke symptoms. Particularly in the elderly with atrial fibrillation, palpitations and chest discomfort are often absent and excessive fatigue is the predominant symptom.
Rhythm Identification
When evaluating patients with a narrow-complex arrhythmia, the QRS complex is by definition less than 120 ms. The regularity of the RR intervals then helps reduce the numerous possibilities, as indicated in the SVT recognition algorithm (Figure 126-1). Only four possibilities exist if the RR intervals are irregular: (1) atrial fibrillation, (2) atrial flutter with variable atrioventricular (AV) node blockade, (3) atrial tachycardia with variable AV node blockade, and (4) multifocal atrial tachycardia (MAT).
Figure 126-1
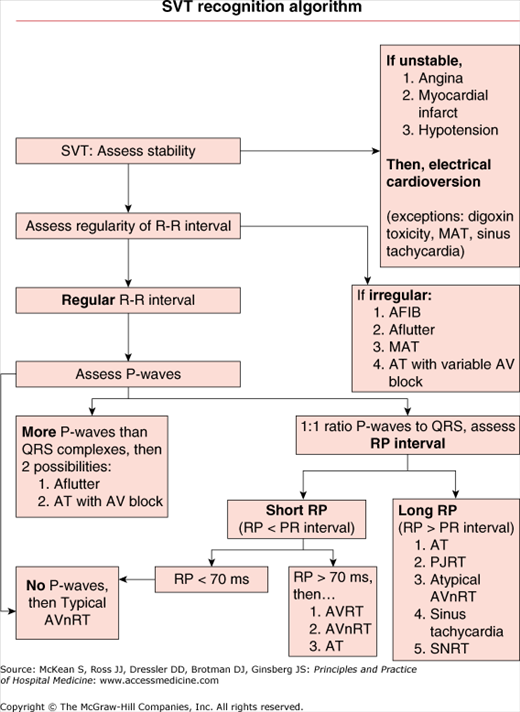
Supraventricular tachyarrhythmia recognition algorithm. AF, atrial fibrillation; Aflutter, atrial flutter; AT, atrial tachycardia; AV block, atrioventricular block; AVnRT, atrioventricular nodal reentrant tachycardia; AVRT, atrioventricular reentry tachycardia; MAT, multifocal atrial tachycardia; PJRT, paroxysmal junctional reentrant tachycardia; SNRT, sinus node reentry tachycardia.
More challenging to diagnose is the SVT with a regular RR interval. If, however, no P wave can be identified, this indicates the most common form of paroxysmal SVT: atrioventricular nodal reentrant tachycardia (AVnRT). The P wave in typical AVnRT is buried within the QRS complex. If the P wave is identified, then determine if there is more than one P wave for each conducted QRS. If so, then only atrial flutter or atrial tachycardia remain as possible diagnoses.
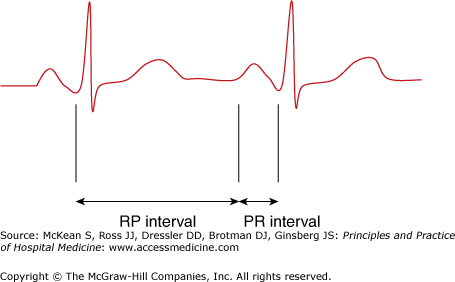
Finally, if only a 1-to-1 relationship between the P waves and QRS complexes exists, measuring the RP interval will further narrow the likely rhythms (Figure 126-2). The response of the rhythm to bedside vagal maneuvers or intravenous adenosine can be used to better differentiate the regular narrow-complex arrhythmias by transiently slowing the AV conduction and revealing the P waves, converting the rhythm to sinus, or gradually slowing and reaccelerating the tachycardia (Table 126-1).
| Rhythm | Response to Transient AV Node Blockade (vagal maneuvers or IV adenosine) |
|---|---|
| AVnRT | Sudden termination |
| AVRT | Sudden termination |
| Sinus reentry tachycardia | Sudden termination |
| Focal atrial tachycardia | Sudden termination, or gradual slowing and reacceleration |
| Ventricular tachycardia (high septal or fascicular origin) | No response |
| Sinus tachycardia | Gradual slowing, then reacceleration |
| Nonparoxysmal junctional tachycardia | Gradual slowing, then reacceleration |
| Atrial flutter | Persistent atrial tachycardia and transient high-grade AV blockade |
| Macroreentrant atrial tachycardia | Persistent atrial tachycardia and transient high-grade AV blockade |
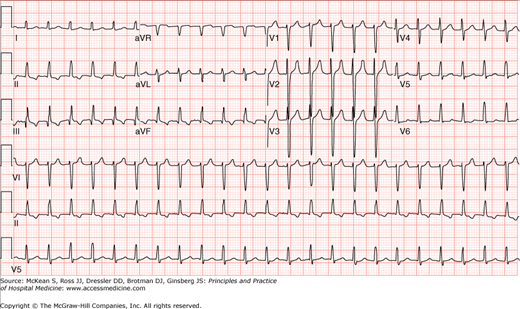
Proceeding through the SVT recognition algorithm (see Figure 126-1) using a sample ECG (Figure 126-3) the clinician first recognizes that the rate is greater than 100 beats per minute (bpm). The QRS complexes are narrow, thus leading to a generic diagnosis of SVT. Following the SVT recognition algorithm, the regularity of the RR intervals is assessed, and the absence of P waves leads to the conclusion that the SVT is attributable to typical AVnRT (see Figure 126-3).
Atrial Fibrillation
Before the age of 60, the prevalence of atrial fibrillation (AF) occurs uncommonly, in stark contrast to the prevalence estimate of 8% among those older than 80 years. As AF is the most common arrhythmia encountered by the inpatient clinician, this section will address the questions pertaining to the valvular and nonvalvular etiology of this arrhythmia, judicious utilization of cardioversion, thromboembolic and other complications, methods for estimating risk of stroke, and management strategies in the acute and chronic settings.
Patients with atrial fibrillation are classified in one of three categories: (1) paroxysmal AF, (2) persistent AF, or (3) permanent AF (Table 126-2).
| Paroxysmal AF | Episodes lasting < 7 days and spontaneously converting to sinus rhythm |
| Persistent AF | Episodes lasting > 7 days unless chemical or electrically cardioverted to sinus rhythm |
| Permanent AF | AF resistant to multiple attempts at cardioversion |
| Lone AF | AF in patients younger than 60 years old in the absence of any predisposing factor |
The atrium in patients with AF shows evidence of fibrosis and increased extracellular mass changes that are seen both in the myocardium of the elderly and in ischemia-induced hibernating myocardium. Within this scarred milieu, a focal-enhanced automaticity and variance in atrial tissue refractory and conduction times (known collectively as the multiple wavelet hypothesis) leads to this common arrhythmia. The enhanced automaticity often can be isolated to atrial tissue near the pulmonary veins. In addition to the aging process, any medical condition that leads to elevated left atrial pressure and dilated atrium—hypertension, mitral stenosis or regurgitation, and any cardiomyopathy—will predispose the patient to atrial fibrillation. Hyperadrenergic states—sepsis, alcohol ingestion or withdrawal, postoperative state, and thyrotoxicosis—also predispose to AF. Lone atrial fibrillation describes AF in patients younger than 60 years old in the absence of any predisposing factor.
Common clinical scenarios for hospitalized patients with AF include those with stable tachycardia and those with hemodynamic compromise. For those with hypotension, a trial of short-acting rate-controlling agents (eg, esmolol) could be attempted to determine if slowing the tachycardia may improve the hemodynamics, keeping in mind that these very agents may exacerbate hypotension. Intravenous digoxin and amiodarone are options if hypotension prevents the use of beta-blockers and calcium channel blockers. Synchronized direct cardioversion should be performed if the hypotension does not resolve (see Chapter 125). Currently there are two types of defibrillators: monophasic and biphasic. Biphasic defibrilators are now more common and require less energy and reduced number of shocks delivered to achieve successful cardioversion. Biphasic defibrillators also have reduced skin injury. The monophasic device should be set at a minimum of 200 joules and a maximum of 400 joules. The biphasic device demonstrates effective cardioversion at 200 joules and often times at just 100 joules for AF.
One or multiple rate-controlling agents may be needed to provide adequate control of the ventricular response (Table 126-3). After 24 hours on the intravenous infusion, switching to an oral regimen can be initiated. Beta-blockers and nondihydropyridine calcium channel blockers are considered first-line agents. Intravenous digoxin and amiodarone are reasonable options, particularly in the setting of congestive heart failure. An important limitation of digoxin is that its vagally induced AV node blockade can be easily overcome in nonsedentary patients. Although very effective in rate control and even rhythm conversion, amiodarone has a long-term side-effect profile which relegates its use as a distant second option. Clinicians should target a heart rate under 110 bpm at rest but consider patient symptoms in modification of rate control.
| Medication | Loading Dose | Maintainence Dose | Side Effects |
|---|---|---|---|
| Esmolol | 500 mcg/kg over 1 minute | 60–200 mcg/kg/minute IV | Hypotension |
| Metoprolol | 2.5–5 mg IV over 2 minutes Up to 3 doses | NA | Hypotension |
| Diltiazem | 0.25 mg/kg IV over 2 minutes | 5–15 mg/hour | Hypotension |
| Verapamil | 0.075–0.15 mg/kg IV over 2 minutes | NA | Hypotension |
| Digoxin | 0.25 mg IV every 2 hours up to total dose 1.5 mg | 0.125–0.375 mg/day IV or orally | Digoxin toxicity, heart block |
| Amiodarone | 150 mg IV over 10 minutes | 0.5–1 mg/minute IV | Pulmonary toxcity, hepatitis, skin discoloration, thyroid dysfunction, corneal deposits, optic neuropathy |
The presence of an accessory pathway would be an absolute contraindication in the use of AV node–blocking agents. As electrical impulses are conducted nondecrementally via the accessory pathway, the ventricular response in AF will actually increase and may degenerate into ventricular fibrillation (VFIB).
After assessing clinical stability and adequately controlling the rapid ventricular response, the clinician should determine if the rhythm event is new, recurrent, or an exacerbation of a permanent form of the arrhythmia. If the condition is a new event or a paroxysmal one with infrequent yet very symptomatic recurrences and has been present for less than 48 hours, cardioversion—chemical or electrical—followed by an attempt to maintain a sinus rhythm may offer symptom benefit and is recommended by the ACC-AHA AF guidelines from 2006 (Table 126-4). If the AF duration is longer than 48 hours, cardioversion remains an option after trans-esophageal echo (TEE) is negative for left atrial thrombus. Cardioverting those with new-onset AF provides the theoretical benefit of curtailing the risk of developing permanent AF.
|
Cardioversion can be achieved not only with electrical means, but also chemical means (Table 126-5). The antiarrhythmics used for cardioversion should be considered after consultation with cardiology service. A class III agent, ibutilide, can be used in select patients that have no evidence of systolic dysfunction, normal magnesium and potassium levels, and a normal corrected QT interval (QTc). Due to the risk of torsades de pointes, this should be performed in a setting equipped to handle this potential complication. Ibutilide has the advantage of increasing the efficacy of electrical cardioversion that would follow a failed chemical cardioversion. An oral class III agent, tikosyn, can be used to both convert to a sinus rhythm and also maintain a sinus rhythm. This medication should be reserved for cardiology consultants due to the need for close monitoring of the QT interval, renal dose adjustments, and limitations of use in patients with liver dysfunction. If the QT interval is greater than 500 ms, this medication should not be initiated or should be discontinued. The use of medications to maintain a sinus rhythm should remain under the care of a cardiologist due to the frequency of treatment failure and significant risk of malignant ventricular arrhythmias.
| Medication | Antiarrhythmic Class | Dosing | Route | Comments |
|---|---|---|---|---|
| Amiodarone (codarone, pacerone) | III |
| Oral |
|
| Ibutilide (corvert) | III |
| IV |
|
| Dofetilide (tikosyn) | III | 500 mcg orally twice a day (restricted distribution is the U.S. to trained prescribers and facilities) | Orally |
|
| Flecainide | Ic | Start 50 mg orally twice a day, may increase 100 mg/day every 4 days; max dose 300 mg every day | Orally or IV |
|
| Propafenone | Ia | Start 150 mg orally three times a day, then may increase to 225 mg orally three times a day after 4 days, then, up to 300 mg orally three times a day | Orally or IV | Contraindicated in structural heart disease including significant LVH, CHF, severe obstructive lung disease |
The unorganized atrial contractions during AF will lead to the formation of thrombus or spontaneous echo contrast (SEC) within the left atrium or the left atrial appendage posing a substantial risk of thromboembolic phenomena to the arterial circulation, which usually manifests as stroke and, less commonly, mesenteric ischemia or an acutely ischemic limb. Although the transthoracic echocardiogram is considered the diagnostic test of choice for initial evaluation, the transesophageal echocardiogram (TEE) provides a much better resolution of the left atrium and left atrial appendage and is useful for an early cardioversion strategy. Thrombus or dense SEC would preclude the option for early cardioversion and necessitate the need for full anticoagulation with a vitamin K antagonist for four weeks prior to cardioversion. In the absence of thrombus or SEC on TEE, the patient may receive early cardioversion in the setting of anticoagulation. For AF recognized greater than 48 hours after onset in patients who do not undergo TEE, full anticoagulation for four weeks is recommended followed by cardioversion, if indicated.
In either strategy, anticoagulation for a minimum of four weeks postcardioversion is necessary to reduce the risk of thromboembolic complications. The risk of embolic stroke is approximately 1% with either approach. Stroke risk postcardioversion is due to a “stunning” effect on the left atrium after any form of cardioversion (electrical, chemical, or even spontaneous). This stunning refers to a delay in the actual mechanical contraction of the left atrium, providing an environment ripe for stasis and thus thrombus formation. Benefits from an early cardioversion approach would be quicker conversion to a sinus rhythm, accelerated care for the patient, and potentially less bleeding complications associated without the preceding four weeks of anticoagulation.
|
Invasive management options for atrial fibrillation should be considered secondary options following failure of medical therapies and recurrent admissions due to symptomatic palpitations or heart failure exacerbations. The palpitations associated with atrial fibrillation can be distressing to some individuals, particularly younger patients, and have significant negative impacts on quality of life. If the use of antiarrhythmic regimens has failed, options for catheter-based interventions or even intraoperative left atrial ablation, also known as the Maze procedure can be offered. One catheter-based approach called ablate-and-pace, entails ablating the AV node and then pacing the ventricle. Another catheter-based approach involves isolating the focus of automaticity, usually near the pulmonary veins of the cavoatrial isthmus, ablating the foci, and initiating anticoagulation therapy thereafter. The latter approach is relatively new and long-term outcome research is still pending. The short-term safety of the procedure in centers with established experience has been proven with death rates or stroke rates under 1% and overall major complications about 6% based on international survey data. However, the mean age of the patients enrolled in these trials was 55 years old with intact systolic function and relatively nondilated atrial diameters. More long-term outcome data will be needed before catheter-based interventions can be considered a parallel option to medical treatment. A final option usually reserved for those who are undergoing open heart bypass or valve replacement is the Maze procedure, and even left atrial appendage resection, both of which may prevent the occurrence of postoperative atrial fibrillation.
Complications and Prognosis
Death or significant neurologic deficits occur in 71% of patients with their first episode of embolic complications associated with AF. Reducing this risk is a crucial component in the management of AF. The annual risk of strokes for AF is approximately 4.5% per year, which is reduced by two-thirds (to 1.5% per year) if patients are fully anticoagulated. However, not all patients with this condition carry the same risk of embolic events and, therefore, should be managed based on risk. Clinicians must diagnose the etiology of AF, as that will help determine risk and direct management. The vast majority of AF is nonvalvular, but valvular etiologies such as significant mitral stenosis must be considered. A severalfold increase in thromboembolic risk occurs with mitral valve stenosis–associated atrial fibrillation, and mandates full anticoagulation regardless of other stroke risk factors present. Patients with other risk factors leading to atrial fibrillation have variable levels of evidence supporting full anticoagulation, and some patients with few stroke or embolism risk factors may not attain benefit from anticoagulation that outweighs its risks (Table 126-6).
| AF Risk Factor | Therapy Recommendation | Level of Evidence |
|---|---|---|
| Thyrotoxicosis | Full anticoagulation (eg, warfarin) | Level C: Expert opinion (ACC/AHA guidelines) |
| Mitral stenosis | Full anticoagulation (eg, warfarin) | Level C: Expert opinion (ACC/AHA guidelines) |
| Mechanical valve | Full anticoagulation (eg, warfarin) | Level 1A (ACCP guidelines 2008) |
| CHADS2 score ≥ 2 | Full anticoagulation (eg, warfarin) | Level 1A (ACCP guidelines 2008) |
| CHADS2 score = 1 | Full anticoagulation (eg, warfarin) or aspirin (75–325 mg daily) |
|
| CHADS2 score = 0 | Aspirin therapy (75–325 mg daily) | Level 1B (ACCP guidelines 2008) |
When considering the more common scenario of nonvalvular atrial fibrillation, multiple risk stratification strategies have been published over the decades to estimate the risk of thromboembolic complications, and to date the one most widely used and derived from large cohort data is known as the CHADS2 score. Congestive heart failure, H
Related posts:
 Strategies for Cost-Effective Care
Strategies for Cost-Effective Care
 Building, Growing, and Managing a Hospitalist Practice
Building, Growing, and Managing a Hospitalist Practice
 Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
Designing a Hospitalist Compensation and Bonus Plan
The Face of Health Care Emerging Issues for Hospitalists
 Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist
Medical Malpractice
Preventing and Managing Adverse Patient Events: Patient Safety and the Hospitalist

Full access? Get Clinical Tree


