AN OVERVIEW OF REHABILITATION
Physical medicine and rehabilitation, also known as physiatry or rehabilitation medicine, is a branch of medicine that aims to enhance and restore functional ability and quality of life to those with physical impairments or disabilities. The development of rehabilitation as a subspecialty, its underlying philosophy, current evidence-based science, and the approach to care have unique characteristics that are discussed in this section.
A Brief History of Rehabilitation
The history of rehabilitation dates back to ancient Egypt in which there are references to adaptive aids and artificial limbs. The first issue of Archives of Physical Medicine and Rehabilitation was published in 1919. World War I had a great impact on rehabilitation because many surviving soldiers sustained amputation injuries and needed care; the Veterans Administration was created to care for those with service-related injuries. In 1938, a small group of physicians lobbied for specialty recognition for physical medicine and rehabilitation. Their efforts resulted in the founding of the American Academy of Physical Medicine and Rehabilitation in 1947. In 1941, Dr. Frank Krusen published the first comprehensive textbook on physical medicine and rehabilitation. In 1943, the Vocational Rehabilitation Act was enacted, providing funds for professional training and research, while at the same time broadening the scope of rehabilitation. This Act was the catalyst for growth in rehabilitation practice. In 1946, the term physiatrist was first used to describe a physician with specialized knowledge in physical medicine and rehabilitation. The Worker’s Compensation Act, which placed an emphasis on the workplace, passed in 1965. In 1973, the Rehabilitation Act passed, demonstrating an increased public awareness of the needs of individuals with disabilities. This act provided guidelines prohibiting discrimination and promoted equal opportunity with the removal of barriers for those with disabilities (Association of Rehabilitation Nurses [ARN], 2011).
In 1990, the Americans with Disabilities Act (ADA) increased accessibility options for individuals with disabilities in the community, employment, education, and health care settings. Finally, after many years of being paid under the Tax Equity and Fiscal Responsibility Act (TEFRA), the payment structure for rehabilitation facilities underwent a major transformation with the implementation of the Inpatient Prospective Payment System in 2002 (ARN, 2011).
A Philosophy of Rehabilitation
A philosophy is a set of broad statements about fundamental beliefs and values. The philosophy of rehabilitation offers a framework to guide the overall rehabilitation process and includes the following concepts.
Rehabilitation is a philosophy of care, not a setting. It is a continuous process that depends on a team approach. The rehabilitation philosophy is founded on the idea that all individuals have inherent worth and have the right to be experts in their own health care (ARN, 2008, 2011; Gender, 1998). The goal of rehabilitation is to assist individuals with a disability and/or chronic illness to restore, maintain, and promote optimal health. Overall health promotion is an important component of rehabilitation for persons with chronic disabling conditions. The rehabilitation process addresses major areas of focus that include prevention, recognition, and management of comorbid conditions; facilitation of maximum coping and adaptation by the patient and family; prevention of secondary disability by promotion of community reintegration including participation in home, family, recreational, and vocational activities; enhancement of quality of life in view of the disability; and prevention of recurrent stroke and other vascular conditions (Leifer et al., 2011; Miller et al., 2010).
Rehabilitation is often defined as the restoration of the person to the highest physical, mental, social, vocational, and economic capacity (World Health Organization [WHO], 2001). Rehabilitation endeavors to prevent further disability, to maintain the patient’s remaining abilities, and to restore lost functions. In all aspects of a disabling injury or disease, a person moves through a period of adjustment and adaptation and then proceeds to restoration. Rehabilitation programs are centered on the philosophy that is geared toward helping the person obtain and maintain his or her optimal functional capability. The philosophy of care reinforces the person’s abilities and motivation to retain the highest level of independence. Integration of restorative interventions is an ongoing process that uses input from the interprofessional team in order to establish the best way or method to optimize the person’s underlying capability and functional performance. Goals are patient-centered and mutually determined between the interprofessional team and the patient and family, with an emphasis on community reentry and integration to minimize deficits, prevent complications, promote wellness, and optimize quality of life.
The Interprofessional Rehabilitation Team
 A variety of team models exist in the rehabilitation setting, including multidisciplinary, interdisciplinary, transdisciplinary, and interprofessional models. These models are described in Chapter 3 and briefly in Table 10-1. The preferred model for the 21st century is the interprofessional practice model. This is the model that sets the framework for discussion of rehabilitation in this chapter. Regardless of the model used in rehabilitation, key characteristics of high-functioning teams include common goals, collaboration, collegiality, trust, mutual respect, cooperation, open communications, patient-centered care, and a commitment to quality outcomes. High-quality stroke care requires a dedicated team of professionals trained in the assessment and treatment of cerebrovascular disease. Evidence suggests that early referral and admission to an organized, interprofessional inpatient rehabilitation program within the first 4 weeks after stroke can result in a decrease in the absolute number of stroke-related deaths (Miller et al., 2010). Additionally, rehabilitation can reduce long-term disability and serve to enhance recovery post stroke (Miller et al., 2010). Many hospitals have developed stroke centers that provide stroke care from the acute hospital through the continuum of care using interprofessional teams who provide coordinated stroke services.
A variety of team models exist in the rehabilitation setting, including multidisciplinary, interdisciplinary, transdisciplinary, and interprofessional models. These models are described in Chapter 3 and briefly in Table 10-1. The preferred model for the 21st century is the interprofessional practice model. This is the model that sets the framework for discussion of rehabilitation in this chapter. Regardless of the model used in rehabilitation, key characteristics of high-functioning teams include common goals, collaboration, collegiality, trust, mutual respect, cooperation, open communications, patient-centered care, and a commitment to quality outcomes. High-quality stroke care requires a dedicated team of professionals trained in the assessment and treatment of cerebrovascular disease. Evidence suggests that early referral and admission to an organized, interprofessional inpatient rehabilitation program within the first 4 weeks after stroke can result in a decrease in the absolute number of stroke-related deaths (Miller et al., 2010). Additionally, rehabilitation can reduce long-term disability and serve to enhance recovery post stroke (Miller et al., 2010). Many hospitals have developed stroke centers that provide stroke care from the acute hospital through the continuum of care using interprofessional teams who provide coordinated stroke services.
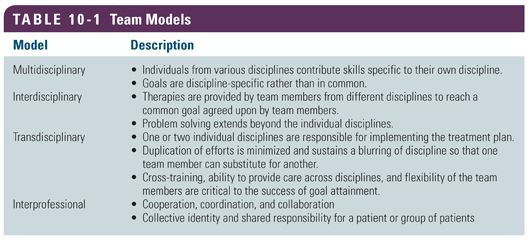
 The interprofessional rehabilitation team provides care that is patient-centered, family-centered, effective, efficient, equitable, timely, safe, and evidence-based. A high level of cooperation, coordination, and collaboration characterize the relationships between professions in delivering patient-centered care. Interprofessional team–based care is care delivered by intentionally created, usually relatively small workgroups in health care who are recognized by others, as well as by themselves, as having a collective identity and shared responsibility for a patient or group of patients, such as stroke patients. Open communications among health providers, the patient, and family are a hallmark of patient-centered care in which the patient and family have an equal voice in care decisions. This concept of relying on the patient and family to have an active voice in care decision is the focus of current research initiatives such as the Patient-Centered Outcomes Research Institute (PCORI, 2014).
The interprofessional rehabilitation team provides care that is patient-centered, family-centered, effective, efficient, equitable, timely, safe, and evidence-based. A high level of cooperation, coordination, and collaboration characterize the relationships between professions in delivering patient-centered care. Interprofessional team–based care is care delivered by intentionally created, usually relatively small workgroups in health care who are recognized by others, as well as by themselves, as having a collective identity and shared responsibility for a patient or group of patients, such as stroke patients. Open communications among health providers, the patient, and family are a hallmark of patient-centered care in which the patient and family have an equal voice in care decisions. This concept of relying on the patient and family to have an active voice in care decision is the focus of current research initiatives such as the Patient-Centered Outcomes Research Institute (PCORI, 2014).
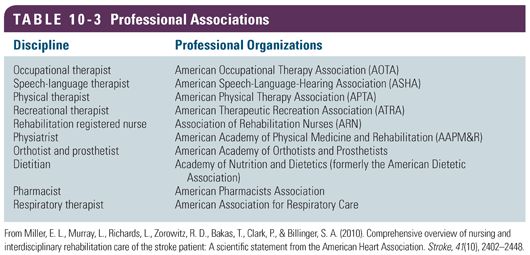
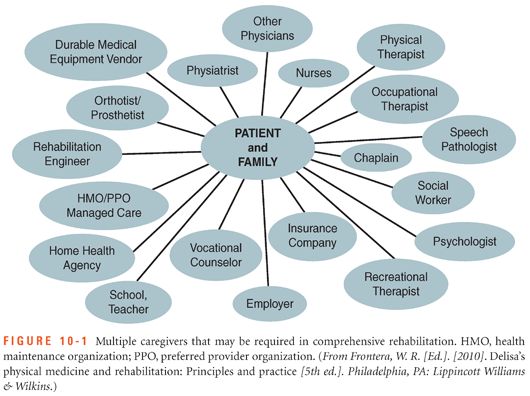
 Interprofessional rehabilitation team members include a variety of health professionals working together to meet the comprehensive needs of a patient. Table 10-2 provides a list of professionals commonly involved in the rehabilitative care of the stroke patient along with their roles. Figure 10-1 depicts an expanded number of caregivers that may be required in comprehensive stroke rehabilitation. In order to practice effectively in interprofessional teams, a new model for educating health professionals is being implemented. The goal of interprofessional education is to “prepare all health professions students for deliberatively working together with the common goal of building a safer and better patient-centered and community/population oriented U.S. health care system” (Interprofessional Education Collaborative Expert Panel, 2011, p. 3). The focus on standards and competencies extends beyond initial professional education. The professional associations for rehabilitation practitioners set and publish standards of care and scope of practice for each specialty (Table 10-3). Many organizations also offer national certification examinations by which professionals demonstrate competency in their specialty area of practice. National certification may be required for legal authority to practice in a state. These organizations emphasize the need for developing and maintaining ongoing interprofessional practice competencies for contemporary practice.
Interprofessional rehabilitation team members include a variety of health professionals working together to meet the comprehensive needs of a patient. Table 10-2 provides a list of professionals commonly involved in the rehabilitative care of the stroke patient along with their roles. Figure 10-1 depicts an expanded number of caregivers that may be required in comprehensive stroke rehabilitation. In order to practice effectively in interprofessional teams, a new model for educating health professionals is being implemented. The goal of interprofessional education is to “prepare all health professions students for deliberatively working together with the common goal of building a safer and better patient-centered and community/population oriented U.S. health care system” (Interprofessional Education Collaborative Expert Panel, 2011, p. 3). The focus on standards and competencies extends beyond initial professional education. The professional associations for rehabilitation practitioners set and publish standards of care and scope of practice for each specialty (Table 10-3). Many organizations also offer national certification examinations by which professionals demonstrate competency in their specialty area of practice. National certification may be required for legal authority to practice in a state. These organizations emphasize the need for developing and maintaining ongoing interprofessional practice competencies for contemporary practice.

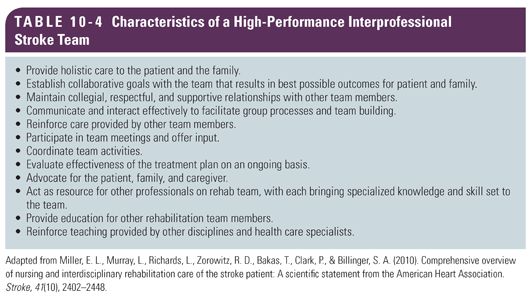
 The interprofessional team approach in rehabilitation has been identified as critical to achieving and maximizing patient outcomes for patients with stroke (Miller et al., 2010). Table 10-4 lists the characteristics of a high-performance interprofessional team.
The interprofessional team approach in rehabilitation has been identified as critical to achieving and maximizing patient outcomes for patients with stroke (Miller et al., 2010). Table 10-4 lists the characteristics of a high-performance interprofessional team.
A Theoretical Framework for Rehabilitation
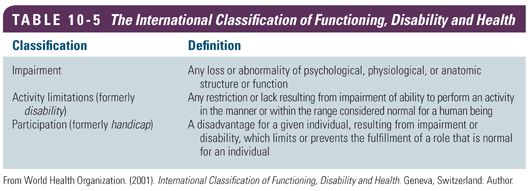
Because of the complexity and heterogeneity of stroke in the rehabilitation setting, a commonly applied framework in conceptualizing residual stroke deficits is provided by WHO. The International Classification of Functioning, Disability and Health is commonly referred to as the ICF. The ICF framework and its concepts have existed for over 25 years and use a biopsychosocial approach to human functioning and disability (WHO, 2001), as shown in Table 10-5. This framework transcends individual disciplines and provides a cross-cultural framework (Tempest & McIntyre, 2006). With the ICF, functioning is viewed as a distinct and separate concept. Functioning refers to “limitations and restrictions related to a health problem” (Cieza et al., 2005, p. 212). The ICF model is a means to view an individual and his or her interactions with the environment and everyday functioning (McIntyre & Tempest, 2007). The dynamic and interactive components of the model provide a viable, theoretical framework applicable to rehabilitation practice. According to Kearney and Pryor (2004), clinicians should prevent and minimize impairments, enable activities, prevent and minimize activity limitations, and enable participation.  In order to do this, the interprofessional team must first understand the social aspect of disability and the impact that health professionals can have in reducing stigmas and barriers to an individual’s overall function.
In order to do this, the interprofessional team must first understand the social aspect of disability and the impact that health professionals can have in reducing stigmas and barriers to an individual’s overall function.
Rehabilitation focuses on activities to optimize functioning and health. For example, an individual with a stroke may have dysphagia and hemiplegia. These impairments may result in activity limitations in bathing, dressing, and other self-care activities and impact on roles or participation within the family and society such as employment or being a church participant. The ICF framework is useful in rehabilitation because it can be used by the  interprofessional team to address the complex needs of stroke survivors and their reintegration into the community.
interprofessional team to address the complex needs of stroke survivors and their reintegration into the community.
 Rehabilitation professionals must adopt a social understanding of disability so that communication between disciplines can occur effectively. In addition, the ICF framework guides interventions, promotes collaboration among disciplines, and serves to guide future research. One of the strengths of the ICF is to help plan interventions to meet specific functional goals that are relevant for an individual to resume activities and become an active member within society. A common framework is needed for health professionals to communicate about function, health, and disability—both within a discipline as well as across disciplines. The ICF framework serves as such a model (Cieza et al., 2005).
Rehabilitation professionals must adopt a social understanding of disability so that communication between disciplines can occur effectively. In addition, the ICF framework guides interventions, promotes collaboration among disciplines, and serves to guide future research. One of the strengths of the ICF is to help plan interventions to meet specific functional goals that are relevant for an individual to resume activities and become an active member within society. A common framework is needed for health professionals to communicate about function, health, and disability—both within a discipline as well as across disciplines. The ICF framework serves as such a model (Cieza et al., 2005).
Evidence-Based Practice and Clinical Practice Guidelines for Rehabilitation
Evidence-based practice (EBP) is defined as use of the best scientific knowledge and research evidence available to guide practice, along with expert opinion and patient and family values and preferences. EBP and clinical practice guidelines (CPGs) are used to support clinical decision making in the rehabilitation setting (Miller et al., 2010). CPGs are systematically developed statements to assist practitioners in making appropriate evidence-based decisions for specific clinical circumstances such as in the care of the patient with stroke. CPGs define the specific assessment parameters, diagnostic and treatment modalities, treatment options, and management strategies and contain recommendations based on evidence from a systematic review and synthesis of the published health care literature (Miller et al., 2010). The major organizations such as the American Heart Association (AHA) and the American Stroke Association (ASA) provide information about the rigor of the process involved in preparing their CPGs.  In 2010, the AHA/ASA published CPGs specific to interprofessional rehabilitative stroke care. Although a comprehensive summary of the guidelines is beyond the scope of this chapter, the guidelines serve as evidence-based framework for the interprofessional team caring for the patient with stroke across the entire continuum. CPGs are also useful in providing a framework to plan, implement, and evaluate stroke rehabilitation programs at a population level. For example, CPGs specific to urinary incontinence in stroke set a standard for stroke rehabilitation programs to conduct a comprehensive assessment of premorbid bladder function, identify the type of poststroke incontinence present, and initiate a behavioral bladder training program specific to the type of incontinence present (Miller et al., 2010).
In 2010, the AHA/ASA published CPGs specific to interprofessional rehabilitative stroke care. Although a comprehensive summary of the guidelines is beyond the scope of this chapter, the guidelines serve as evidence-based framework for the interprofessional team caring for the patient with stroke across the entire continuum. CPGs are also useful in providing a framework to plan, implement, and evaluate stroke rehabilitation programs at a population level. For example, CPGs specific to urinary incontinence in stroke set a standard for stroke rehabilitation programs to conduct a comprehensive assessment of premorbid bladder function, identify the type of poststroke incontinence present, and initiate a behavioral bladder training program specific to the type of incontinence present (Miller et al., 2010).
The Stroke Care Continuum
 The stroke care continuum begins with community outreach focused on screening for early detection of risk factors that can lead to a stroke. Educational programs teach patients, providers, and emergency response teams to recognize the symptoms of stroke. Many stroke teams use stroke protocols to facilitate rapid diagnosis and intervention (The Joint Commission [TJC], 2014). Emergency departments (EDs) work with emergency medical systems to ensure that stroke patients are identified when in route to the ED. Stroke teams facilitate rapid diagnosis and intervention to address acute stroke management and include early involvement of rehabilitation professionals. Stroke units with interprofessional care including early rehabilitation accelerate recovery and reduce complications. Rehabilitation management should be integrated throughout stroke recovery.
The stroke care continuum begins with community outreach focused on screening for early detection of risk factors that can lead to a stroke. Educational programs teach patients, providers, and emergency response teams to recognize the symptoms of stroke. Many stroke teams use stroke protocols to facilitate rapid diagnosis and intervention (The Joint Commission [TJC], 2014). Emergency departments (EDs) work with emergency medical systems to ensure that stroke patients are identified when in route to the ED. Stroke teams facilitate rapid diagnosis and intervention to address acute stroke management and include early involvement of rehabilitation professionals. Stroke units with interprofessional care including early rehabilitation accelerate recovery and reduce complications. Rehabilitation management should be integrated throughout stroke recovery.
 FUNCTIONAL DEFICITS COMMONLY SEEN IN STROKE PATIENTS
FUNCTIONAL DEFICITS COMMONLY SEEN IN STROKE PATIENTS
Initiating rehabilitation early after the stroke is associated with improved function post stroke. A strategy for whole body rehabilitation consisting of minimizing or interrupting sedation and beginning physical and occupational therapy in the earliest days of critical illness is safe and well tolerated and results in better functional outcomes at hospital discharge, a shorter duration of delirium, and more ventilator-free days compared with standard care (Schweickert et al., 2009). Because of the heterogeneity and complexity of stroke, residual deficits are often observed in patients with a diagnosis of stroke.  In order to facilitate the recovery process, the interprofessional team must identify, assess, treat, and evaluate each individual patient’s unique clinical deficits and build a treatment plan that is tailored to address these issues. Common deficits typically observed in stroke patients are described in greater detail in the following section.
In order to facilitate the recovery process, the interprofessional team must identify, assess, treat, and evaluate each individual patient’s unique clinical deficits and build a treatment plan that is tailored to address these issues. Common deficits typically observed in stroke patients are described in greater detail in the following section.
Activities of Daily Living Deficits
Description and Assessment
An estimated 50 million stroke survivors have significant physical, cognitive, and emotional deficits; 25% to 74% of these survivors require some assistance or are fully dependent on caregivers for activities of daily living (ADL) (Anderson, Linto, & Stewart-Wynne, 1995; Kalra & Langhorne, 2007). ADL are activities that are conducted routinely in daily life such as eating, dressing, grooming, bathing, and toileting. They are commonly measured in rehabilitation using the Functional Independence Measure (FIM) instrument (Bottemiller, Bieber, Basford, & Harris, 2006; Keith, Granger, Hamilton, & Sherwin, 1987; Ottenbacher, Hsu, Granger, & Fiedler, 1996). In recent publications, functional status, particularly ADL, was found to have an effect on hospital readmissions. DePalma et al. (2013) reported that unmet ADL needs and transitions involving coping with functional disability are correlated with increased hospital readmissions. This finding is further supported by Arbaje et al. (2008) who found that patients with two hospitalizations within 60 days of discharge had reported at least one unmet ADL need prior to the first hospitalization.
Treatment and Evaluation
In many respects, all rehabilitation modalities and goals should aim to improve ADL. Functional status measured in ADL, including sleep routines and medication management into daily routines, should be integrated into the treatment plan for stroke patients beginning with the acute hospitalization and extending through rehabilitation into the postdischarge setting. Any plan to improve ADL function should be incorporated into the patient’s daily routine along the continuum of care to the home environment. Rehabilitation interventions for ADL include use of adaptive equipment for dressing, bathing, and showering; use of durable medical equipment as applicable, including raised toilet seats and tub or bath chairs/benches; integration of dressing techniques such as one-handed method and/or use of adaptive equipment; and use of adaptive equipment for ADL such as feeding, hygiene, grooming, eating, and ambulation.
Clinical Pearl: Functional status, particularly unmet ADL needs, was found to have an effect on hospital readmissions. Addressing ADL needs is important during the rehabilitation process.
Skin Management
Description and Assessment
Stroke patients are at risk for problems with skin integrity from redness to pressure ulcers due to a number of contributing factors such as immobility, loss of sensation, poor circulation, and presence of pressure, friction or shear; incontinence; decreased sensory perception; hemiparesis or hemiplegia; older age; and altered awareness or consciousness (Miller et al., 2010). Frequent monitoring of skin integrity is imperative beginning in the acute hospital setting through rehabilitation and transition to the community setting. There are many scales available to assess skin integrity. The Braden Scale is frequently used across hospital and rehabilitation settings and may be helpful to determine patients at high risk for skin breakdown and target interventions to the high-risk patient (Miller et al., 2010).
Treatment and Evaluation
The key elements involved in perpetuating skin breakdown are pressure, friction, and shearing forces. Interventions aimed at decreasing skin breakdown should target minimizing pressure by altering positions frequently as well as minimizing friction and shearing forces on the skin. Intact skin integrity is critical for success of the rehabilitation process without secondary complications of reddened or open areas, which can impede the patient’s rehabilitation and recovery. Characteristics of a successful skin management program includes intact skin with no reddened areas or broken skin and the patient or caregiver understanding the implications of a good skin management program and how to implement such a plan.
The following interventions can assist to maintain skin integrity (Miller et al., 2010):  maintain adequate hydration and nutrition; teach patient skin care and weight-shifting strategies; reposition patient every 2 hours; avoid excessive friction, pressure, and shearing when moving patient; keep patient skin clean and dry; use pressure-relieving devices, such as gel mats or cushions, as applicable; educate family and caregivers on proper skin care prior to discharge; and consult with other interprofessional team members, as needed, such as the nutritionist to promote optimal healing if any broken area exists.
maintain adequate hydration and nutrition; teach patient skin care and weight-shifting strategies; reposition patient every 2 hours; avoid excessive friction, pressure, and shearing when moving patient; keep patient skin clean and dry; use pressure-relieving devices, such as gel mats or cushions, as applicable; educate family and caregivers on proper skin care prior to discharge; and consult with other interprofessional team members, as needed, such as the nutritionist to promote optimal healing if any broken area exists.
Clinical Pearl: Exercise vigilance in checking the skin integrity of stroke patients, especially those who are using devices such as splints and orthoses.
Cognitive Deficits
Description and Assessment
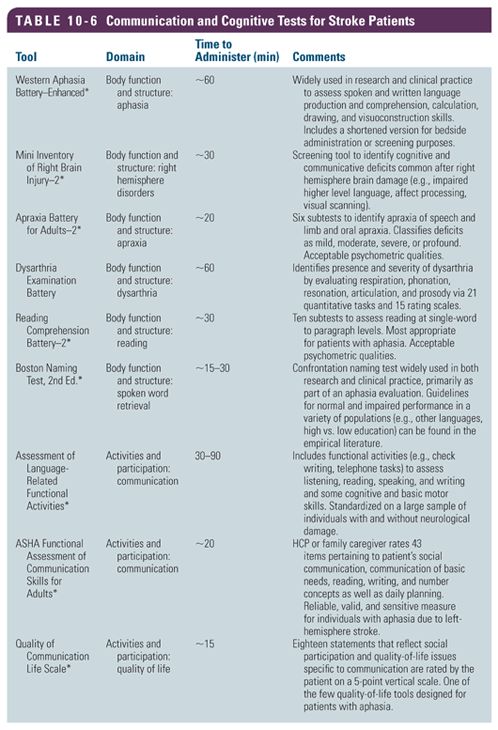
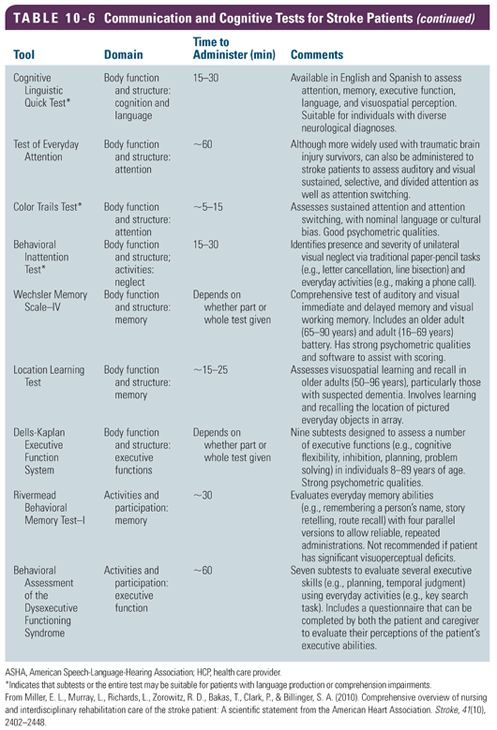
Cognitive impairment is a common problem for stroke survivors (Leys, Henon, Mackowiak-Cordoliani, & Pasquier, 2005; Linden, Skoog, Fagerberg, Steen, & Blomstrand, 2004). A study by Serrano, Domingo, Rodriguez-Garcia, Castro, and Del Ser (2007) found that in a sample of 327 stroke patients, 12.6% had cognitive impairment. The nature and degree of cognitive impairment that occurs after a stroke depends on the location and size of the stroke. Stroke resulting in damage to the left hemisphere may result in difficulty with language skills and loss of memory. Damage to the right hemisphere may result in difficulties with attention, thinking, and behavior. Damage to the frontal lobe of the brain may cause difficulty in the ability to control and organize thoughts and behavior, resulting in difficulty with executive function including thinking through the steps of a complex task (Cicerone, Levin, Malec, Stuss, & Whyte, 2006; Sohlberg et al., 2007). Cognitive impairment is associated with decreased ability to perform ADL and instrumental activities of daily living (IADL) (Salter, Teasell, Bitensky, Foley, & Bhogal, 2014). A number of tools are available to assess the extent and nature of cognitive impairment post stroke. Table 10-6 provides a summary of communications and cognitive assessment tools.
Treatment and Evaluation
The primary goal of cognitive rehabilitation is to improve deficits in order to optimize safety, daily functioning, independence, and quality of life. In developing a cognitive rehabilitation program, it is important to identify all areas of cognitive impairment and to develop a coordinated plan to address each deficit area. Therefore, multiple assessment tools may be necessary to complete a cognitive evaluation. Additionally, patients may be referred to a neuropsychologist for a formal evaluation of cognitive deficits.
Cognitive rehabilitation involves a systematic, functionally oriented provision of therapeutic activities that is based on assessment and understanding of the patient’s cognitive deficits (Cicerone et al., 2000). Interventions should reinforce or strengthen previously learned patterns, establish new patterns of cognitive activity through compensatory cognitive mechanisms or establish new patterns of activity through external compensatory mechanisms through environmental structuring and support, and finally enable patients to adapt to their cognitive deficits.
Cognitive rehabilitation is associated with three stages of treatment: acquisition, application, and adaptation (Sohlberg & Mateer, 2001). Acquisition involves teaching the purpose and treatment strategy that were chosen. This phase helps patients recognize and accept deficits as well as understand the benefits of treatment. Problem orientation and awareness is addressed in this stage and allows patients to recognize and understand the deficits and rationale for receiving cognitive treatment. The next phase, application, is aimed to improve the effectiveness and independence in compensating for deficits as well as promotion of internalizations of strategies, that is, reduced reliance on external cues. This stage is associated with provision of practice and gradual removal of cues to help the patient learn to apply the strategy. That is, the therapist provides structure, practice, and repetition to help optimize the patient’s ability to use external aids or other strategies in functional tasks. The final stage is adaptation, which promotes transfer of training to tasks including those that are less structured, more novel, complex, and/or distracting. This stage promotes the generalization of skills from a structured therapy approach to less structured environments such as home, community, and work.
 Within rehabilitation teams, it is important to establish which interprofessional team member will administer cognitive tests because these deficits fall under the expertise of various team members (Turkstra, Coelho, & Ylvisaker, 2005). Neurocognitive rehabilitation may include the expertise of psychology, neuropsychology, speech-language pathology, and occupational therapy. For stroke patients, rehabilitation interventions aimed at improving cognitive impairment may include assisting with designing a routine, such as doing activities or tasks at specified times during the day; breaking down tasks into steps; putting things away in the same place or in a familiar place; integrating compensatory strategies such as a memory book or journaling; and integrating internal versus external cues into daily activities.
Within rehabilitation teams, it is important to establish which interprofessional team member will administer cognitive tests because these deficits fall under the expertise of various team members (Turkstra, Coelho, & Ylvisaker, 2005). Neurocognitive rehabilitation may include the expertise of psychology, neuropsychology, speech-language pathology, and occupational therapy. For stroke patients, rehabilitation interventions aimed at improving cognitive impairment may include assisting with designing a routine, such as doing activities or tasks at specified times during the day; breaking down tasks into steps; putting things away in the same place or in a familiar place; integrating compensatory strategies such as a memory book or journaling; and integrating internal versus external cues into daily activities.
Clinical Pearl: Development of a cognitive rehabilitation program should identify all areas of cognitive impairment in order to develop a coordinated plan to address each deficit area.
Communications Deficits
Description and Assessment
Communication includes the ability to receive, send, process, and comprehend concepts including verbal, nonverbal, and graphic symbol systems. Communication disorders may be seen in the process of hearing, language, and/or speech (American Speech-Language-Hearing Association [ASHA], 1993). Speech disorders are impairments of the articulation of speech sounds, fluency, and/or voice. Language disorders are impairments in comprehension, both verbal and nonverbal. Language disorders involve the forms of language including the sound system (phonology), the structure of words (morphology), the order and combination of words (syntax), the content of language (semantics), and the function of language used in communication (pragmatics). Common communication disorders seen after stroke include aphasia and dysarthria, although the pathophysiological basis for each is different.
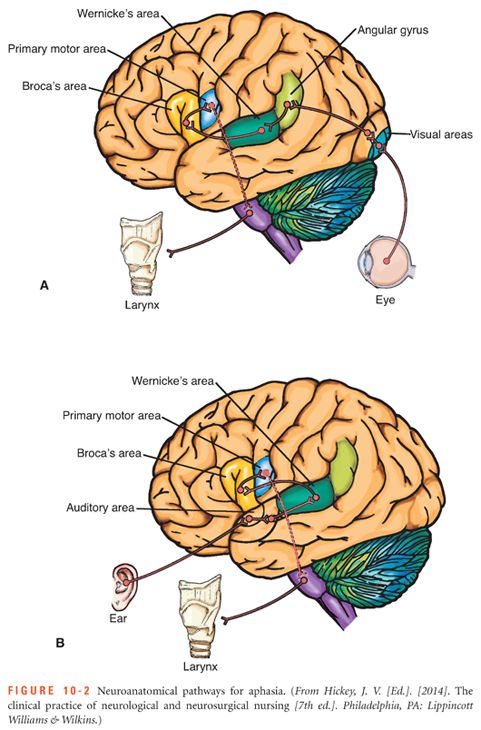
Aphasia is a disturbance in the comprehension and formulation of language and results from damage to the language centers of the brain, usually located in the left hemisphere. Aphasia is seen in 16% to 37% of patients with an acute stroke (Engelter et al., 2006; Kauhanen et al., 2000; Tsouli, Kyritsis, Tsagalis, Virvidaki, & Vemmos, 2009; Wade, Hewer, & David, 1986) which accounts for approximately 100,000 new cases of aphasia in the United States each year (Damasio, 1992). Aphasia is one of the most common poststroke disorders because the middle cerebral artery (MCA) supplies the language centers and is a common site of ischemic stroke. Figure 10-2 shows the neuroanatomy associated with aphasia. Aphasia significantly impacts quality of life in patients and is associated with decreased socialization, depression, and impairment in overall communications (Kauhanen et al., 2000; Wade et al., 1986). Severity of aphasia is a strong predictor of long-term mortality and need for assistance in stroke patients (Tsouli et al., 2009).
Clinical aphasia, as a central neurological disturbance of language, is an impairment of language that is characterized by paraphrasing, word-finding difficulty, and impaired comprehension. It affects the production or comprehension of speech including the ability to read and write (National Aphasia Association, 2014). A classification system, called the Boston classification system, is often used to classify the types of aphasia. The Boston Diagnostic Aphasia Examination 3rd edition (BDAE-3) is a collection of tools that assist the practitioner to identify and determine disorders of language function and neurologically recognized aphasia syndromes. The BDAE is a neuropsychological battery that is used to evaluate adults who have suspected aphasia and evaluates language skills that are based on auditory, visual, and gestural modalities; processing functions including comprehension, analysis, and problem solving; and response modalities including writing, articulation, and manipulation (Spreen & Risser, 2003).
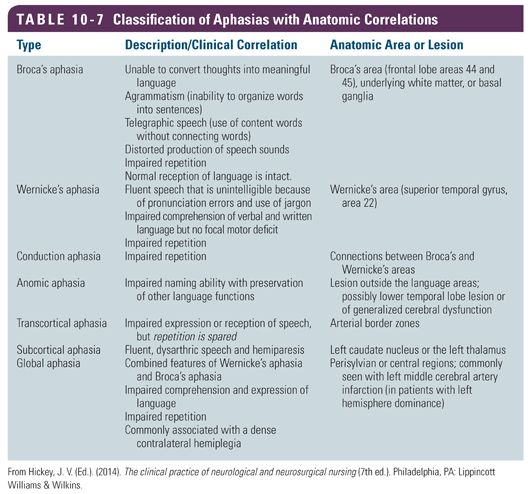
Most common types of aphasia include Wernicke’s aphasia, Broca’s aphasia, and global aphasia. Table 10-7 shows a classification of aphasia and descriptions. Broca’s aphasia or expressive aphasia is difficulty in expressing thoughts into words and involves difficulty stringing words together to form complete sentences (Beeson & Robey, 2006). Wernicke’s aphasia or receptive aphasia involves difficulty with understanding spoken language (Beeson & Robey, 2006). Global aphasia includes difficulty in both understanding and forming words and sentences and is associated with a large left hemispheric stroke. Global aphasia is more common in the acute period after a stroke and affects approximately 25% to 32% of patients with stroke (Laska, Hellblom, Murray, Kahan, & Von Arbin, 2001). Patients with anomic or amnesic aphasia have difficulty in using the correct names for particular objects, people, places, or events.
A growing body of research indicates a significant relation between neuroplastic changes and language recovery (Johansson, 2000; Thompson, 2000). Neuroplasticity is the ability of the nervous system to respond to intrinsic or extrinsic stimuli by reorganizing its structure, function, and connections (Cramer et al., 2011). This research suggests that a major purpose of rehabilitation is to maximize neural plasticity and lead to functional communication gains. The degree and rate of recovery from aphasia varies based on the type and severity of the aphasia, with initial severity associated with poorer outcome (Ferro, Mariano, & Madureira, 1999; Laska et al., 2001). Recovery patterns for aphasia may vary from resolution within the first few days to months or years. Patterns of recovery include spontaneous recovery within the first few days, weeks, and months. This is improvement that occurs as the brain heals from a stroke. Improvement in aphasia recovery can be characterized by progression in communication skills, with the majority of improvement in the areas of auditory comprehension and spontaneous word production. In the first 6 months following a stroke, fluent aphasia patients made the most gains, whereas those with global aphasia made the least amount of gains. In the same study, in the second part of the first year, fluent aphasia showed the least amount of improvement, whereas the most improvement was in the global aphasia group (Sarno & Levita, 1979). Some studies suggest that improvement in language abilities may occur years later following the neurologic injury (Holland, Greenhouse, Fromm, & Swindell, 1989; Kendall et al., 2006), that is, neuroplasticity of the brain enhances the ability of the brain to rewire itself and provides the ability of recovery to extend for months or years. Intensity of therapy over a short period of time may improve the outcomes of speech and language therapy for stroke patients with aphasia (Bhogal, Teasell, & Speechley, 2003).
Other neurogenic speech disorder includes apraxia and dysarthria. Speech apraxia is characterized by an erroneous production of speech sounds, reduced rate of speech, and disorders of prosody, also known as the rhythm and intonation of speech (Wambaugh, Duffy, McNeil, Robin, & Rogers, 2006). Dysarthria is characterized by slurred, slow, and difficult-to-understand speech (Yorkston, Hakel, Beukelman, & Fager, 2007). It accounts for nearly a quarter of outpatient consults to the speech-language pathologist (Mackenzie, 2011). Even though dysarthria is a common symptom in cerebral ischemia, minimal information on its anatomic specificity and associated characteristics as well as etiologic mechanisms is known (Urban et al., 2000). Recently, Canbaz, Celebisoy, Ozdemirkiran, and Tokucoglu (2010) found that the majority of lesions associated with dysarthria were located in the corona radiata followed by pontine lesions. Further, dysarthria prognosis in this study was greatest in the infratentorial lesions on the right side (Canbaz et al., 2010).
Treatment and Evaluation
Aphasia rehabilitation is often led by a speech-language pathologist, also known as a speech therapist and should be provided as early as possible.
Constraint-induced therapy, most frequently used in motor weakness rehabilitation, has also been applied to aphasia rehabilitation. In this case, constraint means avoiding the use of compensatory strategies and forcing the use means communication by talking only (Cherney, Patterson, Raymer, Frymark, & Schooling, 2008). Effectiveness of low-frequency repetitive transcranial magnetic stimulation (rTMS) and intensive speech therapy in poststroke patients with aphasia is a potentially useful neurological rehabilitation technique (Abo et al., 2012). Transcranial magnetic stimulation (TMS) is a noninvasive procedure that used magnetic fields to create electric currents in discrete brain areas (Wasserman et al., 2008). Application of rTMS with the appropriate frequency, intensity, and duration can lead to increases or decreases of excitability of the affected cortex (Pascual-Leone, Davey, Wasserman, Rothwell, & Puri, 2002); in chronic stroke patients, left hemisphere activation has been associated with improved language, and new right hemisphere activation has been observed following speech-language pathology intervention (Cornelissen et al., 2003; Richter, Miltner, & Straube, 2008). Other strategies for rehabilitation professionals to integrate into interventions for patients who have communication difficulties include the following: have patients speak in short sentences; have patients use gestures in addition to speaking; if unable to speak, use communication board strategies or other alternative technology applications; use writing or pictures to ensure that the patient has understood the message; allow additional time for the patient to speak; and be sensitive to the frustration or sense of loss the patient may experience.
Clinical Pearl: Use a normal voice tone when speaking to the patient with aphasia.
Visual Deficits
Description and Assessment
Vision impairments occur frequently after stroke across a spectrum of domains and severities. As many as 87% of stroke patients will manifest some variation of oculomotor dysfunction (Ciuffreda et al., 2007). Oculomotor dysfunction includes nystagmus; abnormalities of vision including saccades, with vergence abnormalities the most common; convergence insufficiency; accommodation; and eye alignment. Other symptoms include difficulty tracking objects (Ciuffreda et al., 2007). Oculomotor-based vision intervention includes oculomotor learning, which is a more specific aspect of motor learning; visual attention and visual field deficits that involve saccadic tracking across midline; remapping of visual space; and localization (Kapoor, Ciuffreda, & Suchoff, 2001; Karnath, Himmelbach, & Kuker, 2003). Hemianopsia, or loss of a visual field on one side of the visual field, is detected in 36% of patients with right hemisphere lesions and in 25% of patients with left hemisphere lesions (Stone, Halligan, & Greenwood, 1993). Binocular vision dysfunction is common after stroke (Wolter & Preda, 2006). Binocular vision involves coordination of the eye muscles that control eye movement. When eye muscles are not properly aligned, the eyes must allow significant corrections to maintain fusion and minimize diplopia (Wolter & Preda, 2006).
The functional implications of visual system malfunction may significantly limit recovery. Visual dysfunction limits progress during the standard rehabilitation continuum of care and decreases overall quality of life (Papageorgiou et al., 2007; Riggs, Andrews, Roberts, & Gilewski, 2007). Stroke-related visual problems include eye movement disorders such as eye deviation, visual field deficits such as hemianopsia or quadrantanopia, reduced visual acuity, and visual inattention or neglect (Pollack et al., 2012). Visual neglect usually occurs after right temporal or parietal stroke.
Treatment and Evaluation
The need for visual rehabilitation is increasingly recognized as a critical element of poststroke rehabilitation. Neurovisual rehabilitation focuses on restitution, compensation, and/or substitution for the visual deficit (Kerkhoff, 2000). Compensation provides a system that will expand the visual field but does not improve internal function. Rehabilitation focuses on the development of abilities through a visual motor–oriented approach that will stimulate the internal neurological system to interact more efficiently with the environment. Visual field deficits may be treated using compensation techniques including head turning or the use of prism glasses. The use of optical devices such as hemianoptic prisms can improve outcomes in patients with homonymous hemianopsia. Hemianoptic prism spectacles enhance peripheral awareness by projecting the picture from the decreased visual field into the functioning visual field (Gottlieb & Miesner, 2004). Prisms affect spatial representation by causing the optical deviation of the visual field; that is, prisms produce changes in orientation with corresponding shifts in both eye movements. Optically, prisms bend light rays toward the base, causing an apparent shift of the image toward the apex from the viewpoint of the observer. The most common type of prism is the Fresnel membrane lenses or prisms that are cemented onto the lens surface. The prism is located outside the residual field of view when the person looks straight ahead. Prism segments are used to expand the upper and lower quadrants. To expand the upper quadrant of the field, the base-out prism segment is placed at the upper part of the glasses on the side of the field loss (e.g., left lens for left hemianopia) (Gottlieb & Miesner, 2004).
Partial or total visual occlusion is an option to eliminate the symptoms of double vision for treatment of binocular dysfunction. Total occlusion is accomplished with a patch by either alternating the patch between the two eyes, covering the eye that has a decrease in visual acuity, or covering the eye with better vision to increase the function of the more limited eye. Partial occlusion is accomplished using the patient’s prescription glasses or on a pair of frames without lenses. Opaque tape is placed over the lens of the nondominant eye starting on the nasal side of the lens and moving laterally until the patient is no longer seeing double. Elimination of double vision through either partial or full occlusion can assist with a patient’s ability to perform ADL (Wolter & Preda, 2006).
Perceptual deficits include the ability to organize, process, and interpret incoming visual information. Perceptual deficit rehabilitation includes the “transfer of training approach” and the “functional approach” (Edmans, Webster, & Lincoln, 2000). The transfer of training approach asserts that practice during ADL on a perceptual task will improve performance. The functional approach strives to promote functional independence through the use of repetitive practice in ADL. Visual impairment is common in stroke patients and is a major factor in one’s ability to conduct daily functions. It is important to increase awareness about visual problems because vision and vision-related deficits are often underassessed and undertreated (Wolter & Preda, 2006). An association between vision impairment and ADL has been established.
 A treatment plan should be developed by the interprofessional team. Occupational therapists have specialized knowledge in visual rehabilitation and visual adaptive devices (Horowitz, 2004; Wolter & Preda, 2006). Interventions include the following: integration of compensation or rehabilitation in ADL including repetition; incorporation of scanning activities including heading turning and the use of verbal or tactile cues; visual inattention or neglect treatment; and integration of prisms and/or patching into daily tasks, as prescribed by a vision specialist, often carried out by the occupational therapist or other interprofessional team members.
A treatment plan should be developed by the interprofessional team. Occupational therapists have specialized knowledge in visual rehabilitation and visual adaptive devices (Horowitz, 2004; Wolter & Preda, 2006). Interventions include the following: integration of compensation or rehabilitation in ADL including repetition; incorporation of scanning activities including heading turning and the use of verbal or tactile cues; visual inattention or neglect treatment; and integration of prisms and/or patching into daily tasks, as prescribed by a vision specialist, often carried out by the occupational therapist or other interprofessional team members.
The rehabilitation needs of patients with vision deficits vary considerably. The level of care and disciplines required are based on the complexity of the problems, goals, and attributes of the patient. The first step is to identify patients with vision-related difficulties after a stroke and to quantify their visual deficits. Specific elements that should be included in the evaluation of vision rehabilitation are visual function, assessment of the patient’s ability to perform tasks requiring vision, assessment of cognitive and psychological status, assessment of risks to the patients due to their visual loss or impairment combined with any other comorbid conditions, and assessment of the potential to benefit from rehabilitation. This includes understanding of the vision impairments and impact on daily activities, safety, and environmental barriers such as lighting or home safety (American Academy of Ophthalmology Vision Rehabilitation Committee, 2012). The overall goal of vision intervention is to eliminate or lessen visual problems in order to reduce the frequency and severity of the patient’s signs and symptoms limiting participation in daily activities due to vision-related problems (Wolter & Preda, 2006).
Clinical Pearl: Early identification of vision and integration into the rehabilitation program assists with ADL performance.
Dysphagia
Description and Assessment
Stroke is one of the most common causes of dysphagia in the adult population, with 42% to 67% of patients presenting with dysphagia within 3 days of a stroke. Fifty percent of these patients aspirate, and about one third who aspirate develop pneumonia (Hinchey et al., 2005). Dysphagia is a disorder of swallowing. Dysphagia and other swallowing dysfunctions may range from physical difficulty of bringing the food to the mouth to manipulation of food in the mouth. Dysphagia may also result from cognitive deficits from surgical intervention, neurological impairments, structural problems, and positioning problems that impact feeding, eating, and swallowing (Cox et al., 2006; Roberts, Cox, Schubert, & Gentry, 2009).
 Dysphagia is a problem that is often seen and addressed by the interprofessional team. The consequences of dysphagia include dehydration, aspiration pneumonia, and airway obstruction (Palmer, Drennan, & Baba, 2000). In assessing the patient for dysphagia, a clinical swallowing evaluation is often completed by a swallowing therapist or speech therapist at the bedside. Many clinical swallowing evaluations rely on the patient to have overt signs of potential aspiration such as coughing or a wet sound when phonating (Terre & Mearin, 2006). The primary drawback of the clinical swallowing evaluation is not being able to detect silent aspiration (Daniels et al., 1998; Smith, Logemann, Colangelo, Rademaker, & Pauloski, 1999). Instrumental evaluations of swallowing are used to provide additional information to assist in the management of dysphagia. The most common tests include the modified barium swallow (MBS), which is a specialized test using a moving x-ray to evaluate a swallowing disorder. This information is used to select the safest diet and any specific compensatory modifications that may be needed. Fiberoptic endoscopic evaluation of swallowing (FEES) is a specialized test using a small camera inserted through the nose to the throat to evaluate swallowing. As with the MBS, the information is used to determine the best diet and compensatory modifications for safe oral intake.
Dysphagia is a problem that is often seen and addressed by the interprofessional team. The consequences of dysphagia include dehydration, aspiration pneumonia, and airway obstruction (Palmer, Drennan, & Baba, 2000). In assessing the patient for dysphagia, a clinical swallowing evaluation is often completed by a swallowing therapist or speech therapist at the bedside. Many clinical swallowing evaluations rely on the patient to have overt signs of potential aspiration such as coughing or a wet sound when phonating (Terre & Mearin, 2006). The primary drawback of the clinical swallowing evaluation is not being able to detect silent aspiration (Daniels et al., 1998; Smith, Logemann, Colangelo, Rademaker, & Pauloski, 1999). Instrumental evaluations of swallowing are used to provide additional information to assist in the management of dysphagia. The most common tests include the modified barium swallow (MBS), which is a specialized test using a moving x-ray to evaluate a swallowing disorder. This information is used to select the safest diet and any specific compensatory modifications that may be needed. Fiberoptic endoscopic evaluation of swallowing (FEES) is a specialized test using a small camera inserted through the nose to the throat to evaluate swallowing. As with the MBS, the information is used to determine the best diet and compensatory modifications for safe oral intake.
There are four main phases in the swallowing process. See Figure 9-1. The first phase is the oral preparatory phase in which the food is chewed, mixed with saliva, and then formed into a cohesive bolus. The second phase is the oral phase in which the food is moved in the mouth from the front to the back with a squeezing action performed primarily with the tongue. The third phase is the pharyngeal phase, which begins with the trigger of the swallow. In this phase, when the food enters the upper throat area, the soft palate elevates, and the epiglottis seals off the trachea. The tongue moves backward and the pharyngeal wall moves forward. These actions assist with moving the food downward to the esophagus. The final phase is the esophageal phase in which the food bolus enters the esophagus and transports the food directly to the stomach through a squeezing action of the throat muscles (Logemann, 1998).
Treatment and Evaluation
It is important to address swallowing problems because they impact on quality of life and place the patient at risk for complications from aspiration. Eating and drinking are key functions to basic survival and are part of daily activities including social events that relate to relationships, acceptance, entertainment, and ADL. Disordered swallow function is associated with aspiration pneumonia and increased mortality rates (Miller et al., 2010). Evidence is lacking regarding interventions to improve swallow, and research is needed to further guide this field of rehabilitation. Interventions commonly employed by the interprofessional team to address dysphagia include (Miller et al., 2010) ongoing swallow assessment, as discussed earlier; encouragement of self- feeding; employment of low-risk feeding strategies such as modified diet consistency, reduced distractions while eating, eating while seated, and slow eating with small bites of food; employment of airway protection strategies such as chin tuck or head rotation while swallowing; electric stimulation; and electromyography biofeedback.

Full access? Get Clinical Tree


