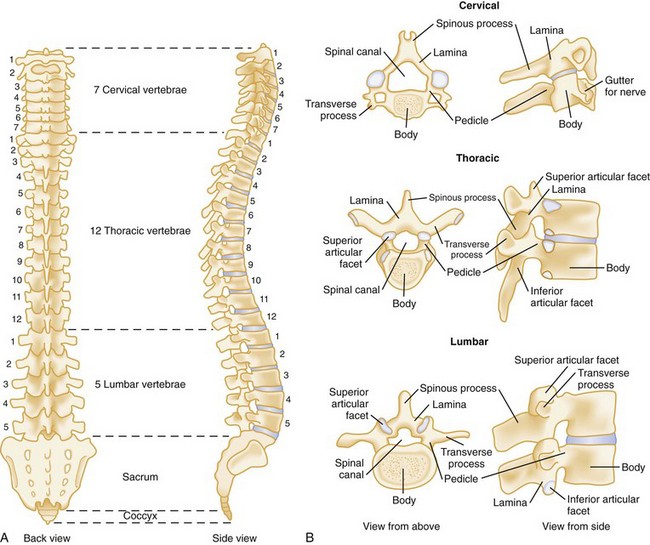
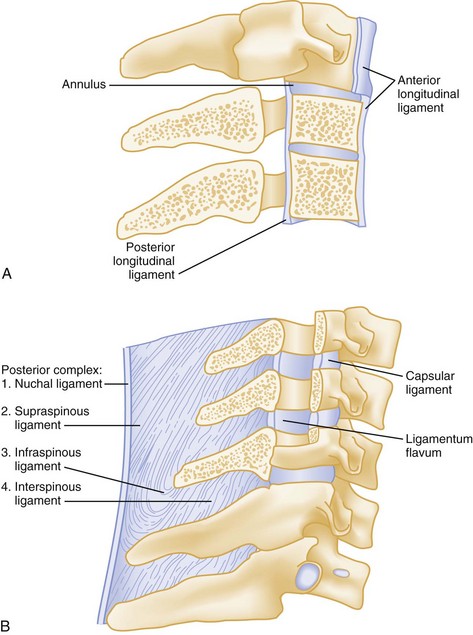
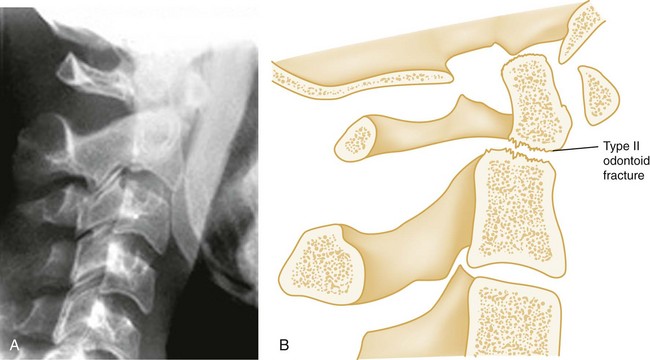
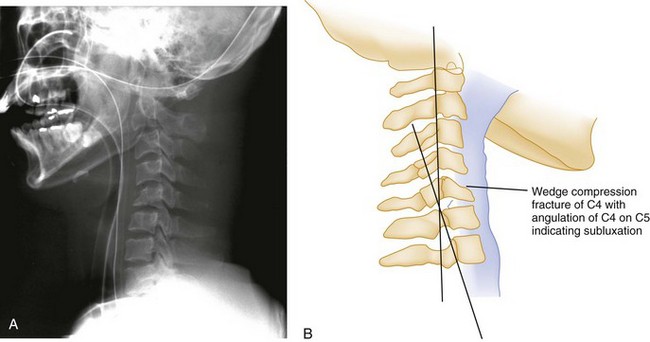
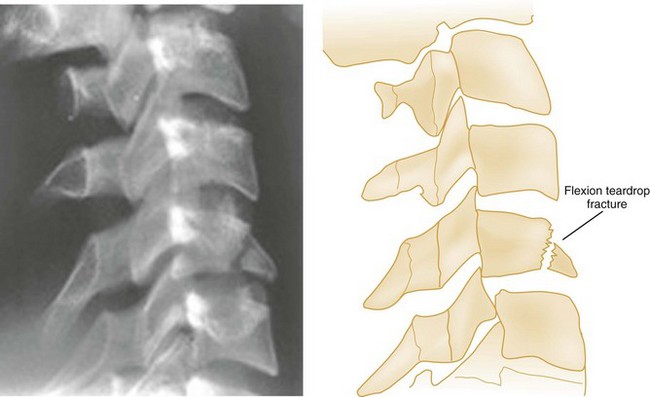
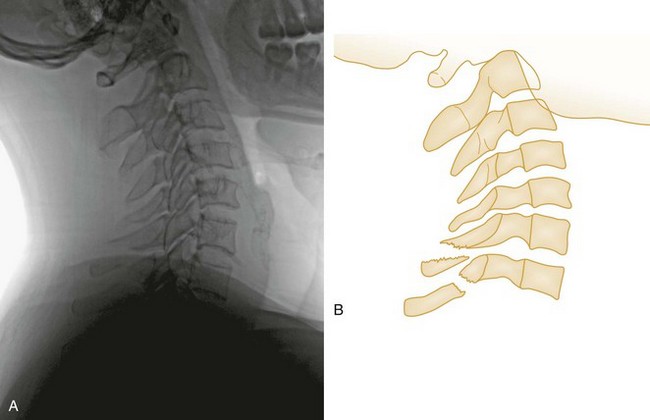
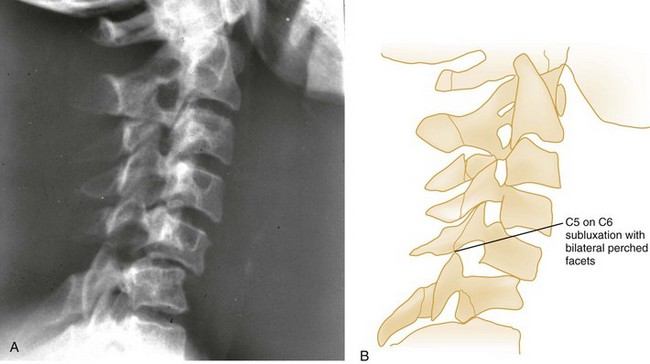
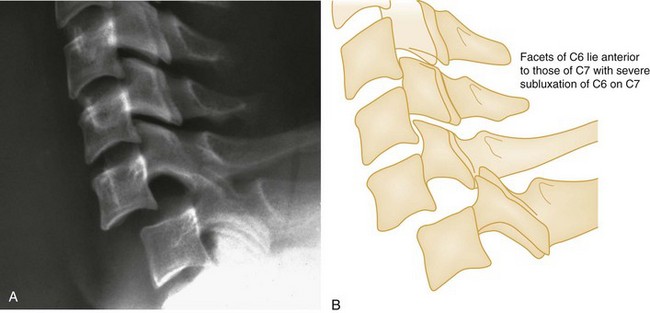
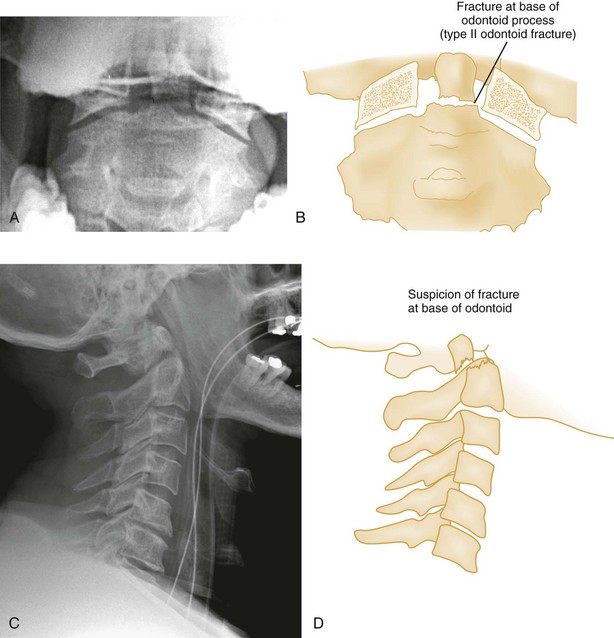
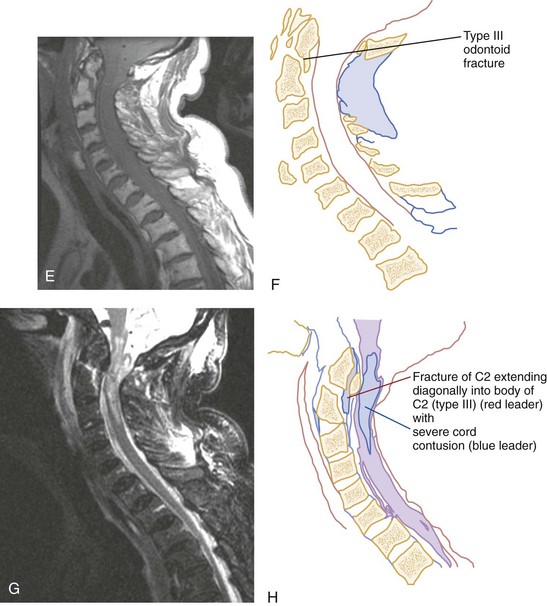
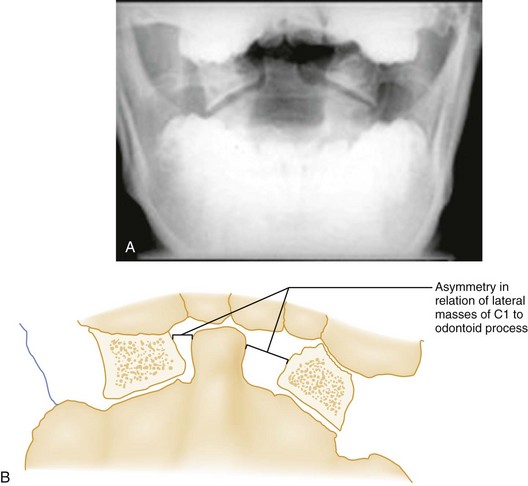
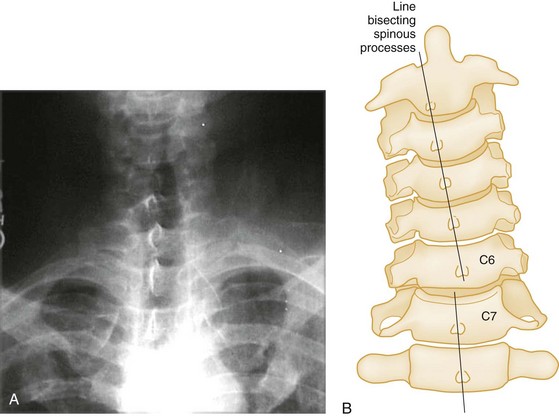
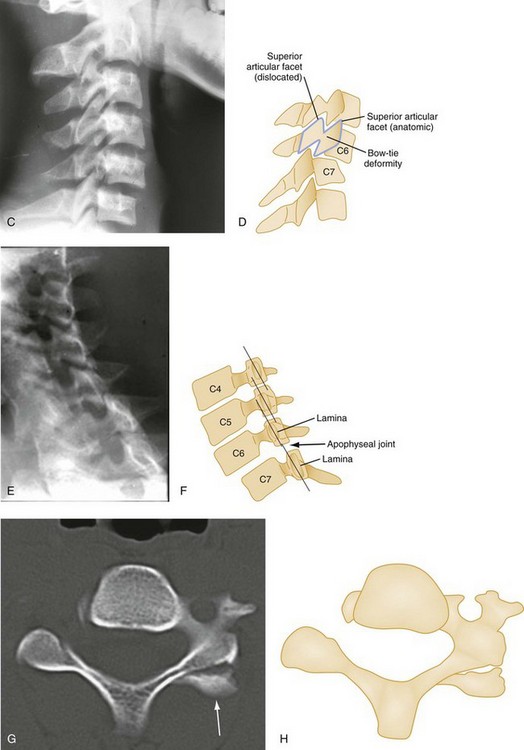
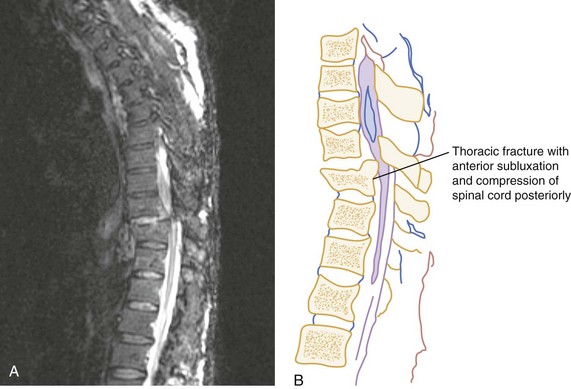
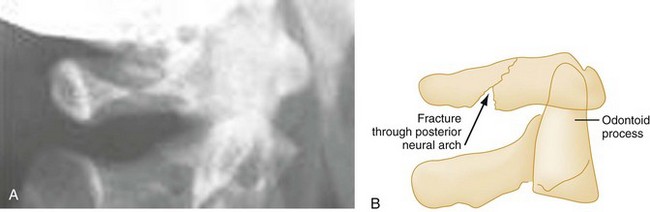
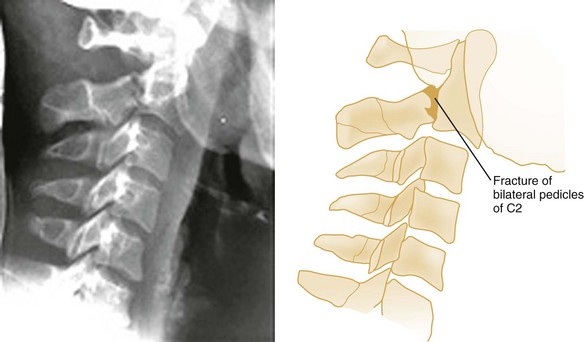
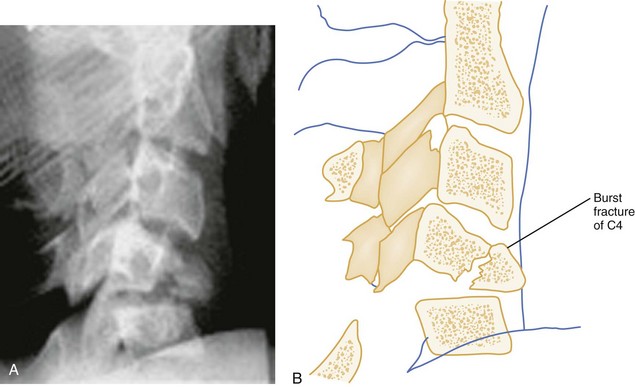
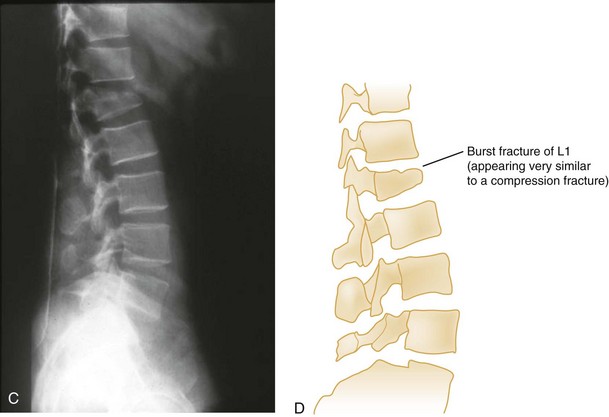
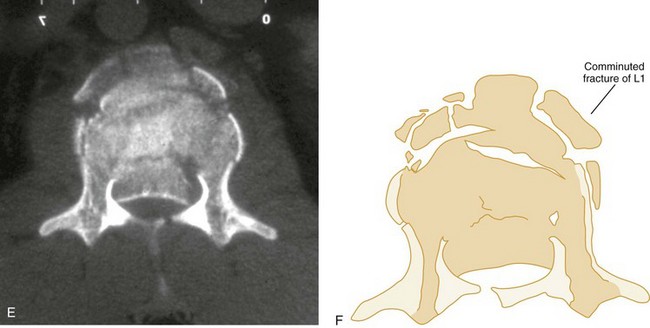
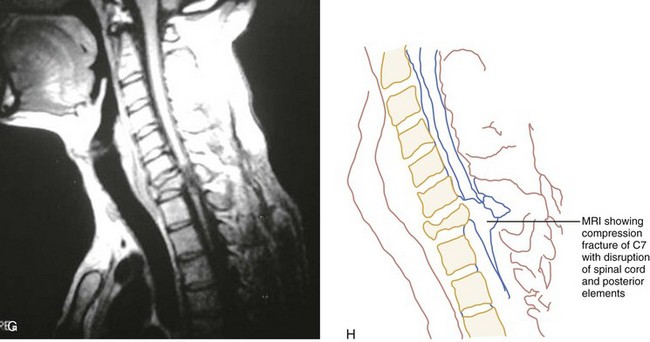
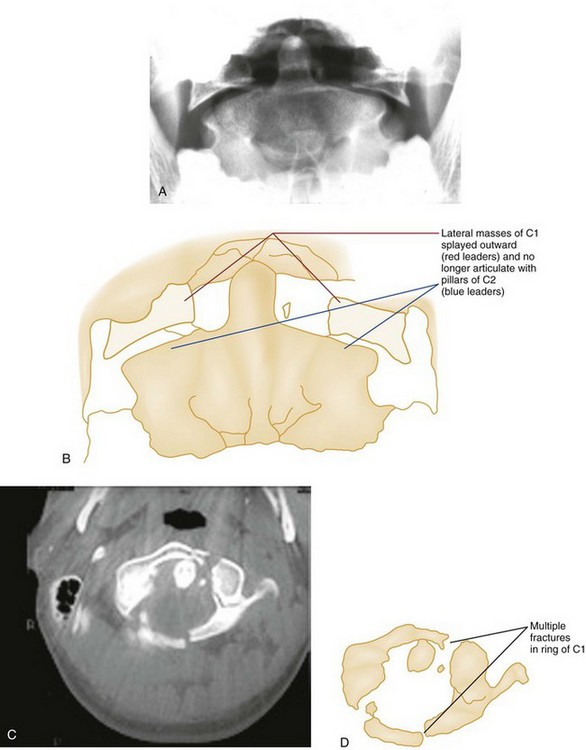
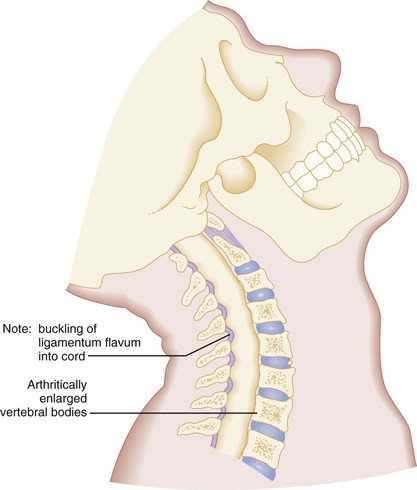
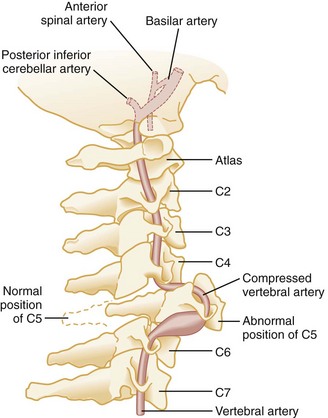
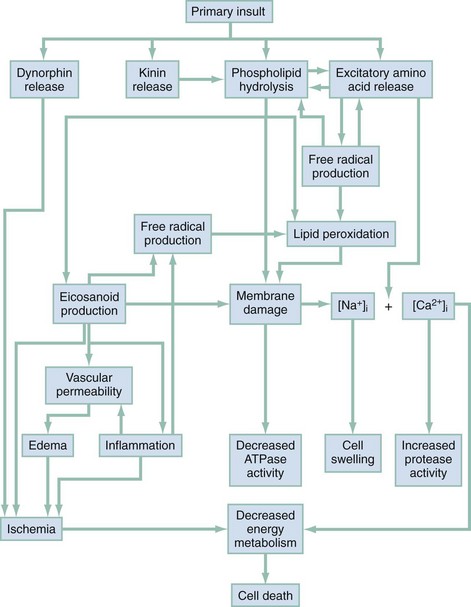
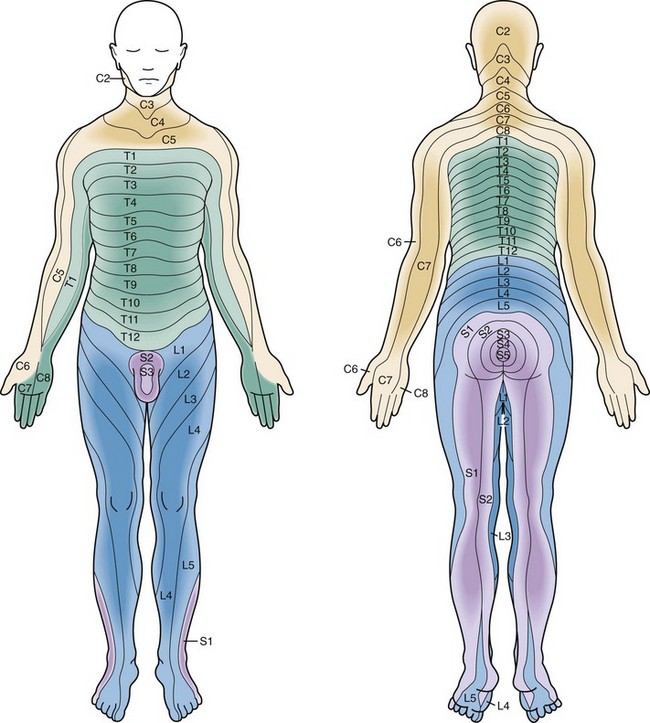
Chapter 43 Statistics from the National Spinal Cord Injury Database show that motor vehicle collisions (MVCs) account for roughly 40% of all spinal injuries.1 Speeding, alcohol intoxication, and failure to use restraints are major risk factors. The next most common cause of spinal cord injury (SCI) is falls, followed by acts of violence (primarily gunshot wounds) and sporting activities. There are currently more than 260,000 spinal injury victims living in the United States, and 12,000 new cases occur each year. Approximately 80% of victims are male, and the average age at injury is 40 years. The lifetime cost to care for SCI victims ranges from $500,000 for people older than 50 years with incomplete motor function to over $3 million for people younger than 25 years with complete paraplegia. The total cost to society from lifelong medical expenses and lost productivity for all age groups and types of spinal injuries is estimated to be more than $5 billion.2 The devastating emotional and psychological impact on the victims and their families is incalculable. The human spine consists of 33 bony vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral (fused into one), and 4 coccygeal (usually fused into one) (Fig. 43-1).3 These 26 individual units are separated from one another by flexible intervertebral disks and connected to form a single functioning unit by a complex network of ligaments. In addition to providing basic structural support, the vertebral column protects the spinal cord, which extends from the midbrain to the level of the second lumbar vertebra. Nerves that receive and transmit sensory, motor, and autonomic impulses pass to and from the spinal cord through intervertebral foramina. Spinal injuries involve fractures in 85% of cases. Ten percent are purely ligamentous injuries, and 5% are SCI without radiographic abnormality (SCIWORA) in which the spinal cord is injured directly without any radiographic evidence of bony or ligamentous injury.4 Stability of a spinal injury refers to the resistance to displacement of fracture fragments or, in the case of ligamentous injury, the entire vertebral unit. Displacement may occur at the time of injury or progressively over hours to weeks and can cause or worsen damage to the spinal cord or nerve roots. There are several conceptual models for assessing the stability of subaxial spinal column injuries, but the most commonly used one is the three parallel vertical column model proposed by Denis (Fig. 43-2)5 The anterior column is formed by alternating vertebral bodies and intervertebral disks surrounded by the annulus fibrosus capsule and the anterior longitudinal ligament. The middle column consists of the posterior part of the annulus fibrosus and posterior vertebral wall, the posterior longitudinal ligament, the spinal cord, the paired laminae and pedicles, the articulating facets, the transverse processes, and the nerve roots and vertebral arteries and veins. The posterior column consists of the spinous processes, nuchal ligament, interspinous and supraspinous ligaments, and ligamentum flavum. Disruption of only a single column usually preserves a high degree of stability but does not preclude SCI from displaced fracture fragments. Disruption of two columns results in an injury that is stable in one direction but unstable in another (e.g., stable in flexion but unstable in extension). Disruption of all three columns produces a highly unstable injury. Until the full extent of the injury is clear, all spinal injuries should be treated as potentially unstable, and spinal immobilization should be maintained. Classification of Spinal Column Injuries Acute spinal injuries are classified according to the mechanism of trauma: flexion, flexion-rotation, extension, and vertical compression (Table 43-1).6,7 Table 43-1 Classification of Spinal Injuries Flexion.: Pure flexion injuries involving the C1-C2 complex can cause unstable atlanto-occipital or atlantoaxial joint dislocation, with or without an associated fracture of the odontoid (Fig. 43-3). These injuries are considered unstable because of their location and the relative lack of muscle and ligamentous support. In pure flexion injuries below C2, a longitudinal pull is exerted on the strong nuchal ligament complex, which usually remains intact. Most of the force is expended on the vertebral body anteriorly, causing a simple wedge fracture. Radiographically, there is a diminished height and increased concavity of the anterior border of the vertebral body, an increased density of the vertebral body resulting from bony impaction, and prevertebral soft tissue swelling (Fig. 43-4). Because the posterior column remains intact, this injury is usually stable and rarely accompanied by nervous system damage. However, spinal instability may occur with severe wedge fractures (loss of more than half the vertebral height) or multiple adjacent wedge fractures, and such injuries are best treated as being potentially unstable. A flexion teardrop fracture results when severe flexion forces cause anterior displacement of a wedge-shaped fragment (resembling a teardrop) of the anteroinferior portion of the involved vertebral body (Fig. 43-5). Because this injury commonly involves anterior and posterior ligamentous disruption, it is often associated with neurologic injury and is highly unstable. The clay shoveler‘s fracture is an oblique fracture of the base of the spinous process of one of the lower cervical segments (Fig. 43-6). The injury derives its name from its common occurrence in clay miners in Australia during the 1930s. When a miner lifted a heavy shovelful of clay, abrupt head flexion against the supraspinous ligament resulted in an avulsion fracture of the spinous process. Today, this fracture is more commonly seen after direct trauma to the spinous process and after sudden deceleration MVCs that result in forced neck flexion. Because this injury involves only the spinous process, it is stable and not associated with neurologic involvement. Pure spinal subluxation occurs when the ligamentous complexes rupture without an associated bony injury. This injury begins posteriorly in the nuchal ligament and proceeds anteriorly to involve other ligaments. The lateral radiograph with the neck in the neutral position may show a widening of both interspinous and intervertebral spaces posteriorly at the level of injury, and oblique views may demonstrate a widening or abnormal alignment of the facets (Fig. 43-7). These findings are often subtle and may be missed if flexion and extension views are not obtained. Although rarely associated with neurologic damage, this injury is potentially unstable. Bilateral facet dislocations occur when a greater force of flexion causes soft tissue disruption to continue anteriorly to the annulus fibrosis of the intervertebral disk and the anterior longitudinal ligament, resulting in an extremely unstable condition. The forward movement of the spine causes the inferior articulating facets of the upper vertebra to pass upward and over the superior facets of the lower vertebra, resulting in anterior displacement of the spine above the level of injury. Radiographically, the anterior displacement will appear to be greater than one half of the anteroposterior (AP) diameter of the lower vertebral body with the superior facets anterior to the inferior facets (Fig. 43-8). Shear Injury.: Trauma to the head directed in an AP direction may result in fracture of the odontoid process above the transverse ligaments (type I) or, more commonly, at the base of the odontoid process where it attaches to C2 (type II) (Fig. 43-9). Slight angulation of the force may result in extension of the fracture into the body of C2 (type III). Type I odontoid fractures are usually stable because they are an avulsion injury to the odontoid tip. However, if traction forces injure the apical and alar ligaments, then the fracture may become unstable. Type II odontoid fractures are unstable and often complicated by nonunion. SCI is uncommon but can occur. Type III odontoid fractures are also mechanically unstable as they can extend laterally into the superior articular facet of the atlas. Flexion-Rotation.: Rotary atlantoaxial dislocation is an unstable injury visualized best on open-mouth odontoid radiographs (Fig. 43-10). If the skull is shown obliquely, there may be a false-positive asymmetry between the odontoid process and the lateral masses of C1. However, when the x-ray film reveals symmetrical basilar skull structures, a unilaterally magnified lateral mass confirms a C1-C2 dislocation. A unilateral facet dislocation involves both flexion and rotation. The rotational component of this injury occurs around one of the facet joints, which acts as a fulcrum. Simultaneous flexion and rotation cause the contralateral facet joint to dislocate, with the superior facet riding forward and over the tip of the inferior facet and coming to rest within the intervertebral foramen. In this position, the dislocated articular mass is mechanically locked in place, making this a stable injury, although the posterior ligament complex is disrupted. The frontal radiograph shows the spinous processes above the level of dislocation displaced from the midline in the direction of the rotation (Fig. 43-11A and B). The lateral radiograph shows a forward displacement of the dislocated segment on the vertebra below (less than one half the AP diameter of this vertebral body) and a rotation of the dislocated vertebra and those above it (Fig. 43-11C and D). Any cervical fracture or dislocation may cause torticollis, but torticollis may also be caused by a benign process such as a muscle spasm. It may be difficult to differentiate torticollis caused by cervical fracture or dislocation from torticollis caused by severe muscle spasm, however, and oblique projections may be necessary to demonstrate the dislocated facet joint (Fig. 43-11E and F). Owing to the varying shapes of the articular processes, particularly between the cervical and lumbar regions, different types of flexion-rotation injuries result. In the cervical region, where articular processes are small, flat, and almost horizontal, unilateral facet dislocations occur as described previously. In the lumbar region, however, where articular processes are large, curved, and nearly vertical, unilateral facet dislocation is rare. Instead, one or both articular processes fracture, and the upper vertebra swings forward. Commonly seen in the thoracolumbar and lumbar region, this rotation fracture-dislocation is unstable (Fig. 43-12). Extension.: The posterior neural arch fracture of the atlas (C1) results from the compression of the posterior elements between the occiput and the spinous process of the axis (C2) during forced neck extension (Fig. 43-13). Although the anterior arch and the transverse ligament remain intact, this fracture is potentially unstable because of its location. The hangman‘s fracture, or traumatic spondylolysis of C2, occurs when the cervicocranium (the skull, atlas, and axis functioning as a unit) is thrown into extreme hyperextension as a result of abrupt deceleration. Bilateral fractures of the pedicles of the axis occur with or without dislocation (Fig. 43-14). Although this lesion is unstable, cord damage is often minimal because the AP diameter of the neural canal is greatest at the C2 level, and the bilateral pedicular fractures permit the spinal canal to decompress itself. Originally described in victims of hanging injury, today it is most often the result of head-on MVCs. The extension teardrop fracture occurs when abrupt extension of the neck causes the anterior longitudinal ligament to pull the anteroinferior corner of a vertebral body away from the remainder of the vertebra, producing a triangular fracture that is radiographically similar to the flexion teardrop fracture. Often occurring in lower cervical vertebrae (C5-C7) from diving accidents, this injury may be associated with a central cord syndrome, which is discussed later, and is caused by the ligamentum flavum buckling into the spinal cord.8 Because the posterior elements remain intact, this injury is stable in flexion but potentially unstable in extension. Vertical Compression.: Vertical compression injuries occur in the cervical and lumbar regions, which are capable of straightening at the time of impact. When forces are applied from either above (skull) or below (pelvis or feet), one or more vertebral body endplates may fracture. The nucleus pulposus of the intervertebral disk is forced into the vertebral body, which is shattered outward, resulting in a burst fracture (Fig. 43-15). The lateral radiograph shows a comminuted vertebral body, and there will typically be greater than 40% compression of the anterior vertebral body, which helps differentiate it from the simple wedge fracture. The frontal radiograph demonstrates a characteristic vertical fracture of the vertebral body, which will also help differentiate it from the simple wedge fracture and the flexion teardrop fracture. This is a stable fracture because all the ligaments remain intact. However, fracture fragments may impinge on or penetrate the ventral surface of the spinal cord and cause an anterior cord syndrome (see Fig. 43-15). The Jefferson fracture of C1 is an extremely unstable injury that occurs when a vertical compression force is transmitted through the occipital condyles to the superior articular surfaces of the lateral masses of the atlas. This force drives the lateral masses outward, resulting in fractures of the anterior and posterior arches of the atlas and a disruption of the transverse ligament. Because this injury is often associated with prevertebral hemorrhage and retropharyngeal swelling, the lateral film may demonstrate a widening of the predental space between the anterior arch of C1 and the odontoid, or dens. The open-mouth view will demonstrate a bilateral offset of both right and left lateral masses of C1 relative to the lateral masses of C2. A fracture should be diagnosed when the sum of the offset distances from the right and left sides exceeds 7 mm (Fig. 43-16). However, when the fragments are minimally displaced, the Jefferson fracture is difficult to recognize, and computed tomography (CT) may be necessary. Primary Spinal Cord Injury.: The spinal cord may be injured in a number of ways.8 First, penetrating trauma or massive blunt trauma with disruption of the vertebral column may cause the transection of neural elements. Because neurons within the central nervous system do not regenerate, such injuries are irreversible. Less severe blunt trauma may have similar effects resulting from a displaced bony fragment or a herniated disk. Second, when elderly patients with cervical osteoarthritis and spondylosis are subjected to forcible cervical spine extension, the spinal cord may be compressed between an arthritically enlarged anterior vertebral ridge and a posteriorly located hypertrophic ligamentum flavum (Fig. 43-17). This injury frequently results in a central cord syndrome. Primary vascular damage to the spinal cord, a third mechanism of injury, may occur in several ways. The spinal cord may be compressed by an extradural hematoma, particularly in patients who are on anticoagulants or have bleeding disorders. Vascular injuries should also be suspected when there is a discrepancy between the clinically apparent neurologic deficit and the known level of spinal injury. For example, a lower cervical dislocation may compress the vertebral arteries as they travel within the spinal foramina of the vertebrae. This compression may result in thrombosis and decreased blood flow through the anterior spinal artery that originates from both vertebral arteries at the level of C1 (Fig. 43-18). On physical examination, such an injury may erroneously appear to be localized to the level of C1 or C2. Also, the great radicular artery of Adamkiewicz, originating from the aorta and entering the spinal canal at the level of L1, sends branches as cephalad as T4. Therefore a lumbar fracture or dislocation can produce a neurologic deficit as high as T4. Secondary Spinal Cord Injury.: The maximum neurologic deficit after blunt spinal cord trauma is often not seen immediately and may instead progress over many hours. The histopathology of the so-called “secondary SCI” has been studied extensively in experimental animal models.9–11 It is now thought that primary SCI initiates a complex cascade of biochemical events that result in progressive ischemia of gray and white matter during the postinjury period (Fig. 43-19). Other factors, such as hypoxia, hypotension, hyperthermia, hypoglycemia, and mishandling by medical personnel, also affect the ultimate extent of SCI. The initial neurologic evaluation of a patient with a suspected spinal injury should begin with simple observation. Careful inspection, beginning with the head and proceeding downward, may reveal signs of possible spinal involvement. Significant head and facial trauma have a 5 to 10% incidence of associated cervical spine injuries.12,13 Scapular contusions suggest a rotation or flexion-rotation injury of the thoracic spine. Chest and neck abrasions from automobile shoulder belts and lower abdominal markings from lap belts indicate possible blunt carotid and vertebral injuries, as well as spinal, intrathoracic, and intra-abdominal injuries. As occurs with falls from considerable heights, injuries to the gluteal region, calcaneal fractures, and severe ankle fractures suggest a compression type of spinal injury. The patient should be observed for the presence and symmetry of both voluntary and involuntary movements. Because the diaphragm is innervated by the phrenic nerve, which originates at C3-C4, an abnormal, abdominal breathing pattern may provide an important clue to a cervical injury. The presence of Horner’s syndrome, characterized by unilateral ptosis, miosis, and anhidrosis, may result from disruption of the cervical sympathetic chain, usually between C7 and T2.5 Priapism may occur with severe SCI, and it is often associated with spinal shock, which is a transient reflex depression of the spinal cord below the level of the injury. The motor activity of the body is complex. Because a single motion is often governed by muscles innervated by multiple spinal segments, localizing a spinal lesion based solely on an assessment of motor function is extremely difficult. Testing the presence and strength of those motions outlined in Table 43-2, however, provides a rapid baseline assessment. When a deficit is noted, the motor and neurologic examination should be repeated at frequent intervals because progression of dysfunction may occur. If there is apparent total loss of function, every effort should be made to elicit the most minimal of motor responses because any response markedly improves the prognosis. A slight toe flicker in an otherwise paralyzed individual indicates that the patient may again eventually walk unassisted. Table 43-2 *Localization of lesions in this area is best accomplished with the sensory examination. The presence of cord-mediated deep tendon reflexes can be helpful as a localizing, diagnostic aid (Table 43-3). Classically, muscle paralysis associated with intact deep tendon reflexes indicates an upper motor neuron (spinal cord) lesion, whereas paralysis associated with absent deep tendon reflexes indicates a lower motor neuron (nerve root or cauda equina) lesion. This differentiation is important because the latter condition is often caused by a surgically correctable lesion. After the initial period of areflexia, reflexes gradually return after 1 to 3 days, and after 1 to 4 weeks, patients with SCI will manifest characteristic hyper-reflexia and spasticity.14 Because reflexes are typically absent during the initial phase of spinal shock, the examination of reflexes is less useful in the emergency department. Table 43-3 Sensory function can be quickly evaluated through use of a structured approach (Table 43-4) or a graphic sensory dermatome chart (Fig. 43-20). After locating an area of hypesthesia, one should move the sensory stimulus from areas of decreased sensation outward, rather than the reverse, because patients are more sensitive to the appearance of sensation than to its disappearance. This test should be performed first with a cotton wisp to assess sensitivity to light touch, a posterior column function. A pin should be used to assess pain sensation, which is an anterior spinothalamic tract function. The presence of islands of preserved sensation within an affected dermatome or below the level of apparent total dysfunction, even in the presence of complete motor paralysis, indicates potential for functional motor recovery.15 An accurate baseline sensory examination is imperative because a cephalad progression of hypesthesia is the most sensitive indicator of deterioration. When this is observed in the cervical region, one should anticipate impending respiratory failure and stabilize the airway. Table 43-4 A complete spinal cord lesion is defined as total loss of motor power and sensation distal to the site of an SCI. Functional motor recovery is rare in a patient with a complete cord syndrome that persists for longer than 24 hours after the injury.7 Before diagnosis of a complete cord syndrome, however, two points should be considered. First, any evidence of minimal cord function, such as sacral sparing, excludes the patient from this group. Signs of sacral sparing include perianal sensation, normal rectal sphincter tone, or flexor toe movement. The presence of any of these signs indicates a partial lesion, usually a central cord syndrome, and the patient may have marked functional recovery, including bowel and bladder control and eventual ambulation. Second, it is important to note that a complete spinal cord lesion may be mimicked by a condition known as spinal shock, which may persist from a few days to a few weeks. Spinal shock results from a concussive injury to the spinal cord that causes total neurologic dysfunction distal to the site of injury.16 The end of spinal shock is heralded by the return of the bulbocavernosus reflex, which is a normal cord-mediated reflex elicited by placing a gloved finger in the patient’s rectum and then squeezing the glans penis or clitoris or by tugging gently on the Foley catheter. An intact reflex results in rectal sphincter contraction. Absence of this reflex indicates the presence of spinal shock, during which time the patient’s prognosis cannot be accurately assessed. A complete spinal cord lesion will remain unchanged after the cessation of spinal shock.
Spinal Injuries
Perspective
Epidemiology
Principles of Disease
Pathophysiology
MECHANISM OF SPINAL INJURY
STABILITY
Flexion
Wedge fracture
Stable
Flexion teardrop fracture
Extremely unstable
Clay shoveler’s fracture
Stable
Subluxation
Potentially unstable
Bilateral facet dislocation
Always unstable
Atlanto-occipital dislocation
Unstable
Anterior atlantoaxial dislocation with or without fracture
Unstable
Odontoid fracture with lateral displacement fracture
Unstable
Fracture of transverse process
Stable
Flexion-Rotation
Unilateral facet dislocation
Stable
Rotary atlantoaxial dislocation
Unstable
Extension
Posterior neural arch fracture (C1)
Unstable
Hangman’s fracture (C2)
Unstable
Extension teardrop fracture
Usually stable in flexion; unstable in extension
Posterior atlantoaxial dislocation with or without fracture
Unstable
Vertical Compression
Bursting fracture of vertebral body
Stable
Jefferson fracture (C1)
Extremely unstable
Isolated fractures of articular pillar and vertebral body
Stable
Classification of Spinal Cord Injuries
Clinical Features
LEVEL OF LESION
RESULTING LOSS OF FUNCTION
C4
Spontaneous breathing
C5
Shrugging of shoulders
C6
Flexion at elbow
C7
Extension at elbow
C8-T1
Flexion of fingers
T1-T12
Intercostal and abdominal muscles*
L1-L2
Flexion at hip
L3
Adduction at hip
L4
Abduction at hip
L5
Dorsiflexion of foot
S1-S2
Plantar flexion of foot
S2-S4
Rectal sphincter tone
LEVEL OF LESION (AT OR ABOVE)
RESULTING LOSS OF REFLEX
C6
Biceps
C7
Triceps
L4
Patellar
S1
Achilles
LEVEL OF LESION
RESULTING LEVEL OF LOSS OF SENSATION
C2
Occiput
C3
Thyroid cartilage
C4
Suprasternal notch
C5
Below clavicle
C6
Thumb
C7
Index finger
C8
Small finger
T4
Nipple line
T10
Umbilicus
L1
Femoral pulse
L2-L3
Medial aspect of thigh
L4
Knee
L5
Lateral aspect of calf
S1
Lateral aspect of foot
S2-S4
Perianal region
Complete Spinal Cord Lesions





Full access? Get Clinical Tree


