Fig. 13.1
The cervical ganglion trunk: (1) superior cervical ganglion, (2) middle cervical ganglion, and (3) cervicothoracic ganglion (With permission from Danilo Jankovic)
Fig. 13.2
Paramedian sagittal dissection (head and thorax): (1) stellate ganglion, (2) the subclavian artery, (3) the vertebral artery, (4) pleura, (5) the brachial plexus, (6) the carotid artery, (7) the vagus nerve, (8) clavicle, (9) V. brachiocephalica (With permission from Danilo Jankovic)
Fig. 13.3
The immediate vicinity of the stellate ganglion: (1) pleura, (2) brachial plexus, (3) vagus nerve, (4) recurrent laryngeal nerve, (5) trachea (With permission from Danilo Jankovic)
Fig. 13.4
Close anatomical connections in the ganglion trunk include those to (1) the phrenic nerve, (2) the recurrent laryngeal nerve, (3) the vagus nerve, and (4) the brachial plexus (With permission from Danilo Jankovic)
Fig. 13.5
Fibers from the gray rami communicantes (circles) supply the heart, esophagus, airways, and thymus (With permission from Danilo Jankovic)
Fig. 13.6
The immediate vicinity of the ganglion (transverse section). (1) First rib, (2) subclavian artery and scalenus anterior muscle, (3) jugular vein, (4) second rib, (5) cervicothoracic ganglion, (6) common carotid artery and thyroid gland, (7) T2 intervertebral artery and zygapophyseal joint, (8) T2 vertebral body, (9) spinal medulla. The average size of the cervicothoracic ganglion is 25 mm × 3–10 mm × 5 mm (With permission from Danilo Jankovic)
Fig. 13.7
Course of the phrenic nerve (circle shows the end position of the phrenic nerve) (With permission from Danilo Jankovic)
Fig. 13.8
Positions of (1) the recurrent laryngeal nerve and (2) the vagus nerve (With permission from Danilo Jankovic)
Fig. 13.9
Risk of intravascular injection into (1) the vertebral artery, (2) the inferior thyroid artery, (3) the carotid artery, and (4) first intercostal artery (With permission from Danilo Jankovic)
Traditional Approach for SGB
The most widely practiced approach to SGB is the anatomic-landmark- or fluoroscopy-guided paratracheal approach, in which the needle is inserted toward the anterior tubercle of the sixth (Chassaignac tubercle) cervical vertebra (Figs. 13.10 and 13.11). This approach is essentially a blockade of the cervical sympathetic chain in proximity to the middle cervical ganglion instead of the stellate ganglion, which is located opposite to the neck of the first rib. Thus, the classical approach is a cervical sympathetic trunk block rather than SGB.

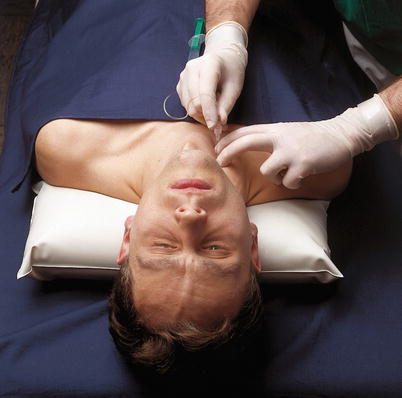
Fig. 13.10
Two-finger method of locating the level of C7 (With permission from Danilo Jankovic)
Fig. 13.11
Introducing the needle (With permission from Danilo Jankovic)
There are significant limitations and potential hazards associated with traditional approaches. The cephalocaudal extent of the Chassaignac tubercle can be as narrow as 6 mm [13], and it can be easily missed with needle advancement with conventional techniques.
Possible consequences of non-ultrasound-guided approaches for SGB are:
1.
Potential for penetration of vascular structures and intravascular injection:
Retropharyngeal and cervicomediastinal hematomas after SGB has been reported despite negative aspiration of blood, and these can cause severe airway compromise [10, 20, 26]. Kapral et al., in one of the earliest papers examining US guidance, reported hematomas in three out of 12 patients who received SGB without US guidance [14]. Possibility of other arteries at risk (e.g. the ascending cervical branch of the inferior thyroid artery, transverse cervical artery) that traverse over the C6 anterior tubercle has also been mentioned [18]. Siegenthaler and colleagues found that the vertebral or other arteries were located in the needle path for traditional approach for SGB in over 28 % of subjects [22], while Bhatia and colleagues reported that a major vessel was observed in up to 29 and 43 % of patients at the C6 and C7 levels, respectively. It was also noted that the vertebral artery was outside the foramen transversarium in 7 % of subjects at the C6 level [2], and this has also been shown in other studies [4, 16]. A modified fluoroscopy-guided oblique approach has been proposed to reduce the risk of vertebral artery puncture as the needle is directed to the junction of the uncinate process and the vertebra body [1]. However, this technique directs the needle much closer to the esophagus (see below).
2.
Potential for penetration of esophagus, pleura, lateral lobes of thyroid gland, and cervical nerve roots:
Two recent studies have indicated that the esophagus is frequently located in the needle path of SGB performed using traditional approaches. The esophagus was located along the needle path in 37–50 % and 65–74 % of subjects at the C6 and C7 levels, respectively, in these studies [2, 22]. The risk of esophageal penetration is greater than on the left side because of the anatomical location of the esophagus. Esophageal puncture can result in mediastinitis especially if the patient has an unrecognized diverticulum.
Pneumothorax is also a potential complication with anatomic-landmark- or fluoroscopy-guided techniques, especially if SGB is performed at the C7 level. Finally, a needle traversing through the thyroid gland can result in a hematoma, and exiting cervical nerve roots can also be traumatized during SGB.
Use of ultrasound enables the operator to visualize blood vessels, esophagus, pleura, nerve roots, and thyroid, and this can help avoid penetration of these structures [3, 17].
In addition to the risks of potential complications with traditional approaches for SGB, precision in deposition of the injectate and adequacy of its spread to the first and second thoracic vertebral levels are key considerations for ensuring efficacy. The location of CST is in the loose connective tissues of the prevertebral fascia. However, traditional approaches rely on contact with bony landmarks (transverse processes of C6 or C7) followed by withdrawal of the needle by a few millimeters and then injection. The spread of injectate with these approaches has been shown to be anterior to the prevertebral fascia and in the paratracheal space in most patients, without much caudal spread [12], whereas subfascial injection results in more caudal spread, higher rate of sympathetic block of the upper limbs, and lower incidence of blockade of vagus or recurrent laryngeal nerve (causing hoarseness) [5, 21].
Sonoanatomy and Injection Technique for Ultrasound-Guided Stellate Ganglion Block
The patient is placed in the semi-lateral position with the procedure side nondependent and the neck in slight extension. A high-frequency linear US probe (6–15 MHz) is used and a probe with a small footprint is desirable. The probe placed transversely at the level of cricoid cartilage and the transverse process (TP) of the cervical vertebra is identified. If the TP has a prominent anterior tubercle and a smaller posterior tubercle, then this is likely to be the C6 level, but scanning should be continued in a caudal direction to allow recognition of the TP at C7 level that has only a posterior tubercle. The vertebral artery can easily be identified in cross section, its location being deeper and lateral to the common carotid artery at C7 level. Once the TP of the C6 vertebra has been identified, the longus colli muscle is identified in cross section (Fig. 13.12). This muscle is located anterior to the TP and medial to the anterior tubercle and is around 1 cm thick at this level [9]. The prevertebral fascia on the anterior surface of the muscle deep to the longus capitis muscle is then identified. Other important structures to recognize include the lateral lobe of the thyroid gland, blood vessels including the common carotid artery and the internal jugular vein, esophagus, exiting cervical nerve root, and any vessels that may be in the planned path of the injecting needle (Figs. 13.13 and 13.14).