CHAPTER 156
Subungual Hematoma
Presentation
After a blow or crushing injury to the fingernail or toenail (i.e., stubbing one’s toe or having one’s finger closed in a door), the patient experiences severe throbbing pain that persists for hours. The fingertip is very sensitive, and the fingernail has an underlying deep blue-black discoloration, which may be localized to the proximal portion of the nail or extend beneath its entire surface (Figure 156-1, A and B). The nail margins should be completely intact without any free blood visible.
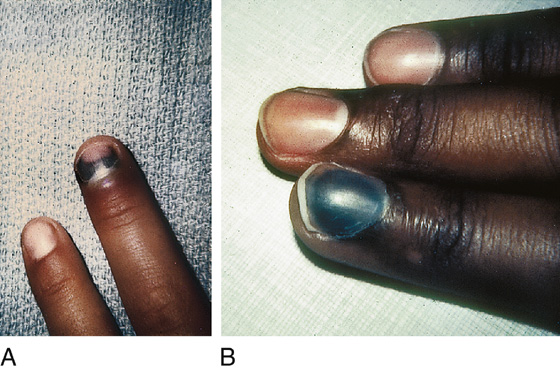
Figure 156-1 A and B, Subungual hematomas.
What To Do:
 Evaluate for possible extensor tendon avulsion (baseball finger) by having the patient fully extend the distal interphalangeal (DIP) joint (see Chapter 108).
Evaluate for possible extensor tendon avulsion (baseball finger) by having the patient fully extend the distal interphalangeal (DIP) joint (see Chapter 108).
 If there is a concern for an underlying fracture, radiographs may be obtained. Comminuted tuft fractures commonly underlie larger subungual hematomas and are helpful in determining the patient’s expected length of pain and possible disability. If the mechanism of injury is clear, it is not necessary to delay nail trephination (see below) before obtaining radiographs.
If there is a concern for an underlying fracture, radiographs may be obtained. Comminuted tuft fractures commonly underlie larger subungual hematomas and are helpful in determining the patient’s expected length of pain and possible disability. If the mechanism of injury is clear, it is not necessary to delay nail trephination (see below) before obtaining radiographs.
 Keep in mind that not all dark patches under the nail are subungual hematomas. Consider the diagnosis of a simple ecchymosis (see Chapter 155), melanoma, Kaposi sarcoma, splinter hemorrhages (often associated with infective endocarditis), and other tumors when the history of trauma and the physical examination are not consistent with a simple subungual hematoma.
Keep in mind that not all dark patches under the nail are subungual hematomas. Consider the diagnosis of a simple ecchymosis (see Chapter 155), melanoma, Kaposi sarcoma, splinter hemorrhages (often associated with infective endocarditis), and other tumors when the history of trauma and the physical examination are not consistent with a simple subungual hematoma.
 If significant pain is present, paint the nail with 10% providone-iodine (Betadine) solution (or equivalent antiseptic) and perform trephination at the base of the nail with an electric cauterizing lance or carbon laser. A single-bevel 18-gauge needle or 23-gauge double bevel may also be used with a boring technique (Figure 156-2).
If significant pain is present, paint the nail with 10% providone-iodine (Betadine) solution (or equivalent antiseptic) and perform trephination at the base of the nail with an electric cauterizing lance or carbon laser. A single-bevel 18-gauge needle or 23-gauge double bevel may also be used with a boring technique (Figure 156-2).
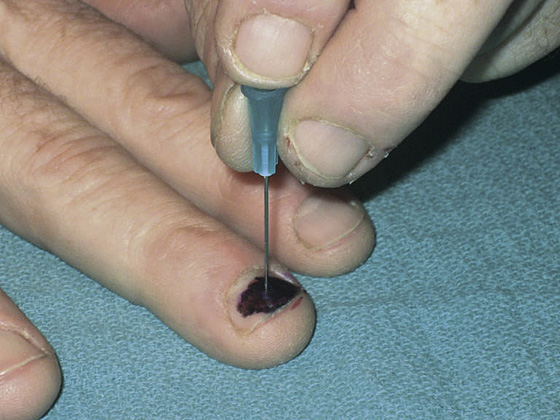
Figure 156-2 Trephination with a sterile, disposable, 23-gauge, double-bevel, 1-inch needle. (From Bonisteel PS: Practice tips. Trephining subungual hematomas. Can Fam Physician 54:693, 2008.)
 When trephination is performed quickly with a hot cauterizing lance or paperclip, patients do not feel the heat before the relief of pressure. Tap rapidly a few times with the cautery or drill in the same spot at the base of the hematoma until the hole is through the nail. When resistance from the nail gives way, stop further downward pressure to avoid damaging the underlying nail bed.
When trephination is performed quickly with a hot cauterizing lance or paperclip, patients do not feel the heat before the relief of pressure. Tap rapidly a few times with the cautery or drill in the same spot at the base of the hematoma until the hole is through the nail. When resistance from the nail gives way, stop further downward pressure to avoid damaging the underlying nail bed.
 Persistent bleeding from this opening can be controlled by simply having the patient hold a folded 4 × 4 gauze pad firmly over the trephination site while holding his hands over his head.
Persistent bleeding from this opening can be controlled by simply having the patient hold a folded 4 × 4 gauze pad firmly over the trephination site while holding his hands over his head.
 Apply an antibacterial ointment, such as Betadine, and cover the trephination site with a Band-Aid.
Apply an antibacterial ointment, such as Betadine, and cover the trephination site with a Band-Aid.
 To prevent infection, instruct the patient to keep his finger protected from soaking in contaminated water for approximately 1 week.
To prevent infection, instruct the patient to keep his finger protected from soaking in contaminated water for approximately 1 week.
 The patient should be instructed to monitor for signs of infection (worsening pain, redness, swelling, red streaking, fevers) and to return immediately if these occur.
The patient should be instructed to monitor for signs of infection (worsening pain, redness, swelling, red streaking, fevers) and to return immediately if these occur.
 A protective aluminum fingertip splint may also be comforting, especially if the bone is fractured (see Chapter 111).
A protective aluminum fingertip splint may also be comforting, especially if the bone is fractured (see Chapter 111).
 If little discomfort is present, when the patient initially seeks care, protective splinting and an analgesic may be all that is required. Be sure to explain to the patient that you are not drilling a hole in his nail to reduce the possibility of infection and that putting a hole in his nail will not provide him with significantly more pain relief. That being said, always allow the patient to select his choice of method(s) for pain relief.
If little discomfort is present, when the patient initially seeks care, protective splinting and an analgesic may be all that is required. Be sure to explain to the patient that you are not drilling a hole in his nail to reduce the possibility of infection and that putting a hole in his nail will not provide him with significantly more pain relief. That being said, always allow the patient to select his choice of method(s) for pain relief.
 Inform the patient that he will eventually lose his fingernail, and a new nail will grow out after 3 to 6 months.
Inform the patient that he will eventually lose his fingernail, and a new nail will grow out after 3 to 6 months.
What Not To Do:
 Do not perform trephination on a subungual ecchymosis (see Chapter 155).
Do not perform trephination on a subungual ecchymosis (see Chapter 155).
 Do not perform a digital block. Anesthesia should not be necessary under most circumstances.
Do not perform a digital block. Anesthesia should not be necessary under most circumstances.
 Do not perform trephination on a patient who is no longer experiencing any significant pain at rest. A mild analgesic and protective splint will usually suffice.
Do not perform trephination on a patient who is no longer experiencing any significant pain at rest. A mild analgesic and protective splint will usually suffice.
 Do not make such a small opening that free drainage does not occur. A slender electrocautery tip may have to be bent to the side or spread apart for it to produce a wide enough hole.
Do not make such a small opening that free drainage does not occur. A slender electrocautery tip may have to be bent to the side or spread apart for it to produce a wide enough hole.
 Do not hold a cautery wire on the surface of the nail without applying enough slight pressure to melt through the nail. Just holding the hot tip adjacent to the nail can heat up the hematoma and increase the pain without making a hole to relieve the pressure.
Do not hold a cautery wire on the surface of the nail without applying enough slight pressure to melt through the nail. Just holding the hot tip adjacent to the nail can heat up the hematoma and increase the pain without making a hole to relieve the pressure.
 Do not send a patient home to soak his finger after trephination. This is unnecessary (there is never reaccumulation of blood), and it may break down the protective fibrin clot and introduce bacteria into this previously sterile space.
Do not send a patient home to soak his finger after trephination. This is unnecessary (there is never reaccumulation of blood), and it may break down the protective fibrin clot and introduce bacteria into this previously sterile space.
 Do not routinely prescribe antibiotics. Even when opening a subungual hematoma with an underlying fracture of the distal phalanx, antibiotics have not been shown to be of any value in preventing infection. A brief course of cephalexin (Keflex) may be justified when treating patients with diabetes and peripheral vascular disease or those who are immunocompromised.
Do not routinely prescribe antibiotics. Even when opening a subungual hematoma with an underlying fracture of the distal phalanx, antibiotics have not been shown to be of any value in preventing infection. A brief course of cephalexin (Keflex) may be justified when treating patients with diabetes and peripheral vascular disease or those who are immunocompromised.
 Do not remove the nail, even with a large subungual hematoma, as long as the nail and nail margins are intact. It is not necessary to inspect for nail bed lacerations or repair them with a closed injury.
Do not remove the nail, even with a large subungual hematoma, as long as the nail and nail margins are intact. It is not necessary to inspect for nail bed lacerations or repair them with a closed injury.
Discussion
The subungual hematoma is a space-occupying mass that produces pain secondary to increased pressure against the very sensitive nail bed and matrix. Given time, the tissues surrounding this collection of blood will stretch and deform until the pressure within this mass equilibrates. Within 24 to 48 hours, the pain therefore subsides. Although the patient may continue to complain of pain with activity, performing trephination at this time may not improve his discomfort to any significant extent and will potentially expose him to a small risk for infection. If trephination is not performed, explain this to the patient, who may be requesting trephination too late. The patient is often the best judge whether the pain is sufficient to warrant taking on this very small risk for infection.
Though many clinicians use a heated paper clip as a cautery device, it may be contraindicated in many settings, because it involves the use of an open flame to heat the material. Many paper clips are also made of metals that do not heat sufficiently to penetrate the nail. However, if it is the only device available, it is usually sufficiently effective (Figure 156-3). An alcohol wipe that is partially pulled from its foil package, when lit with a match, can serve as a readily available flame for heating up a paper clip.
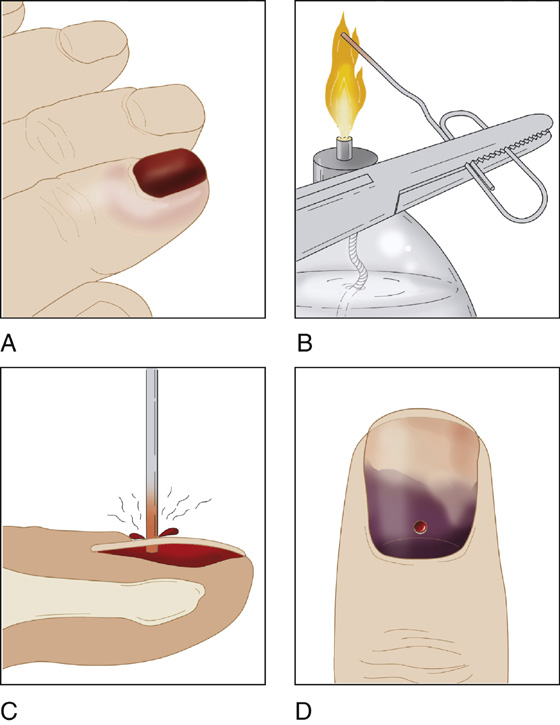
Figure 156-3 Trephination with a red-hot paper clip. A, Subungual hematoma. B, Heating metal. C, Nail trephination. D, Result.
There is some controversy in the literature about whether the nail should be removed if the hematoma occupies greater than 25% to 50% of the nail, because there may be an underlying nail bed laceration. It appears that trephination alone is safe and effective for treating these closed injuries, without apparent risk for infection or significant secondary nail deformity. There is some risk for missing a nail bed laceration under the hematoma but, even if present, splinting the wound by its own nail plate should help heal the underlying laceration.
When there are associated lacerations, open hemorrhage, broken nails, or disruption of the nail plate borders, perform a digital block and remove the nail to inspect the nail bed and repair any lacerations as necessary (see Chapter 146).
Related posts:

Full access? Get Clinical Tree


