Fig. 57.1
Anatomy. (1) Celiac plexus, (2) superior hypogastric plexus, (3) inferior hypogastric plexus (With permission from Danilo Jankovic)
Axonal fibers exit these regions as a white rami communicantes to synapse in the paravertebral lumbar sympathetic chain and preaortic ganglia and plexuses. Postganglionic fibers emerge from these regions and, together with contributions from the parasympathetic sacral ganglia, form the superior hypogastric plexus.
The superior hypogastric plexus is a bilateral retroperitoneal structure situated at the level of the lower third of the L5 vertebral body and the upper third of the S1 vertebral body, at the sacral promontory and close to the bifurcation of the common iliac vessels (Fig. 57.2a, b). The superior hypogastric plexus divides into the right and left hypogastric nerves, which descend lateral to the sigmoid colon and rectosigmoid junction to reach the two inferior hypogastric plexuses. The inferior hypogastric plexus is a bilateral structure situated on either side of the rectum, the lower portion of the bladder, and the prostate and seminal vesicles (in males) or the uterine cervix and vaginal fornices (in females) (Fig. 57.4).
Fig. 57.2
(a) Hypogastric plexus. Transverse anatomic section through the spine at L4/5 level revealing the hypogastric plexus, vertebrae, and associated structures. (1) Psoas muscle, (2) iliacus muscle, (3) bifurcation iliac vessels, (4) hypogastric plexus, (5) articulatio intervertebralis, (6) cauda equina (With permission from Danilo Jankovic). (b) Transverse anatomic section. (1) Hypogastric plexus (2) sacrum, (3) sacral canal, (4) sacroiliac joint, (5) iliopsoas muscle, (6) lumbar plexus (With permission from Danilo Jankovic)
At the level of the pelvic inlet, the lumbar part of the sympathetic trunk becomes the sacral part of the sympathetic trunk. This lies behind the parietal peritoneum and the rectum in the parietal pelvic fascia and on the ventral surface of the sacrum immediately medial to the sacral foramina, with the vessels and nerves that course through them. The sacral part of the sympathetic trunk consists of three (but sometimes four or five) sacral ganglia, which have connections with the contralateral ganglia. From the two (or three) cranial ganglia emerge (two or three) sacral splanchnic nerves, with efferent (usually postganglionic) and afferent fibers to the inferior hypogastric plexus. The two sacral sympathetic trunks approach closer to each other caudally and join to form the ganglion impar (Walther ganglion), which is located in front of the coccyx (Fig. 57.3a, b). White rami communicantes are absent, but gray rami communicantes with postganglionic sympathetic fibers course from each of the sacral ganglia to the corresponding spinal nerves in the sacrococcygeal region. Along with branches of the sacrococcygeal plexus, these fibers reach vessels, sweat glands, erector muscles of the hair, cross-striated muscles, bones, and joints (Fig. 57.4).
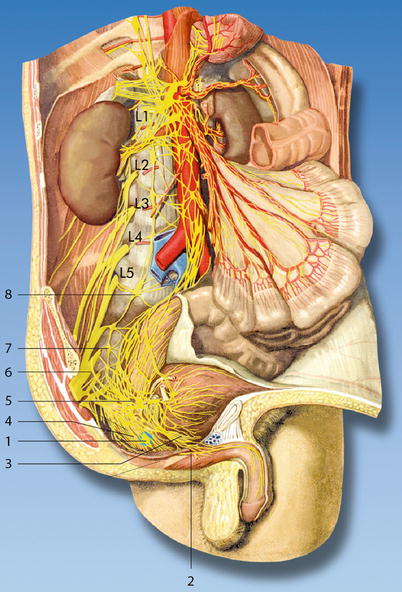
Fig. 57.3
(a) Ventral surface of the sacrococcygeal joint. (1) Ganglion impar (Walther’s ganglion) (With permission from Danilo Jankovic). (b) (1) Ganglion impar, (2) lumbosacral plexus, (3) sacral sympathetic trunk (With permission from Danilo Jankovic)
Fig. 57.4
Sacral ganglia and sacral plexus. (1) Ganglion impar, (2) pudendal nerve, (3) prostatic plexus, (4) rectal plexus, (5) ventral part of the inferior hypogastric plexus, (6) sacral plexus, (7) ganglion of the sympathetic trunk, (8) lumbosacral ganglion of the sympathetic trunk (With permission from Danilo Jankovic)
Superior Hypogastric Plexus Block
Injection of a local anesthetic or neurolytic in the region of the hypogastric plexus (pelvis region), one of the three large sympathetic plexuses.
Indications [4–10]
Diagnostic and Prognostic
1.
Pelvic pain that has been unresponsive to more conservative interventions.
2.
A diagnostic superior hypogastric plexus block may help distinguish between pelvic pain of visceral and somatic origin because it innervates only the pelvic viscera and vasculature; referred pain emanating from somatic structures will be unaffected.
Therapeutic
1.
Neurolysis of the plexus to produce long-lasting pain relief in patients with pelvic cancer (cervical, proximal vaginal, uterine, ovarian testicular, prostatic, and rectal cancers)
2.
Pain of oncologic origin (pain and tenesmus due to radiation injury and rectal anastomosis)
3.
In patients with distal colonic or rectal inflammatory bowel disease
4.
Penile pain after transurethral resection of the prostate
5.
Chronic pelvic pain in the presence of endometriosis
Contraindications
1.
Anticoagulant treatment
2.
Infections and skin diseases in the injection area
Procedure
This block should only be carried out by experienced anesthetists, or under their supervision. Full information should be given to the patient.
Preparations
Check that the emergency equipment is complete and in working order; sterile precautions, intravenous access, ECG monitoring, pulse oximetry, intubation kit, ventilation facilities, emergency medication.
Materials
Fine 26-G needle, 25 mm long, for local anesthesia. Atraumatic 22-G needle, 0.7 × 120–140 mm (15°) with injection lead or spinal needle, 0.7 (0.9) × 120–140 mm (150 mm), 20–22-G syringes: 2, 5, and 10 mL. Disinfectant, swabs, compresses, sterile gloves and drape, flat, and firm pillow.
Patient Positioning
Prone position on a radiographic imaging table: support with a pillow in the lower abdomen (to eliminate lumbar lordosis). The patient’s arms should be dangling. The patient should breathe with the mouth open, to reduce tension in the back muscles. This position is preferable, particularly when the block is carried out under radiographic control using an image intensifier.
Landmarks (Fig. 57.2a, b)
1.
The location of L4–L5 interspace is approximated by palpation of the iliac crests and spinous processes and is then verified by fluoroscopy.
2.
Skin wheals are raised 5–7 cm bilateral to the midline at the level of L4–L5 interspace.
Disinfection, generous local anesthetic infiltration of the injection channel, covering with a sterile drape, drawing up the local anesthetic, and testing the patency of the injection needle.
During the injection, the following points must be observed:
1.
The person carrying out the injection must stand on the side being blocked.
2.
Usually, the injection point should not be located more than 8 cm lateral to the midline and no more than 5 cm medial to it (the lateral side of the vertebra is more difficult to reach).
3.
Paresthesias occur relatively frequently during introduction of the needle and indicate irritation of the lumbar somatic nerves.
4.
There is a risk of perforating the dural cuff if the injection is made too far medially (epidural or subarachnoid injection).
5.
Aspirate frequently and inject incrementally.
6.
No neurolytics should be administered without precise confirmation of the needle position using radiographic control with an image intensifier.
Injection Technique [4–6]
1.
A short-beveled needle with a depth marker is inserted through one of the skin wheals with the needle bevel directed toward the midline. From a position perpendicular in all planes to the skin, the needle is oriented about 30° caudad and 45° medial, so that its tip is directed toward the anterolateral aspect of the bottom of the L5 vertebral body.
The iliac crest and the transverse process of L5, which is sometimes enlarged, are potential barriers to needle passage. If the transverse process of L5 is encountered during advancement of the needle, the needle is withdrawn to the subcutaneous tissue and is redirected slightly caudad or cephalad.
2.



The needle is readvanced until the body of the L5 vertebra is encountered or until its tip is observed fluoroscopically to lie at its anterolateral aspect, at the depth of approximately 10–12.5 cm. If the vertebral body is encountered, gentle effort may be made to further advance the needle.
Related posts:






Full access? Get Clinical Tree
