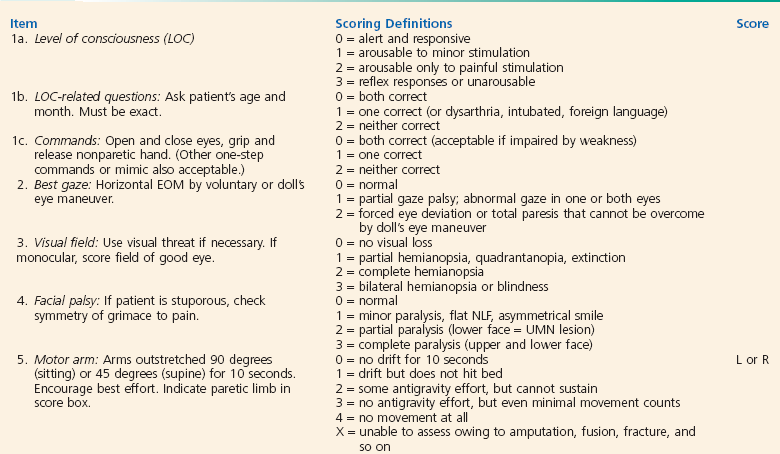
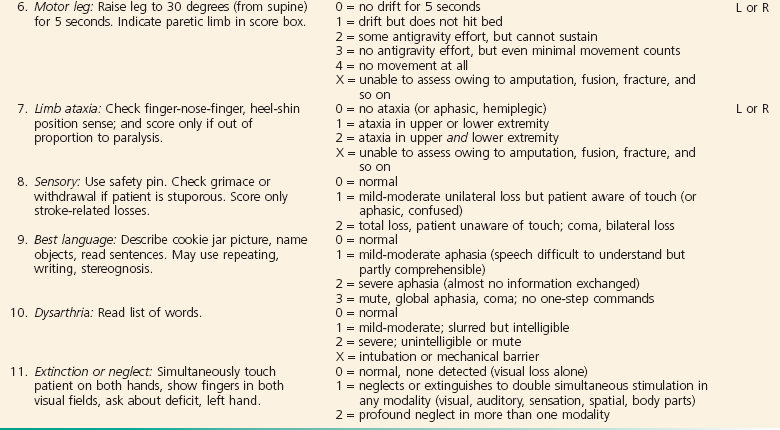
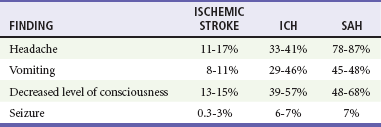
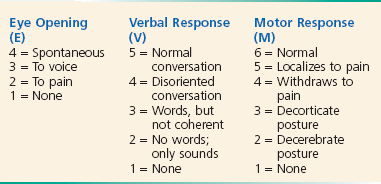
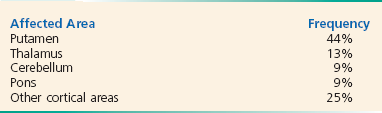
Chapter 101 Stroke is the third leading cause of death in the United States and a leading cause of long-term disability.1 It affects about 795,000 people per year. On average, someone has a stroke every 40 seconds, and someone dies of a stroke every 4 minutes.2 Stroke patients have an in-hospital mortality rate of 5 to 10% for ischemic stroke and 40 to 60% for intracerebral hemorrhage (ICH).3 Only 10% of stroke survivors will recover completely. The remaining survivors will be left with an impairment that will often necessitate rehabilitation.4 The estimated direct and indirect cost of stroke in the United States in 2010 was $73.7 billion.2 Stroke can be defined as any vascular injury that reduces cerebral blood flow (CBF) to a specific region of the brain, causing neurologic impairment. The onset of symptoms may be sudden or stuttering, often with transient or permanent loss of neurologic function. Approximately 87% of all strokes are ischemic in origin, caused by the occlusion of a cerebral vessel.2 Approximately 13% are hemorrhagic strokes caused by the rupture of a blood vessel into the parenchyma of the brain (ICH) or into the subarachnoid space (subarachnoid hemorrhage [SAH]).2 Only ischemic stroke and ICH are discussed in this chapter. An estimated 610,000 “first-ever” ischemic strokes occur each year in the United States.2 These may result either from in situ thrombosis or embolic obstruction from a more proximal source, usually the heart. In more than one third of these first-ever strokes, no clear cause is identified5–7 (Table 101-1). Table 101-1 Data from Woo D, et al: Incidence rates of first-ever ischemic stroke subtypes among blacks: A population-based study. Stroke 30:2517, 1999; and Petty GW, et al: Ischemic stroke subtypes: A population-based study of incidence and risk factors. Stroke 30:2513, 1999. Lacunae, or small-vessel strokes, involve small terminal sections of the vasculature and more commonly occur in African Americans and patients with diabetes and hypertension.5 A history of hypertension is present in 80 to 90% of patients who experience lacunar strokes. The subcortical areas of the cerebrum and brainstem often are involved. The infarcts range in size from a few millimeters to 2 cm and are seen most commonly in the basal ganglia, thalamus, pons, and internal capsule. They may be caused by small emboli or by a process termed lipohyalinosis, which occurs in patients with hypertensive cerebral vasculopathy. Although nearly 20 lacunar syndromes have been described, the most common of these lacunar syndromes are pure motor strokes, pure sensory strokes, or ataxic hemiparesis. Because they are subcortical and well localized, lacunar strokes do not typically cause cognitive impairment, aphasia, or simultaneous sensorimotor findings. One fourth of all ischemic strokes are cardioembolic in nature.5,6 Embolization of a mural thrombus in patients with atrial fibrillation is the most common mechanism, and patients with atrial fibrillation have an approximate fivefold increased risk for development of a stroke.8 In addition, roughly 45% of all embolic strokes occur as a result of atrial fibrillation.8 Noncardiac sources of emboli may include diseased portions of extracranial arteries, resulting in an artery-to-artery embolus. One common example is amaurosis fugax, in which emboli from a proximal carotid artery plaque embolizes to the ophthalmic artery, causing transient monocular blindness. Another cause of stroke is recent myocardial infarction (MI). Approximately 12 ischemic strokes occur per 1000 nonfatal MI patients within 1 month after the index event. Furthermore, 11 ischemic strokes occur per 1000 nonfatal MI patients in the post-MI hospitalization period. Independent predictors of stroke after acute MI are advanced age, diabetes, hypertension, history of previous stroke, anterior location of index MI, previous MI, atrial fibrillation, heart failure, and nonwhite race.9 The use of aspirin has been shown to reduce the incidence of post-MI stroke by 46%.10 Carotid and vertebral dissections often are associated with trauma but may follow such mild events as turning the head sharply. Carotid and vertebral dissections also are seen more frequently in people with underlying pathology of the vessel wall, such as in fibromuscular dysplasia and connective tissue disorders. Alteration in the vessel intima can lead to vessel stenosis, occlusion, or embolism. The patient may report a minor preceding event such as spinal manipulation, yoga, working overhead, coughing, or vomiting. Presenting manifestations may include headache, facial pain, visual changes, cranial nerve (CN) palsies, pain over the affected vessel, Horner’s syndrome, amaurosis fugax, SAH, or an ischemic stroke. The headache frequently is unilateral and may occur days before onset of the other neurologic symptoms.11 Although angiography has been the standard diagnostic study, dissections are increasingly being diagnosed by less invasive modalities such as ultrasonography, magnetic resonance angiography (MRA), and computed tomography angiography (CTA).12 Medical therapy includes early anticoagulation if SAH is not suspected. If symptoms recur despite anticoagulation, the patient may be eligible for endovascular intervention. Carotid or vertebral dissection is not considered a contraindication to use of tissue plasminogen activator (tPA) in the eligible patient.13 This entity is considered a major cause of stroke in younger patients.11,14,15 A transient ischemic attack (TIA) was historically defined as a neurologic deficit with complete resolution within 24 hours. However, advances in neuroimaging suggest that many such events represent minor stroke with resolved symptoms rather than true TIAs.16 Therefore the American Heart Association (AHA) recommends the following definition: a transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction.17 From 200,000 to 500,000 TIAs per year are diagnosed in the United States, and emergency department (ED) visits for TIA occur at a rate of about 1 visit per 1000 population.16 TIAs constitute an important warning sign for the future development of cerebral infarction. Approximately 10% of the patients who experience a TIA will experience a stroke within 3 months of the sentinel event, and one half of these occur within the first 2 days.18 Spontaneous ICH causes 10 to 15% of all acute strokes, affecting approximately 65,000 patients per year.19 It carries a 30-day mortality rate of up to 50%, with one half of patients dying in the first 2 days. Among survivors, only 1 in 5 are living independently at 6 months.3 The two major underlying causes of ICH are hypertensive vasculopathy (caused by long-standing hypertension) and cerebral amyloid angiopathy (usually found in elders, the result of amyloid deposition in cerebral vessel walls). Hypertensive hemorrhage results from degenerative changes in the small penetrating arteries and arterioles, leading to lipohyalinosis of small, deep penetrating arteries. Such hemorrhages generally occur in the deep regions including basal ganglia and thalamus. The most common sites for hypertensive hemorrhage are listed in Box 101-1. ICH caused by amyloid angiopathy tends to be lobar in nature and to occur more commonly in elders. Specific apolipoprotein E alleles appear to predispose to the development and recurrence of ICH. Other factors leading to ICH include underlying vascular malformations, including arteriovenous malformations (AVMs) and aneurysms, drug intoxication (particularly sympathomimetics, such as cocaine), malignant hypertension, saccular aneurysms, blood dyscrasias, venous sinus thrombosis, hemorrhagic transformation of an ischemic stroke, moyamoya disease, and tumors. High-risk features for such secondary forms of ICH include lobar location, presence of intraventricular blood, and younger age.20 The cerebral vasculature supplies the brain with a rich flow of blood that contains the critical supply of oxygen and glucose necessary for normal brain function. When a stroke occurs, there are immediate alterations in CBF and extensive changes in cellular homeostasis. The normal CBF is approximately 40 to 60 mL/100 g of brain per minute. When CBF drops below 15 to 18 mL/100 g of brain per minute, several physiologic changes occur. The brain loses electrical activity, becoming electrically “silent,” although neuronal membrane integrity and function remain intact. Clinically, the areas of the brain maintaining electrical silence manifest a neurologic deficit, even though the brain cells are viable. When CBF is below 10 mL/100 g of brain per minute, membrane failure occurs, with a subsequent increase in the extracellular potassium and intracellular calcium and eventual cell death. The ischemic penumbra is the area of the brain surrounding the primary injury, which is preserved by a tenuous supply of blood from collateral vessels. This border zone of neuronal tissue is the area of greatest interest to investigators for possible salvage in both ischemic and hemorrhagic stroke. In ischemic stroke, the duration of occlusion plays a critical role in neuronal survival.21 Increasing the duration of occlusion increases both the irreversibility of deficits and the amount of cerebral infarction. Thus, ischemic stroke trials typically focus on the first few hours after symptom onset. In ICH, acute vessel rupture is most often caused by underlying small vessel disease, as noted earlier, and causes injury by several mechanisms. First, there is mass effect from the hematoma itself, followed by activation of the coagulation cascade, release of inflammatory cytokines, and blood-brain barrier (BBB) disruption. This leads to perihematomal edema formation and secondary brain injury. Finally, continued bleeding, or hematoma expansion, occurs in many patients—either continued bleeding from the primary source or secondary bleeding at the periphery of the hemorrhage.19 The National Institutes of Health Stroke Scale (NIHSS) is a useful and rapid tool for quantifying neurologic deficit in patients with stroke and can be used in determining treatment options22 (Box 101-2). NIHSS scores have been shown to be reproducible and valid and to correlate well with the amount of infarcted tissue on CT scan.23,24 The baseline NIHSS score can identify patients who are appropriate candidates for fibrinolytic therapy as well as those at increased risk for hemorrhage. In addition, it has been used as a prognostic tool to predict outcome and is currently being used by some stroke centers to stratify patients for entry into treatment trials.22 BOX 101-2 National Institutes Of Health (NIH) Stroke Scale Scoring Form EOM, extraocular movement; L, left; NLF, nasolabial fold; R, right; UMN, upper motor neuron. Modified from online document. Massachusetts General Hospital Stroke Service. NIH stroke scale materials. Scoring form. Available at http://www2.massgeneral.org/stopstroke/pdfs/scoring_form.pdf. Accessed March 6, 2013. The classic presentation of ICH is the sudden onset of headache, vomiting, severely elevated BP, and focal neurologic deficits that progress over minutes. Similar to ischemic stroke, ICH is often associated with a motor and sensory deficit contralateral to the brain lesion. Almost 40% of patients will demonstrate significant growth in hemorrhage volume within the first few hours.25 Although headache, vomiting, and coma are common, many patients do not have these findings, and the clinical presentation can be identical to that of patients with ischemic stroke; the two cannot reliably be differentiated in the absence of neuroimaging (Table 101-2). Table 101-2 Data from Bogousslausky J, Van Melle G, Regli F: The Lausanne Stroke Registry: Analysis of 1000 consecutive patients with first stroke. Stroke 19:1083, 1988; Foulkes MA, et al: The Stroke Data Bank: Design, methods, and baseline characteristics. Stroke 19:547, 1988; and Mohr JP, et al: The Harvard Cooperative Stroke Registry: A prospective registry. Neurology 28:754, 1978. As with ischemic stroke, a careful neurologic examination is important in localizing the region and extent of injury. Baseline NIHSS and Glasgow Coma Scale (GCS) scores can be used to assess stroke severity, although the GCS score may be more feasible to follow for neurologic deterioration (Box 101-3). In addition, serial examinations can detect early changes that may suggest ongoing bleeding during the acute phase. BOX 101-3 Glasgow Coma Scale Shoestring Graphics. Glasgow coma score. Available at http://www.ssgfx.com/CP2020/medtech/glossary/glasgow.htm. Accessed March 6, 2013. Poor prognostic indicators for patients with ICH include a decreased level of consciousness on arrival, intraventricular hemorrhage, and large ICH volume, all of which can be assessed in the ED. The ABC/2 technique is a quick and accurate method of measuring ICH volume at the bedside26 (Fig. 101-1). One validated tool to predict outcome is the ICH score (Box 101-4)21: Patients are given 0 to 2 points for GCS score, 1 point for age over 80, 0 to 2 points for ICH volume, 1 point for presence of intraventricular blood, and 1 point for hemorrhage location. This score has been shown to predict short- and long-term mortality. BOX 101-4 Intracerebral Hemorrhage (ICH) Score Predicting Mortality after Acute ICH 30-Day Mortalities for Total ICH Scores Adapted from Hemphill JC, et al: The ICH Score. Stroke 32:891-897, 2001. Venous sinus thrombosis is another cause of focal neurologic symptoms that most commonly affects the superior sagittal sinus and lateral sinuses (see Chapter 105). The diagnosis of cerebral venous thrombosis can be difficult because of the nonspecific nature of symptoms, as well as the variable time frame of symptom onset (from hours to a few weeks). Patients may have generalized headaches, nausea, vomiting, paresis, visual disturbances, depressed level of consciousness, seizures or even symptoms generally ascribed to psychiatric disorders (such as depression).27 Depending on the location of the thrombus, physical examination of the patient may reveal papilledema, proptosis, or palsies of CNs III, IV, and VI, as well as other focal neurologic signs and symptoms.27 Multiple risk factors predisposing affected patients to venous sinus thrombosis are recognized, including trauma, infectious processes, hypercoagulable states, low-flow states, compression of the venous sinus, dehydration, various drugs (such as androgens, “ecstasy,” and oral contraceptives), and pregnancy or the postpartum state.
Stroke
Perspective
Epidemiology
STROKE SUBTYPE
ESTIMATED NUMBER
Large vessel
69,000 (16%)
Small vessel/lacunae
76,000 (17.5%)
Cardioembolic
113,000 (26%)
Stroke of uncommon mechanisms
15,000 (3.5%)
Infarction of unknown cause
157,000 (36.5%)
Total strokes and TIAs
430,000 (100%)
Hemorrhagic Stroke
Principles of Disease
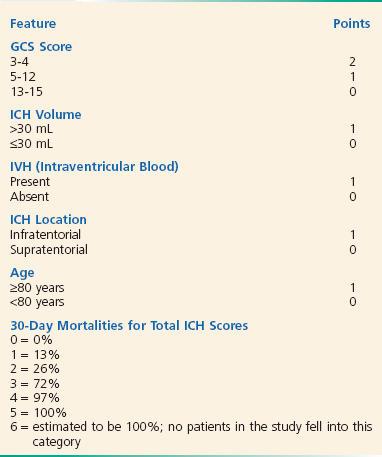
Clinical Features
Hemorrhagic Stroke
Differential Considerations






Full access? Get Clinical Tree


